 E-submission
E-submission TOTA
TOTA TOTS
TOTS
Search
- Page Path
- HOME > Search
Original Articles
- Epidemiological changes and surgical trends of distal radius fractures in adults over 50 years during the COVID-19 pandemic in Korea: a nationwide repeated cross-sectional study
- Han-Kook Yoon, So Ra Yoon, Kee-Bum Hong, Youngsu Jung, SeongJu Choi, Jun-Ku Lee
- J Musculoskelet Trauma 2026;39(1):12-19. Published online January 25, 2026
- DOI: https://doi.org/10.12671/jmt.2025.00297

-
 Abstract
Abstract
 PDF
PDF Supplementary Material
Supplementary Material - Background
The COVID-19 pandemic is likely to have affected bone health in older adults in Korea. This study aimed to analyze changes in the epidemiology and management of distal radius fractures (DRFs) in older adults before and during the COVID-19 pandemic.
Methods
Patients with DRF aged over 50 years in 2017, 2018, 2020, and 2021 were included in this study. Patients were classified into a group with DRF occurring between 2017 and 2018 (before COVID-19) and a group with DRF occurring between 2020 and 2021 (during COVID-19). We calculated the incidence rates of DRF and compared them between the two groups. We also analyzed and compared demographic data (age, sex, income, residence) and the operation rate for DRF between the two groups. Patient selection and treatment were based on International Classification of Diseases, 10th revision codes.
Results
A total of 140,634 patients with DRF (before COVID-19, 69,794; during COVID-19, 70,840) were included. The incidence of DRF before COVID-19 (184.4/100,000 person-years) was higher than during COVID-19 (169.8/100,000 person-years). The operation rate was higher during COVID-19 (86.9%) than before COVID-19 (83.3%).
Conclusion
During the COVID-19 pandemic, the incidence of DRF decreased in South Korea. However, the rate of surgical treatment increased and exceeded the global surgical rate. Level of evidence: III.
- 214 View
- 6 Download

- Computed tomography plane reformatting to reduce projection error in measuring Pauwels angle of femoral neck fractures: a cross-sectional study
- Gyu Min Kong, Jae-Young Lim, Se-Lin Jeong, Gu-Hee Jung
- J Musculoskelet Trauma 2026;39(1):38-47. Published online January 25, 2026
- DOI: https://doi.org/10.12671/jmt.2025.00038

-
Abstract
PDF
- Objectives
This study aimed to assess fracture verticality in both coronal and axial planes after eliminating projection error in femoral neck fractures among non-older adults, and to demonstrate its clinical utility using computed tomography (CT)-based modeling at actual size.
Methods
This retrospective observational study enrolled 57 patients (30 males and 27 females), aged 20–65 years, with displaced femoral neck fractures. Based on CT images, an actual-size fracture model was constructed. The CT scanning plane was reformatted with the neck-shaft fragment realigned vertically to the ground and parallel to the femoral neck axis. Three consecutive images were used to generate coronal reformats at the centerline and posterior border to measure central and posterior coronal plane verticality as Pauwels’ angle (PA). The central image of the reformatted axial plane was used to assess axial plane verticality. Differences in verticality were analyzed using analysis of variance.
Results
Three coronal morphology types were identified: linear (n=30), concave (n=25), and convex (n=2). Two axial morphology types were observed: cephalad (n=35) and trochanteric (n=22). The mean central PA, posterior PA, and axial verticality were 55.43°±13.79°, 51.44°±11.13°, and 85.74°±18.41°, respectively. Only the central PA showed a significant difference (P<0.001). The PA was significantly higher in the linear coronal type between images (P<0.05) and in the trochanteric axial type (P<0.05).
Conclusions
After reformatting the scanning plane, the central PA showed significant variation between images. Femoral neck fractures of the linear type in the coronal plane and the trochanteric type in the axial plane demonstrated greater verticality than other morphological types. Level of evidence:
- 147 View
- 4 Download
- Surgical outcomes of the coracoid process fracture associated with the acromioclavicular joint injury in Korea: a case series
- Dongju Shin, Sung Choi, Sangwoo Kim, Byung Hoon Kwack
- J Musculoskelet Trauma 2026;39(1):54-61. Published online January 14, 2026
- DOI: https://doi.org/10.12671/jmt.2025.00346
-
Abstract
PDF
- Background
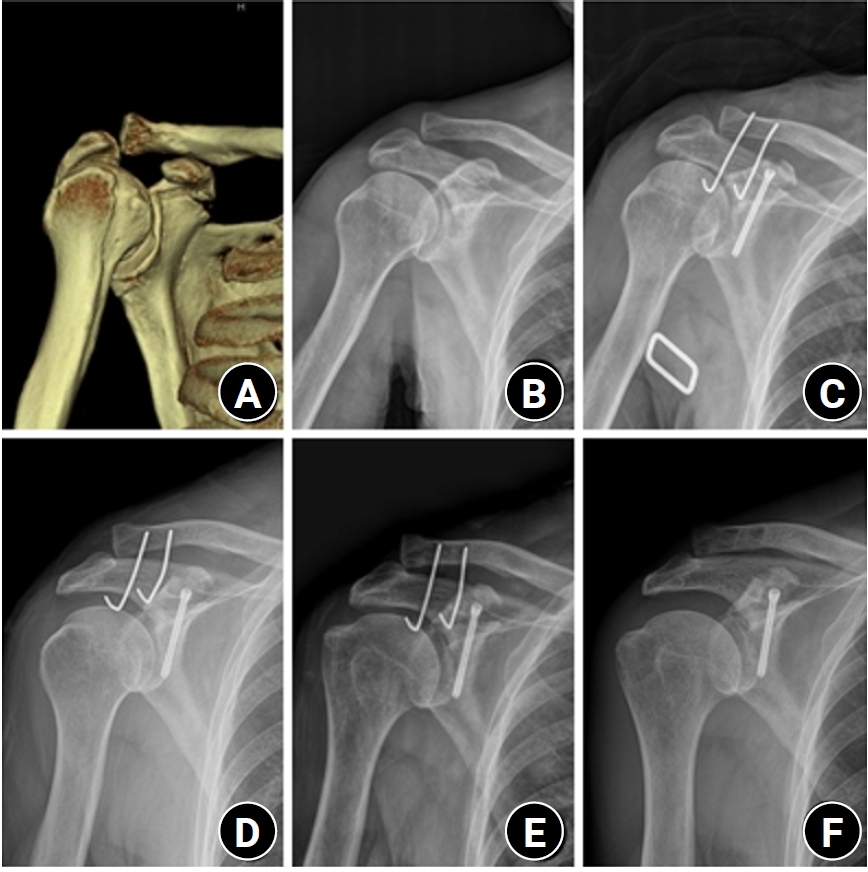
Excluding technical reports and isolated case reports, there are no published studies evaluating coracoid process fixation with or without an acromioclavicular joint (ACJ) stabilization procedure for coracoid process fractures associated with ACJ injury. The purpose of this study was to assess the surgical outcomes of coracoid process fractures associated with ACJ injuries and to determine the usefulness of coracoid process fixation with or without an ACJ stabilization procedure.
Methods
From February 2006 to December 2015, patients with coracoid process fractures associated with ACJ injuries were enrolled. Radiological and clinical outcomes were analyzed in 12 patients who underwent coracoid process fixation with or without an ACJ stabilization procedure. A 3.5-mm cannulated screw with a washer or a 3.0-mm headless compression screw was used for coracoid process fixation, and either a clavicle hook plate or Kirschner (K)-wires were used for ACJ injuries when additional fixation was necessary.
Results
Bone union was achieved in 11 patients (91.7%), while one case was determined to be a nonunion at 6 months. Radiological union occurred at an average of 3 months (range, 1.5–4 months) in all patients except the nonunion case. At the final follow-up, the average clinical scores were a visual analogue scale (VAS) pain score of 1.5 (range, 0–4) and a UCLA score of 30.9 (range, 28–35). Clinical outcomes were satisfactory in all patients, including the patient with nonunion.
Conclusion
The clinical and radiological outcomes of treating coracoid process fractures associated with ACJ injuries using coracoid process fixation with or without ACJ stabilization were favorable. A cannulated screw with a washer and clavicle hook plate fixation may provide sufficient stability for both the coracoid process fracture and the ACJ injury when feasible. Level of evidence: IV.
- 182 View
- 6 Download
- Hook plate versus periarticular-type volar locking plate for distal radius fractures involving the volar lunate facet in Korea: a retrospective cohort study
- Hyun-Jae Park, Joo-Hak Kim
- J Musculoskelet Trauma 2025;38(4):221-228. Published online October 24, 2025
- DOI: https://doi.org/10.12671/jmt.2025.00241
-
Abstract
PDF
- Background
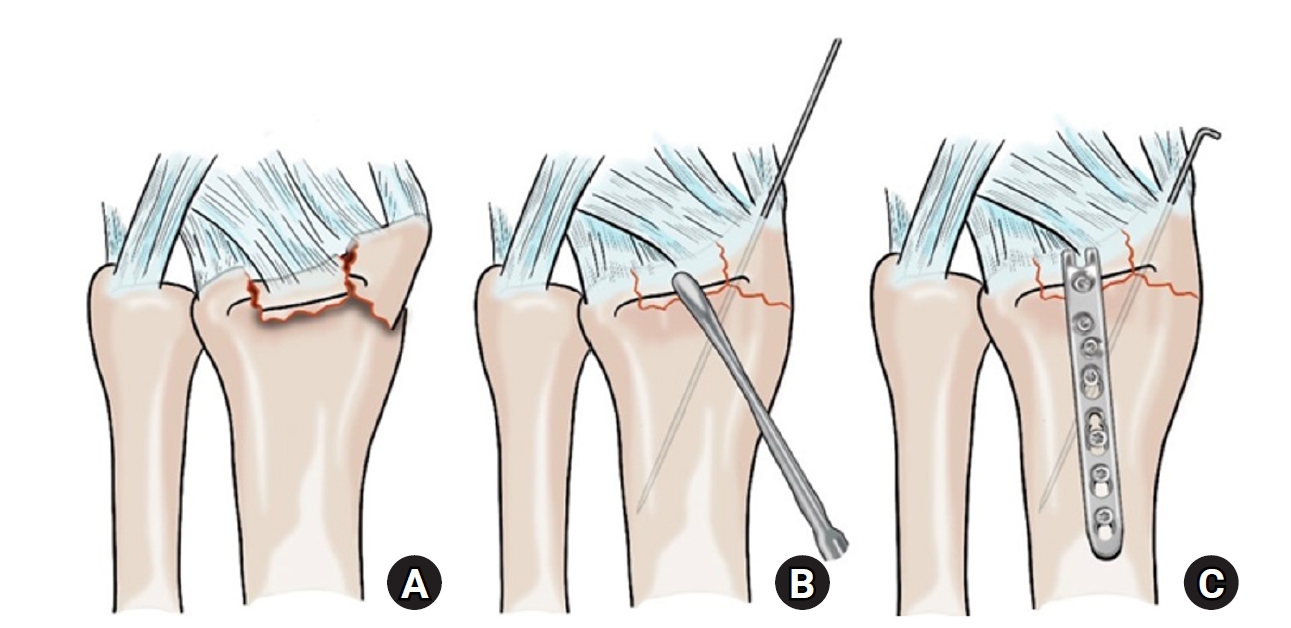
This study investigated the clinical and radiographic outcomes of hook plate (HP) fixation for volar lunate facet fractures, comparing them with periarticular-type volar locking plates (PVLPs).
Methods
A retrospective review was conducted on 24 patients with distal radius fractures involving volar lunate facet fragments who underwent surgery between January 2016 and April 2021. Patients were divided into two groups: HP (n=12) and PVLP (n=12). Radiographic union, wrist range of motion, Disabilities of the Arm, Shoulder and Hand (DASH) scores, and implant-related complications were compared. Statistical analyses included the Mann-Whitney U test and Fisher exact test.
Results
Radiographic union was achieved in all patients (100%), without secondary displacement or hardware failure. No significant differences were observed between the two groups in wrist flexion (P=0.152), extension (P=0.832), pronation (P=0.792), or supination (P=0.328). The mean DASH scores were 12.8±5.5 in the HP group and 14.6±6.0 in the volar plate group (P=0.449). One patient in the HP group experienced mild flexor tendinopathy that resolved with conservative management. No cases of tendon rupture or early reoperation were reported.
Conclusions
Fixation of volar lunate facet fractures using a HP yielded clinical and radiographic outcomes comparable to those of PVLPs, with a low rate of complications and reliable bony union. Due to its mechanical stability, compatibility with standard surgical approaches, and low risk of flexor tendon irritation, the HP may serve as a valuable alternative for managing volar lunate facet fractures. Level of evidence: IV.
- 382 View
- 11 Download
- Relationship of lateral malleolar fracture patterns to posterior malleolar fracture morphology in supination-external rotation ankle fractures in Korea: a retrospective cohort stduy
- Jong-Eun Kim, Chan-Jin Park, Jun-Young Lee, Keun-Bae Lee, Gun-Woo Lee
- J Musculoskelet Trauma 2025;38(4):212-220. Published online October 24, 2025
- DOI: https://doi.org/10.12671/jmt.2025.00234
-
Abstract
PDF
- Background
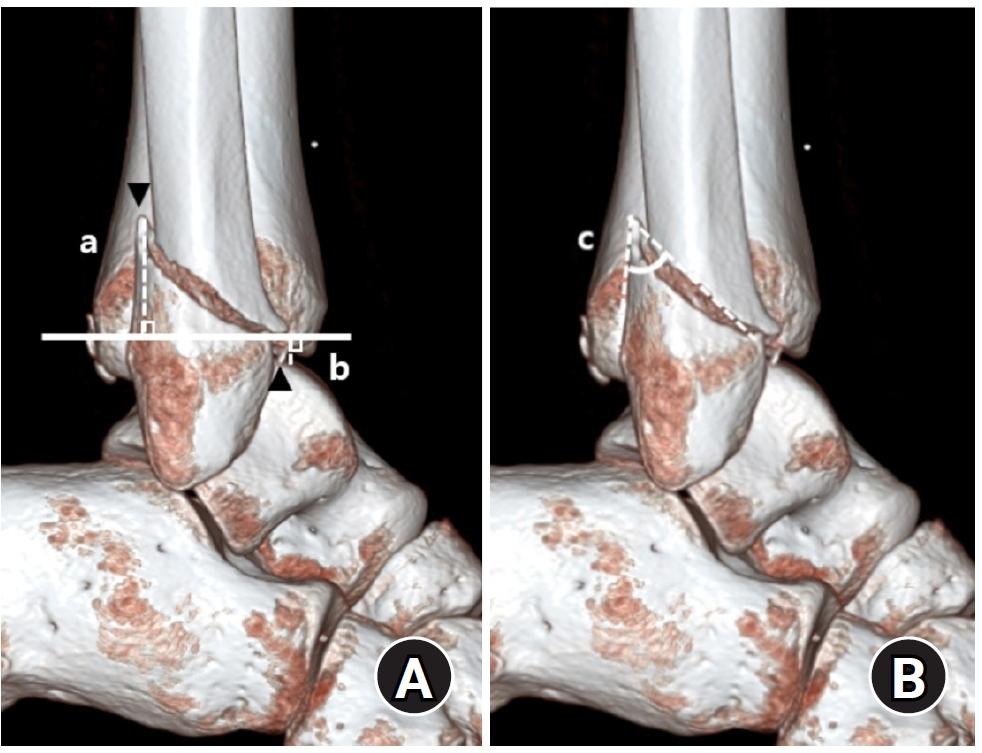
Posterior malleolar fractures frequently accompany rotational ankle fractures. However, the morphological relationship between lateral and posterior malleolar fractures in supination-external rotation (SER) ankle fractures remains unclear. This study aimed to classify lateral malleolar fracture patterns in SER type 3 and 4 ankle fractures and investigated their associations with posterior malleolar fracture morphology.
Methods
We retrospectively reviewed 132 patients with SER type 3 or 4 ankle fractures and concurrent posterior malleolar fractures between January 2016 and December 2021. Lateral malleolar fractures were categorized as fibular fractures extending <4.5 cm proximal to the ankle joint (102 ankles) or fibular fractures extending ≥4.5 cm proximal to the ankle joint (30 ankles) based on posterior cortex height measured using three-dimensional computed tomography (3D-CT). Posterior malleolar fracture morphology was assessed using the Haraguchi and Bartonicek classifications. Quantitative parameters—including fracture height, angle, and articular involvement—were analyzed using 3D-CT imaging.
Results
Fibular fractures extending ≥4.5 cm proximal to the ankle joint were associated with a significantly higher frequency of Haraguchi type II and Bartonicek types 3 and 4 posterior malleolar fractures. This group also exhibited greater articular involvement (19.2% vs. 12.0%) and posterior cortical height (55.4 mm vs. 24.8 mm) compared to the <4.5 cm group (all P<0.001).
Conclusions
In SER type 3 and 4 ankle fractures, a fibular fracture extending ≥4.5 cm proximal to the ankle joint may be associated with posterior malleolar fractures exhibiting greater articular involvement and medial extension. Preoperative evaluation of the lateral malleolar fracture pattern may provide useful insights into posterior malleolar morphology and assist in surgical planning. However, these findings should be interpreted with caution due to inherent study limitations. Level of evidence: IV
- 986 View
- 20 Download
- Computational simulation of coracoclavicular screw insertion through the superior distal clavicular plate for clinical applications in Korean cadavers
- Hyung-Lae Cho, Ji Han Choi, Se-Lin Jeong, Gu-Hee Jung
- J Musculoskelet Trauma 2025;38(3):143-151. Published online July 22, 2025
- DOI: https://doi.org/10.12671/jmt.2025.00122
-
Abstract
PDF
- Background
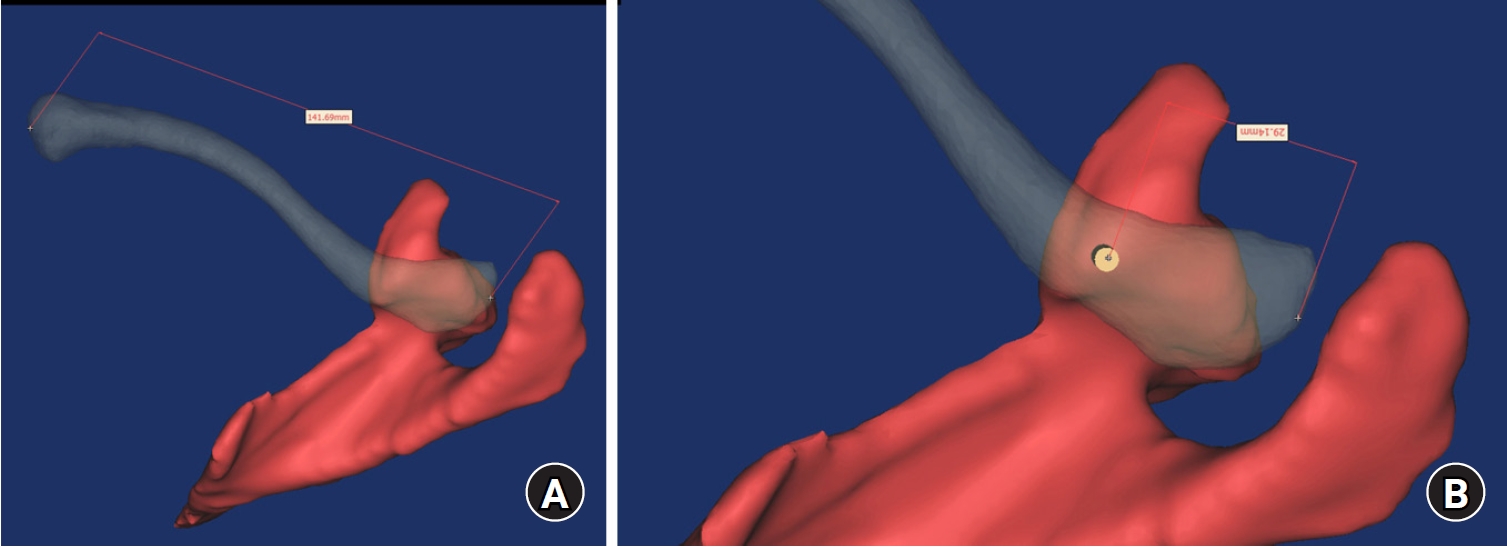
The study was conducted to determine the practical area for inserting the coracoclavicular (CC) screw through the plate by analyzing three-dimensional (3D) shoulder models featuring virtually implanted, actual-size plates and screws.
Methods
Ninety cadaveric shoulders (41 males and 49 females) underwent continuous 1.0-mm slice computed tomography scans. The data were imported into image-processing software to generate a 3D shoulder model, including the scapula and clavicle. The overlapping area between the clavicle and the horizontal portion of the coracoid process (horizontal portion_CP) was analyzed in the cranial view. A curved pelvic recon plate was virtually placed on the upper surface of the distal clavicle, and an actual-size (3.5 mm) CC screw was inserted through the plate.
Results
The distal clavicle directly overlapped with the horizontal portion_CP in the vertical direction. The overlapping area was sufficient to place the 3.5 mm and 4.5 mm-sized screws. In all shoulder models, the CC screw could be inserted through the plate into the vertical direction, with an average length of 35.5 mm (range, 26.2–62.5 mm; standard deviation, 1.2 mm). In 87 models, the CC screw was inserted through the third hole from the lateral end of the plate. Two models were inserted through the second hole, and one model through the fourth hole.
Conclusions
The upper surface of the clavicle has sufficient overlapping area to place CC screws through the plate in the vertical direction in the corresponding hole. Supplemental CC screw fixation through the plate can be performed without additional or special equipment. Level of evidence: IV
- 671 View
- 22 Download
Review Article
- Fracture-related infections: a comprehensive review of diagnosis and prevention
- HoeJeong Chung, Hoon-Sang Sohn
- J Musculoskelet Trauma 2025;38(2):86-95. Published online April 25, 2025
- DOI: https://doi.org/10.12671/jmt.2025.00164
-
Abstract
PDF
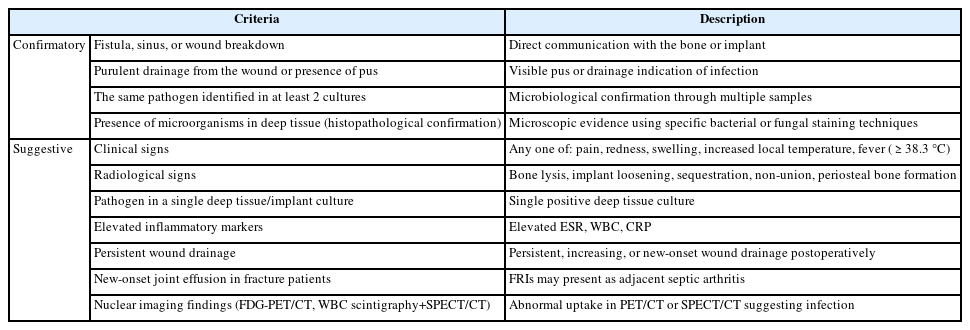
- Fracture-related infections are challenging complications in orthopedic trauma that often require prolonged treatment and impose a significant healthcare burden. Accurate diagnosis and effective prevention strategies are essential for minimizing their occurrence. A recent international consensus has established standardized diagnostic criteria based on clinical, microbiological, radiological, and histopathological findings. Prevention is the top priority and involves a thorough preoperative risk assessment, along with glycemic control, nutritional optimization, and management of comorbidities, as well as intraoperative and postoperative measures such as appropriate antibiotic prophylaxis, surgical site antisepsis, and meticulous wound care. A multidisciplinary approach involving orthopedic surgeons, infectious disease specialists, and microbiologists is crucial for successfully reducing the burden of fracture-related infections.
-
Citations
Citations to this article as recorded by
- Personalized Approaches to Diagnostic and Therapeutic Strategies in Periprosthetic Fracture-Related Infections (PFRIs): Case Series and Literature Review
Marianna Faggiani, Marco Zugnoni, Matteo Olivero, Salvatore Risitano, Giuseppe Malizia, Silvia Scabini, Marcello Capella, Stefano Artiaco, Simone Sanfilippo, Alessandro Massè
Journal of Personalized Medicine.2025; 15(12): 576. CrossRef - Pathogen-Specific Risk for Iterative Surgical Debridement in Orthopedic Infections: A Prospective Multicohort Analysis
Flamur Zendeli, Anna Jędrusik, Raymond O. Schaefer, David Albrecht, Michael Betz, Felix W. A. Waibel, Tanja Gröber, Nathalie Kühne, Sören Könneker, İlker Uçkay
Journal of Clinical Medicine.2025; 14(24): 8750. CrossRef
- Personalized Approaches to Diagnostic and Therapeutic Strategies in Periprosthetic Fracture-Related Infections (PFRIs): Case Series and Literature Review
- 6,757 View
- 274 Download
- 2 Crossref
Original Article
- Reverse V step-cut osteotomy for the correction of cubitus varus in adults: a retrospective study
- Jinyoung Bang, Hyung Jun Koo
- J Musculoskelet Trauma 2025;38(2):102-108. Published online April 25, 2025
- DOI: https://doi.org/10.12671/jmt.2025.00045

-
Abstract
PDF
- Background
Cubitus varus deformity in adults most commonly occurs as a late complication resulting from malunion of distal humeral fractures sustained during childhood. This deformity can cause cosmetic problems and anatomical deformities that hinder normal sports activities and potentially lead to long-term complications. Although various surgical techniques exist for correcting cubitus varus, this study investigated the clinical and functional outcomes of reverse V step-cut osteotomy.
Methods
In total, 15 patients underwent surgical treatment with reverse V step-cut osteotomy between 2012 and 2023. The mean age of the patients at the time of surgery was 46.3 years (range, 20–65 years). The preoperative carrying angle was ‒11.09° of varus, which was corrected to +12.81° of valgus postoperatively. The mean preoperative lateral prominence index (LPI) was ‒10.03, and the mean postoperative LPI improved to ‒4.48. A comparison to the unaffected side showed a P-value of 0.978, indicating similarity.
Results
Preoperatively, eight patients exhibited signs of posterolateral rotatory instability, and among them, three underwent concomitant lateral ulnar collateral ligament reconstruction. Seven patients reported ulnar nerve symptoms, and all underwent concurrent ulnar nerve release. Postoperatively, improvements in elbow pain, instability, and ulnar nerve symptoms were observed. One patient required reoperation due to malunion and insufficient correction, but no other complications were noted.
Conclusions
These outcomes demonstrate that reverse V step-cut osteotomy can be an effective treatment method for cubitus varus deformity in adults. Level of evidence: IV.
- 1,964 View
- 56 Download
Review Articles
- Treatment of avulsion fractures around the knee
- Jeong-Hyun Koh, Hyung Keun Song, Won-Tae Cho, Seungyeob Sakong, Sumin Lim
- J Musculoskelet Trauma 2025;38(2):63-73. Published online March 31, 2025
- DOI: https://doi.org/10.12671/jmt.2025.00073
-
Abstract
PDF
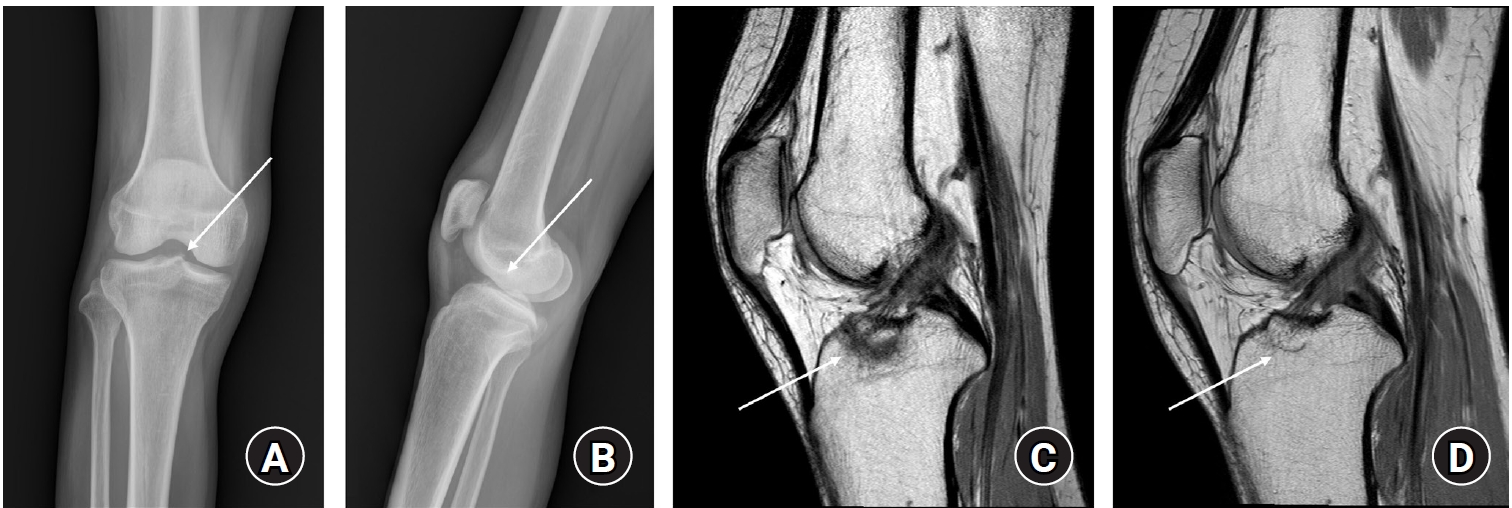
- Avulsion fractures of the knee occur when tensile forces cause a bone fragment to separate at the site of soft tissue attachment. These injuries, which frequently affect adolescent athletes, can involve the cruciate and collateral ligaments, arcuate complex, iliotibial band, and patellar and quadriceps tendons. Radiographs aid in the initial diagnosis, while computed tomography and magnetic resonance imaging facilitate a comprehensive evaluation of injury severity and concomitant damage. Specific avulsion fracture types include: anterior cruciate ligament avulsions (tibial site, Meyers and McKeever classification), posterior cruciate ligament avulsions (tibial attachment, Griffith's classification), Segond fractures (anterolateral complex injury), iliotibial band avulsions, medial collateral ligament avulsions (reverse Segond, Stieda fractures), arcuate complex avulsions ("arcuate sign"), medial patellofemoral avulsions (patellar dislocations), and patellar/quadriceps tendon avulsions. The treatment depends on the fracture location, displacement, and associated injuries. Non-displaced fractures can be managed conservatively, while displaced fractures or those with instability require surgical reduction and fixation. Prompt recognition and appropriate intervention prevent complications such as deformity, nonunion, malunion, and residual instability. This review provides an overview of the pathogenesis, diagnosis, and management of knee avulsion fractures to guide clinical decision-making.
-
Citations
Citations to this article as recorded by- Lateral marginal fractures of the patella and patellofemoral pain
Jae-Ang Sim, Chul-Ho Kim, Ji Wan Kim
Journal of Musculoskeletal Trauma.2025; 38(3): 152. CrossRef
- Lateral marginal fractures of the patella and patellofemoral pain
- 18,961 View
- 205 Download
- 1 Crossref
- Avulsion fractures around the hip joint and pelvis
- Won-Sik Choy, Yonghan Cha, Jung-Taek Kim, Jun-Il Yoo, Jin-Woo Kim
- J Musculoskelet Trauma 2025;38(2):53-62. Published online March 24, 2025
- DOI: https://doi.org/10.12671/jmt.2025.00010
-
Abstract
PDF
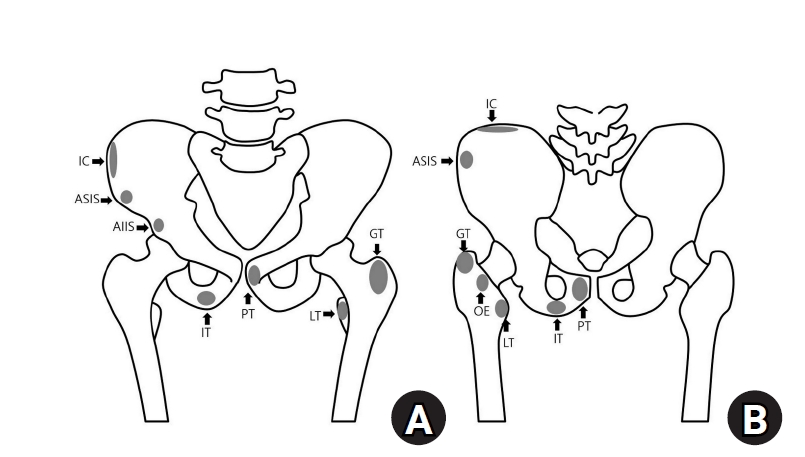
- Avulsion fractures occur when tendons or ligaments are subjected to forces greater than they can withstand at the apophysis or enthesis, regardless of fusion status. The pelvis and hip joint are vulnerable to these injuries due to the diverse muscular structures in these structures, which serve as origins for multiple muscles leading to the lower extremities. Pelvic avulsion fractures commonly affect young athletes, but can also occur in adults. The diagnosis typically involves assessing trauma history, a clinical examination, and radiographic imaging. If the diagnosis is unclear, additional tests such as computed tomography and magnetic resonance imaging may assist in the diagnosis and provide useful information for treatment decisions. While most avulsion fractures respond well to conservative treatment, surgical intervention may be preferred in severe displacements, cases of significant retraction in active athletes, or when a faster recovery is necessary. Chronic or neglected injuries may lead to excessive osseous formation around the pelvis, causing impingement syndromes. Recognizing characteristic radiological findings based on pelvic anatomy helps to make an accurate diagnosis, as chronic injuries can mimic tumors or infectious conditions, necessitating a careful differential diagnosis.
-
Citations
Citations to this article as recorded by- Avulsion Fracture of the Lesser Trochanter and the Use of Conservative Treatment
Dawid Bartosik, Bartlomiej Cwikla, Anna Kowalczyk, Michalina Loson-Kawalec, Anna Palka-Szymaniec, Bartosz Starzynski, Alina Keska, Jakub Szkuta, Klaudia Wojcik
Cureus.2026;[Epub] CrossRef
- Avulsion Fracture of the Lesser Trochanter and the Use of Conservative Treatment
- 9,169 View
- 137 Download
- 1 Crossref
- Easily missed nondisplaced fractures accompanying complete fractures in the lower extremity and pelvis: a narrative review
- Young-Chang Park
- J Musculoskelet Trauma 2025;38(1):5-12. Published online January 24, 2025
- DOI: https://doi.org/10.12671/jmt.2025.00017

-
Abstract
PDF
- Nondisplaced fractures accompanying complete fractures are often difficult to detect on plain radiographs or computed tomography scans, posing a diagnostic challenge. The diagnosis of these frequently overlooked injuries can be delayed, potentially leading to suboptimal patient outcomes. This review discusses four commonly missed fracture patterns in the lower extremity and pelvis, including posterior involvement in fragility fractures of the pelvis, intertrochanteric extensions in isolated greater trochanter fractures, ipsilateral femoral neck fractures in high energy femoral shaft fractures, and posterior malleolar fractures in distal spiral tibial shaft fractures. An accurate diagnosis of these accompanying nondisplaced fractures is critical for optimizing surgical outcomes. Surgeons should incorporate thorough preoperative evaluations into their clinical practice to facilitate early detection and appropriate treatment strategies. Prompt identification and comprehensive management remain essential for improving patient outcomes.
- 1,376 View
- 47 Download
Original Articles
- Interpositional tricortical iliac bone graft in nonunion of midshaft clavicular fractures
- Eun-Seok Son, Bum-Soon Park, Chang-Jin Yon, Chul-Hyun Cho
- J Musculoskelet Trauma 2025;38(1):23-31. Published online January 24, 2025
- DOI: https://doi.org/10.12671/jmt.2025.00004
-
Abstract
PDF
- Background
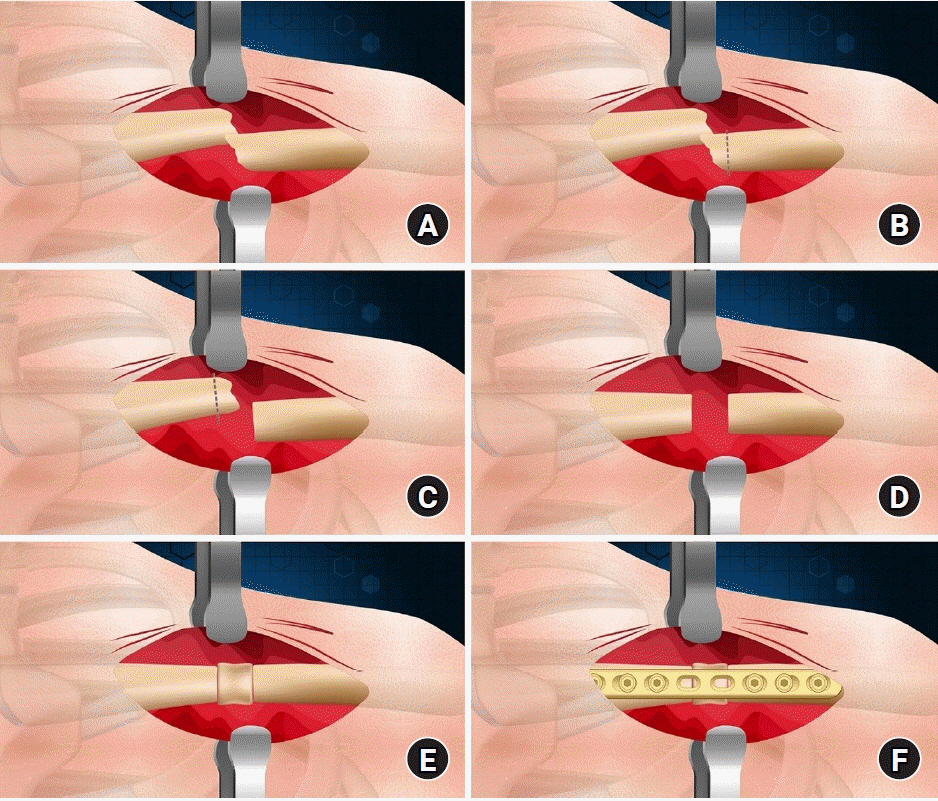
The purpose of this study was to investigate the radiological and clinical outcomes after interpositional tricortical iliac bone graft with plate fixation for the nonunion of clavicle midshaft fractures. Methods: Between 2007 and 2020, 17 cases who were treated by interpositional tricortical iliac bone graft with plate fixation for the clavicle midshaft nonunion combined with bone defect were investigated. The mean age was 53 years (range, 22–70 years). The mean follow-up period was 102.2 months (range, 18–193 months). Serial plain radiographs were used to evaluate radiological outcomes. The University of California, Los Angeles (UCLA) score, American Shoulder and Elbow Surgeons (ASES) score, and Quick-disabilities of the arm, shoulder, and hand (DASH) score were used to evaluate clinical outcomes. Complications were also evaluated. Results: All cases achieved complete bony union with mean healing time of 17.6 weeks (range, 14–22 weeks). The mean clavicle length difference was significantly decreased from 9.1 mm preoperatively to 2.6 mm postoperatively (P<0.001). The mean UCLA and ASES scores were significantly improved from 18.1 and 52.2 before surgery to 30.6 and 88.6 after surgery (both P<0.001), respectively. The mean final Quick-DASH score was 18.0. Three cases (17.6%) developed postoperative complications including two cases of shoulder stiffness and one case of screw irritation. Conclusions: Interpositional tricortical iliac bone graft with plate fixation for the clavicle midshaft nonunion demonstrated excellent radiological and clinical outcomes. In cases of atrophic nonunion combined with bone defect, this technique is an effective option that can provide structural support and restore clavicle length. Level of evidence: Level IV, case series.
- 2,027 View
- 44 Download
- Does the Operator’s Experience Affect the Occurrence of Complications after Distal Radius Fracture Volar Locking Plate Fixation? A Comparative Study of the First Four Years and Thereafter
- Kee-Bum Hong, Chi-Hoon Oh, Chae Kwang Lim, Sungwoo Lee, Soo-Hong Han, Jun-Ku Lee
- J Musculoskelet Trauma 2024;37(4):175-183. Published online October 25, 2024
- DOI: https://doi.org/10.12671/jmt.2024.37.4.175
- Correction in: J Musculoskelet Trauma 2025;38(1):40
-
Abstract
PDF
- Purpose
The management of distal radius fractures (DRFs) has evolved with the introduction of volar locking plate (VLP) fixation, offering stable fixation and better outcomes. Nevertheless, the impact of the surgeon’s experience on the complication rates in VLP fixation remains to be determined, particularly for less-experienced surgeons. This study compared the complication rates during the initial four years and subsequent two years of a hand surgeon’s practice of VLP fixation for DRFs.
Materials and Methods
The data between March 2016 and December 2022 were analyzed retrospectively under the Institutional Review Board approval. A single surgeon performed all VLP fixation surgeries after finishing regular hand surgery training, with the first four years representing the less experienced phase (Group 1) and the following two years indicating the experienced phase (Group 2). The patients’ characteristics, operation-related factors, and postoperative complications, including tendon injuries, nerve-related complications, fixation and instrument-related issues, osteosynthesis-related problems, and infections, were compared. In addition, the authors compared the data with a large multicenter study conducted by experienced hand surgeons.
Results
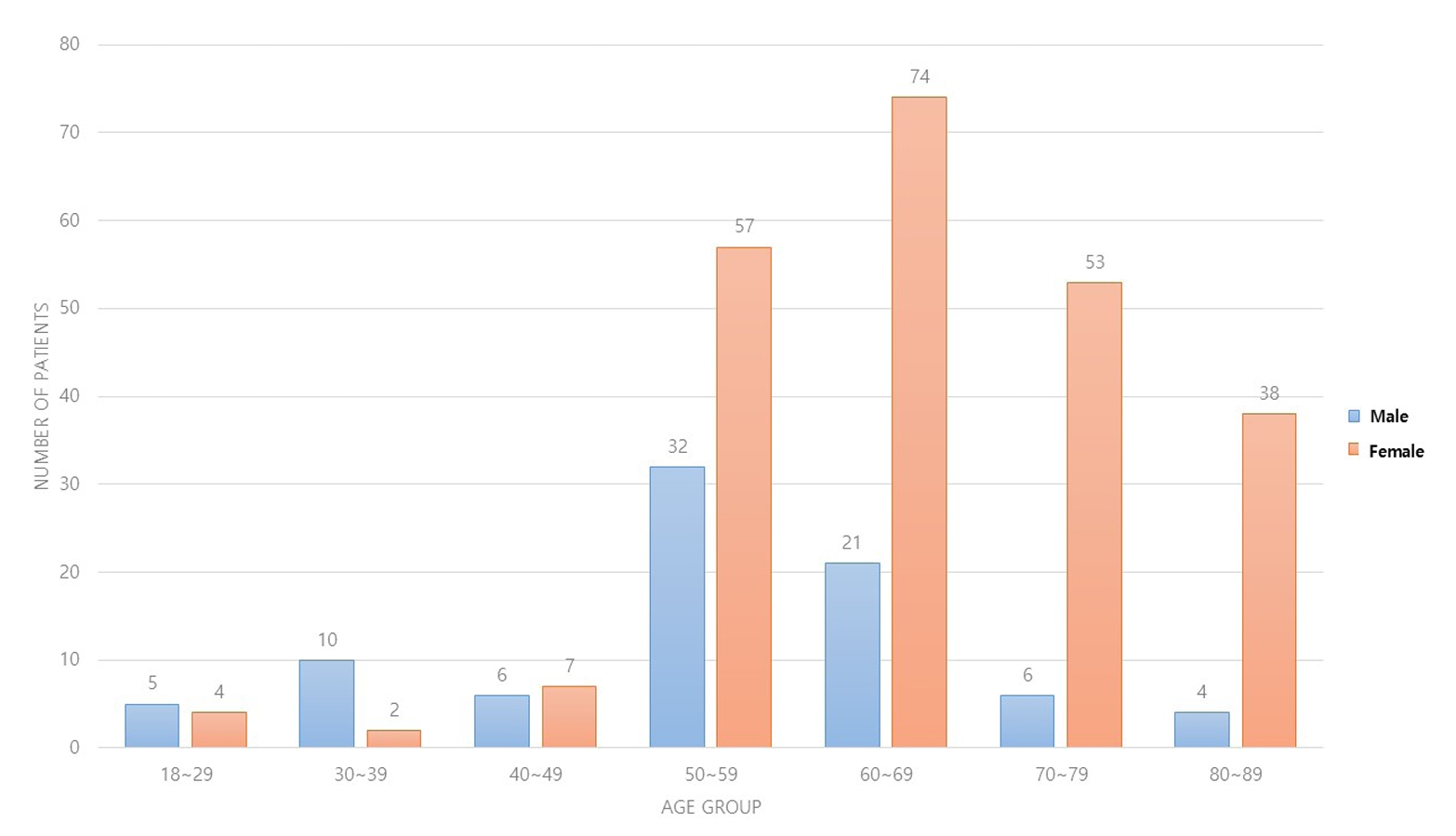
Three hundred and nineteen patients (321 wrists) were included. The mean age was 63.3 years, and 26.3% were male and 73.7% were female. The operation time was 53.7±14.5 minutes and 74.4±26.5 minutes in groups 1 and 2, respectively, which was statistically significantly shorter (p<0.001). The complication rates between the two groups were similar, except for the higher implant removal rates in Group 1. A comparison with a previous multicenter study revealed higher reduction losses and carpal tunnel syndrome in this study, but the overall complication rate was low.
Conclusion
In DRF management, when the operating surgeon has completed an accredited training course, VLP fixation is a good treatment method that can be performed effectively even by less experienced surgeons with low complication rates. -
Citations
Citations to this article as recorded by- Epidemiological changes and surgical trends of distal radius fractures in adults over 50 years during the COVID-19 pandemic in Korea: a nationwide repeated cross-sectional study
Han-Kook Yoon, So Ra Yoon, Kee-Bum Hong, Youngsu Jung, SeongJu Choi, Jun-Ku Lee
Journal of Musculoskeletal Trauma.2026; 39(1): 12. CrossRef - Author correction: “Does the operator's experience affect the occurrence of complications after distal radius fracture volar locking plate fixation? A comparative study of the first four years and thereafter”
Kee-Bum Hong, Chi-Hoon Oh, Chae Kwang Lim, Sungwoo Lee, Soo-Hong Han, Jun-Ku Lee
Journal of Musculoskeletal Trauma.2025; 38(1): 40. CrossRef - Characteristics of patients with distal radius fracture requiring arthroscopic foveal repair after bone union
Min Jung Park, Cheungsoo Ha, Hyun Tak Kang, Yong Hyun Yoon, Jun-Ku Lee, Soo-Hong Han
Arthroscopy and Orthopedic Sports Medicine.2025; 12(2): 70. CrossRef
- Epidemiological changes and surgical trends of distal radius fractures in adults over 50 years during the COVID-19 pandemic in Korea: a nationwide repeated cross-sectional study
- 2,757 View
- 53 Download
- 3 Crossref
Review Articles
- Avulsion Fractures of around the Hand
- Dong Whan Kim, Jung Il Lee
- J Korean Fract Soc 2024;37(3):158-168. Published online July 31, 2024
- DOI: https://doi.org/10.12671/jkfs.2024.37.3.158
-
Abstract
PDF
- An avulsion fracture occurs when soft tissues, including the tendons and ligaments, are forcibly detached from the main bone by an external force. The hand contains numerous anatomical structures, such as ligaments, tendons, and volar plates, which are essential for maintaining multidirectional motion and joint stability. Excessive force applied in a specific direction can damage these structures, leading to avulsion fractures around the joint. These fractures can result in severe complications if left untreated or improperly managed, including joint deformity, contracture, nonunion or malunion of the fracture, secondary osteoarthritis, and limited range of motion. Therefore, an accurate examination, diagnosis, and appropriate treatment are crucial for preventing these adverse outcomes. An avulsion fracture can be managed conservatively when the avulsed fragment does not compromise joint stability or motion. Nevertheless, surgical intervention is required to stabilize the fragment if it affects joint stability or motion. The use of internal fixation has become more prevalent because of recent advances in small implants for fixation.
- 1,080 View
- 18 Download
- Avulsion Fractures around the Hip Joint and Pelvis
- Ha-Yong Kim, Hajun Jang, Jung-Taek Kim, Jin-Woo Kim, Jun-Il Yoo, Won-Sik Choy, Yonghan Cha
- J Korean Fract Soc 2024;37(3):150-157. Published online July 31, 2024
- DOI: https://doi.org/10.12671/jkfs.2024.37.3.150
-
Abstract
PDF
- Avulsion fractures occur when tendons or ligaments are subjected to forces greater than they can withstand at the apophysis or enthesis, regardless of the fusion status. Given the diverse muscular structures around the pelvis and hip joint, which serve as origins for multiple muscles leading to the lower extremities, these areas are vulnerable to such injuries. Pelvic avulsion fractures commonly af-fect young athletes, but they can also occur in adults. Diagnosis typically involves assessing the trauma history, clinical examination, and radiographic imaging. In cases of unclear diagnosis, additional tests, such as computed tomography or magnetic resonance imaging, may assist in treatment decisions and diagnosis. Although most avulsion fractures respond well to conservative treatment, surgical interven-tion may be preferred in severe displacements, significant retraction in active athletes, or when a faster recovery is necessary. Chronic or neglected injuries may lead to excessive osseous formation around the pelvis, causing impingement syndromes. Recognizing the characteristic radiological findings based on the pelvic anatomy aids in accurate diagnosis because chronic injuries might mimic tumors or infectious conditions, necessitating a careful differential diagnosis.
- 1,537 View
- 45 Download
Original Articles
- Analysis of Missed Fractures by Bone Scan in Elderly Hip Fracture Patients with Osteoporosis
- Tae Hun Lee, Yeong Hyun Lee, Seo Won Kang
- J Korean Fract Soc 2024;37(3):144-149. Published online July 31, 2024
- DOI: https://doi.org/10.12671/jkfs.2024.37.3.144
-
Abstract
PDF
- Purpose
The incidence of hip fractures is increasing due to an increase in elderly populations because elderly patients often have accompanying diseases, such as cognitive impairment or dementia, which may lead to missed fractures. Therefore, this study assessed the utility of bone scans in detecting missed fractures in elderly patients.
Materials and Methods
This study analyzed the data from 178 patients treated from January 2014 to March 2023. The inclusion criteria were patients who had hip fractures with osteoporosis over 70 years old. Bone scans were performed on average 10 days after injury. The rate and trend of missed fractures not detected in the initial diagnosis were determined based on sex, age, dementia status, and the presence of osteoporosis.
Results
Among the 178 hip fracture patients over 70 years old, 37 patients had a history of being diagnosed with dementia, and 141 patients had never been diagnosed. Missed fractures were confirmed in 49 cases (42 patients) (23.6%). The dementia group had 13 missed fractures, and the non-dementia group had 36 missed fractures, but there was no significant difference. Rib fractures were most common, followed by vertebral fractures.
Conclusion
Missed diagnoses of fractures were common among elderly hip fracture patients. A whole body bone scan appeared to be effective in detecting missed fractures. Therefore, identifying accompanying fractures through bone scans and delivering appropriate treatment can play an important role in postoperative rehabilitation.
- 683 View
- 9 Download
- Restoration of Lateral Tibial Plateau Widening and Articular Depression Is Necessary to Prevent Valgus Deformities after Arthroscopic Reduction and Internal Fixation in AO/OTA 41.B2 or B3 Fractures
- Jun-Ho Kim, Kang-Il Kim, Sang-Hak Lee, Gwankyu Son, Myung-Seo Kim
- J Korean Fract Soc 2024;37(3):125-136. Published online July 31, 2024
- DOI: https://doi.org/10.12671/jkfs.2024.37.3.125
-
Abstract
PDF
- Purpose
This study examined the factors affecting valgus deformities after arthroscopic reduction and internal fixation (ARIF) in lateral joint-depression tibial plateau fractures.
Materials and Methods
Patients with lateral joint-depression tibial plateau fractures treated with ARIF were assessed retrospectively. The radiological evaluations included the articular depression distance (ADD) and the lateral plateau widening distance (LPWD) on preoperative and postoperative computed tomography. A postoperative valgus deformity was defined as valgus malalignment (mechanical axis ≥3°) and valgus deviation (Δmechanical axis of the operated knee from the healthy knee of ≥5°). Subgroup analyses based on a postoperative valgus deformity were performed to compare the clinical outcomes, including the range of motion, patient-reported outcomes measures, and failure and osteoarthritis progression. Furthermore, factors affecting the postoperative mechanical and Δmechanical axes were assessed.
Results
Thirty-nine patients were included with a mean follow-up of 44.6 months (range, 24-106 months). Valgus malalignment and valgus deviation were observed after ARIF in 10 patients (25.6%) and five patients (12.8%), respectively. The clinical outcomes were similar in patients with and without a postoperative valgus deformity. On the other hand, lateral compartment osteoarthritis progression was significantly higher in the valgus deformity group than in the non-valgus deformity group (valgus malalignment group: 50.0% vs 6.9%, p=0.007; valgus deviation group: 60.0% vs 11.8%, p=0.032). One patient with valgus deformity underwent realignment surgery at postoperative five years. The preoperative ADD and postoperative LPWD were significantly associated with the postoperative mechanical (both, p<0.001) and Δmechanical (ADD, p=0.001; LPWD, p=0.025) axes. Moreover, the lateral meniscectomized status during ARIF was significantly associated with the Δmechanical axis (p=0.019).
Conclusion
Osteoarthritis progression was highly prevalent in patients with postoperative valgus deformity. Thus, the restoration of lateral plateau widening and articular depression and preservation of the meniscus are necessary to prevent a valgus deformity after ARIF in lateral joint-depression tibial plateau fractures.
- 2,861 View
- 43 Download
- Comparison of Results between Minimally Invasive Plate Fixation and Antegrade Intramedullary Nailing of Recon-Type in Low-Energy Injury Distal Femoral Shaft Fractures
- Hong Moon Sohn, Gwangchul Lee, Ba Rom Kim, Jung Soo Oh
- J Korean Fract Soc 2024;37(2):87-94. Published online April 30, 2024
- DOI: https://doi.org/10.12671/jkfs.2024.37.2.87
-
Abstract
PDF
- Purpose
This study compared the outcomes of minimally invasive plate osteosynthesis and antegrade intramedullary nailing for low-energy fracture of the distal femoral shaft.
Materials and Methods
A study was conducted on 30 patients who underwent surgery for low-energy fractures of the distal femoral shaft between January 2016 and April 2022. The study compared 15patients who underwent minimally invasive plate osteosynthesis (Group P) with 15 patients who underwent recon-type antegrade intramedullary nailing (Group N). We evaluated intraoperative blood loss, operative time, C-arm exposure time, bone density, final union status, anatomical reduction, and clinical evaluation. The complications were also examined, and statistical analysis was conducted to compare the two groups.
Results
The blood loss, surgery time, and C-arm time were similar in the two groups. The radiographic assessments and clinical evaluations were also similar in the two groups. The clinical results showed no difference between the groups. Group N had one case of nonunion and one case of delayed union, while Group P had one case of nonunion and one case of peri-prosthetic fracture.
Conclusion
Antegrade intramedullary nailing of the recon-type demonstrated comparable results to minimally invasive plate osteosynthesis. Hence, antegrade intramedullary nailing of the recon-type, which enhances stability by fixing the entire femur and providing additional fixation in the distal portion, is deemed appropriate for treating distal femoral shaft fractures.
- 788 View
- 17 Download
Review Articles
- Treatment of Avulsion Fractures around the Knee
- Sumin Lim
- J Korean Fract Soc 2024;37(2):117-124. Published online April 30, 2024
- DOI: https://doi.org/10.12671/jkfs.2024.37.2.117
-
Abstract
PDF
- Avulsion fractures are common in athletes and result from high-impact or sudden, forceful movements involving the separation of a bone fragment at the ligament or tendon attachment site. The key focus areas include the anterior and posterior cruciate ligaments, medial collateral ligament, anterolateral complex, arcuate complex, medial patellofemoral ligament, patellar tendon, and quadriceps tendon. Diagnostic approaches combine radiography with advanced imaging techniques, such as computed tomography and magnetic resonance imaging, to elucidate the extent of injury and guide treatment decisions. Treatment ranges from conservative management for non-displaced fractures to surgical intervention for displaced fractures, with strategies customized based on the specific ligament involved and the nature of the fracture.
- 1,317 View
- 10 Download
- Avulsion Fractures in the Ankle and Foot
- Gyeong Hoon Lim, Jae Won Kim, Sung Hyun Lee
- J Korean Fract Soc 2024;37(2):102-116. Published online April 30, 2024
- DOI: https://doi.org/10.12671/jkfs.2024.37.2.102
-
Abstract
PDF
- An avulsion fracture occurs when a muscle-tendon unit attached to a bone produces sufficient force to tear a fragment of the bone. If not treated properly, this injury can lead to deformity, nonunion, malunion, pain, and disability. Although avulsion fractures around the foot and ankle can occur anywhere there are tendon and ligament attachments, they are common in the anterior talofibular ligament, anterior-inferior tibiotalar ligament, calcaneal tuberosity, the base of the fifth metatarsal, and navicular bone. The optimal treatment for each fracture depends on the location and severity of the fracture. Conservative treatment involves limiting weight bearing for a period, splint immobilization, and using various orthoses. Surgical treatment is usually reserved for cases of severe displacement or when nonsurgical treatment has failed. The goals of surgery include reduction of the fracture fragment, prevention of nonunion or malunion and soft tissue injury, and early return to function. The decision for each treatment modality may depend on the patient demographics or preferences and the surgeon experience. This review summarizes previous and current views on the pathogenesis, diagnosis, and treatment of common avulsion fractures to guide the treatment and diagnosis.
- 2,097 View
- 48 Download
- Complications of Hand Fractures and Its Prevention
- Jong Woo Kang
- J Korean Fract Soc 2024;37(1):46-51. Published online January 31, 2024
- DOI: https://doi.org/10.12671/jkfs.2024.37.1.46
-
Abstract
PDF
- Complications of hand fractures occur regardless of the methods used for their treatment. The treatment is also challenging. The most common and troublesome complications of hand fractures are malunion, finger stiffness, and consequent functional impairment. Early recognition and meticulous treatment of these complications is essential for improvement in hand function and satisfaction. Most of all, surgeons should clearly understand that prevention of complications is the easiest way to ensure a satisfactory outcome in hand fractures.
- 685 View
- 19 Download
Original Articles
- Cephalomedullary Nailing with an Additional Cannulated Screw Fixation in Basicervical Femur Fractures
- Keong-Hwan Kim, Woo Dong Nam, Yeon Sik Heo, Gu-Hee Jung
- J Korean Fract Soc 2024;37(1):22-29. Published online January 31, 2024
- DOI: https://doi.org/10.12671/jkfs.2024.37.1.22
-
Abstract
PDF
- Purpose
The purpose of this study is to analyze the clinical results of patients with basicervical fracture undergoing cephalomedullary nailing (CMN) with an additional cannulated screw fixation compared to only performing CMN. We hypothesized that a difference may exist in the clinical outcomes if an ad-ditional screw is fixed with CMN compared to only performing CMN in basicervical fracture.
Materials and Methods
A total of 28 consecutive patients who underwent CMN for basicervical fracture were included. In 9 cases, only CMN was conducted, and in 19 cases, an additional cannulated screw fixation was performed with CMN. Bone union, sliding distance, reduction status, and fixation failure were evaluated by postoperative radiography, and ambulatory ability was evaluated by functional results. These findings were compared between a group of CMN and a group of CMN with an additional cannulated screw.
Results
There were 4 males and 24 females with a mean age of 84 years (range, 69–100 years). No significant difference was found in postoperative reduction, tip-apex distance, bone union, and walking function recovery after surgery between the two groups, but in the sliding distance of the lag screw, the CMN group demonstrated more sliding (6.2 mm [range, 2.5–13.4 mm] vs 3.5 mm [range, 0.1– 9.2 mm]; p=0.045). Among the two groups, only one case of fixation failure at the postoperative four months was observed in the CMN group (p=0.321), and hemiarthroplasty with nail construct removal was performed.
Conclusion
CMN with additional cannulated screw fixation is a safe and reliable surgical option in basicervical fracture. It provided favorable clinical outcomes and may be a good alternative for treating basicervical fracture.
- 1,273 View
- 14 Download
- Short-term Treatment Comparison of Teriparatide and Percutaneous Vertebroplasty in Patients with Acute Osteoporotic Vertebral Compression Fractures
- Joonoh Seo, Ki Youn Kwon, Bumseok Lee, Hoon-Sang Sohn
- J Korean Fract Soc 2024;37(1):15-21. Published online January 31, 2024
- DOI: https://doi.org/10.12671/jkfs.2024.37.1.15
-
Abstract
PDF
- Purpose
This study compared the 3-month treatment effects of teriparatide and percutaneous vertebroplasty for acute osteoporotic vertebral compression fractures.
Materials and Methods
A retrospective study was conducted on 76 patients diagnosed with acute osteoporotic vertebral compression fractures from January 1, 2020 to December 31, 2022. The patients were divided into the teriparatide group and the percutaneous vertebroplasty+alendronate group. The visual analog scale (VAS), Oswestry disability index (ODI), and height of the vertebrae anterior wall were measured before treatment and at 1 and 3 months after treatment.
Results
Of the 76 patients, 42 were treated with teriparatide, and 34 were treated with percutaneous vertebroplasty. The symptoms improved in both groups, with a decrease in the VAS and ODI scores at 1 and 3 months after treatment, respectively. On the other hand, there was no significant difference in the VAS, ODI score, and anterior vertebral body height between the two groups before treatment and at 1 and 3 months after treatment.
Conclusion
In the treatment of acute osteoporotic vertebral compression fractures, conservative treatment using teriparatide showed similar short-term (3 months) treatment results to percutaneous vertebroplasty in terms of improvement in back pain and function and degree of reduction in anterior vertebral body height.
- 994 View
- 32 Download
Review Articles
- Systematic Diagnosis and Treatment Principles for Acute Fracture-Related Infections
- Jeong-Seok Choi, Jun-Hyeok Kwon, Seong-Hyun Kang, Yun-Ki Ryu, Won-Seok Choi, Jong-Keon Oh, Jae-Woo Cho
- J Korean Fract Soc 2023;36(4):148-161. Published online October 31, 2023
- DOI: https://doi.org/10.12671/jkfs.2023.36.4.148
-
Abstract
PDF
- Acute fracture-related infection (FRI) is a common and serious complication of fracture treatment. The clinical symptoms of the patient and the results of the serological, radiological, and histopathologi-cal examinations can be divided into ‘Confirmatory’ criteria and ‘Suggestive’ criteria, allowing for the diagnosis of FRI. Treatment principles can be broadly categorized into (1) the DAIR (Debridement, Antimicrobial therapy, Implant Retention) method and (2) the staged reconstruction method. The choice of treatment depends on factors such as the time elapsed after infection, stability of the internal fixation device, reduction status, host physiology, and virulence of the pathogens. Thorough surgical debridement and irrigation, ensuring stability at the fracture site, reconstruction of bone defects, and appropriate soft tissue coverage, along with antibiotic therapy, are essential to suppress or eradicate the infection. The restoration of limb function should be promoted through proper soft tissue coverage and bone union at the fracture site.
- 816 View
- 15 Download
- Fracture-Related Complications: What You Can Do to Prevent Infection
- HoeJeong Chung, Jin Woo Lee, Sang-Ho Lee, Hoon-Sang Sohn
- J Korean Fract Soc 2023;36(4):139-147. Published online October 31, 2023
- DOI: https://doi.org/10.12671/jkfs.2023.36.4.139
-
Abstract
PDF
- Fracture-related infections (FRI) can occur when bacteria enter the wound during a traumatic injury. All efforts should be made to prevent FRI-associated complications due to the complexity of treatment at the time of onset and poor treatment outcomes. The risk factors for FRIs vary and several preoperative, perioperative, and postoperative measures can be implemented to prevent infections. Preoperative measures include blood sugar control, nutritional support, discontinuation of steroids and immunosuppressants, treatment of accompanying pre-existing infections, and decolonization of pathogens, specifically Staphylococcus aureus. The perioperative and postoperative measures include the use of prophylactic antibiotics, proper surgical site preparation (hair removal, preoperative washing, skin antisepsis), suitable surgical environment (operating room ventilation system, behavioral interventions in the operating room), correct surgical techniques (debridement, irrigation, wound closure, and negative pressure wound therapy). All medical staff should pay careful attention and ensure the implementation of the correct preventive measures.
- 801 View
- 26 Download
Original Articles
- Bone Union Time of Simple Distal Femur Fractures in the Elderly according to Fracture Gap after Treated with Minimally Invasive Plate Osteosynthesis
- Young Ho Cho, Sangwoo Kim, Jaewook Koo
- J Korean Fract Soc 2023;36(4):133-138. Published online October 31, 2023
- DOI: https://doi.org/10.12671/jkfs.2023.36.4.133
-
Abstract
PDF
- Purpose
This study examined the difference in bone union time according to the fracture gap after minimally invasive plate osteosynthesis (MIPO) for simple distal femoral fractures in elderly patients.
Materials and Methods
From January 2010 to December 2019, patients aged 60 years or older who underwent surgical treatment for distal femoral fractures due to a low-energy injury were investigated retrospectively. Forty patients were enrolled in the study. The patients were divided into two groups according to the fracture gap after reduction: no more than 2 mm (Group A) and more than 2 mm (Group B) in the anteroposterior and lateral plane. The demographic, operation time, presence or absence of cerclage wiring, plate screw density, plate span ratio, plate length, bone union period, non-union, and complications were evaluated.
Results
No statistical differences in operation time, cerclage wiring, plate screw density, plate span ratio, and plate length were observed between the two groups, and the bone union was achieved in all patients without complication. The bone union period was 17.24±1.48 weeks in Group A and 24.53± 5.20 weeks in Group B, which was statistically significant (p<0.001).
Conclusion
The bone union time in treating geriatric simple distal femur fractures using the MIPO tech-nique was significantly shorter in the 2 mm or less fracture gap than in the greater than 2 mm group.
- 760 View
- 5 Download
- Outcomes of Minimally Invasive Surgery in Intra-Articular Calcaneal Fractures: Sanders Type III, Joint Depressive Type Calcaneal Fracture
- Je Hong Ryu, Jun Young Lee, Kang Yeol Ko, Sung Min Jo, Hyoung Tae Kim
- J Korean Fract Soc 2023;36(3):85-94. Published online July 31, 2023
- DOI: https://doi.org/10.12671/jkfs.2023.36.3.85
-
Abstract
PDF
- Purpose
To evaluate the radiologic and clinical outcomes of a minimally invasive technique using the tarsal sinus approach in the management of Sanders type III, joint depressive type calcaneal fractures.
Materials and Methods
Between July 2011 and September 2019, data of 29 patients who underwent a minimally invasive procedure with the sinus tarsi approach for Sanders type III joint depressive intra-articular calcaneal fractures, and were followed up for more than 1 year were analyzed. We evaluated the radiologic outcomes by assessing the radiologic parameters (Böhler angle, Gissane angle, calca-neal length, calcaneal height, calcaneal width). We also evaluated the clinical outcomes based on the American Orthopaedic Foot and Ankle Society (AOFAS) ankle-hindfoot score and the complications associated with the technique.
Results
The radiological results showed an improvement in the Böhler angle from 2.5° to 18.6° and the Gissane angle from 132.4° to 119.1° after the operation. The mean AOFAS score during the clini-cal evaluation was 79.5. We observed 13 cases of posttraumatic arthritis, 1 case of subtalar arthrodesis, and no case of wound complication.
Conclusion
Minimally invasive technique for Sanders type III joint depressive calcaneal fractures resulted in relatively satisfactory radiologic and clinical outcomes. Open reduction and internal fixation through the sinus tarsi approach reduce complications including wound problems. This approach offers satisfactory results without long-term complications.
- 564 View
- 2 Download
Case Report
- Single Percutaneous Retrograde Anterior Column Screw Fixation in a Minimally Displaced Transverse Acetabular Fracture - A Case Report -
- Seungyup Shin, Jinkyu Park, Sungho Lee
- J Korean Fract Soc 2023;36(2):57-61. Published online April 30, 2023
- DOI: https://doi.org/10.12671/jkfs.2023.36.2.57
-
Abstract
PDF
- According to the Letournel classification, a transverse fracture is the only elementary fracture pattern that breaks both the anterior and posterior border of the innominate bone. A transverse acetabular fracture separates the innominate bone into two segments: the iliac segment and the ischiopubic segment. Therefore, minimally displaced transverse fractures can be stabilized by purchasing both segments with a large-diameter single screw. Although it is not a stable internal fixation construct compared with plates and screws, it provides sufficient stability to promote early mobilization and early weight-bearing while minimizing the risk of secondary displacement and preventing secondary complications associated with prolonged bed rest and immobilization. The authors successfully treated a case of minimally displaced transverse acetabular fracture with percutaneous column fixation using a retrograde fashion of a single anterior column screw. This report discusses the case with a literature review and deliberates the usefulness of the procedure.
- 505 View
- 11 Download
Original Article
- Demographic and Radiographic Parameters as Predictors of Reduction Loss after Conservative Treatment of Distal Radius Fractures in Adults
- Kyu Jin Kim, Dae Won Shin, Seong Kee Shin
- J Korean Fract Soc 2023;36(2):45-51. Published online April 30, 2023
- DOI: https://doi.org/10.12671/jkfs.2023.36.2.45
-
Abstract
PDF
- Purpose
This study examined the demographic and radiological risk factors for later reduction loss of distal radius fractures treated conservatively. Materials and Methods This study enrolled patients treated for distal radius fractures between January 2017 and December 2019. Seventy-eight patients were included in the analysis and divided into two groups. The patients who showed minimal reduction loss within an acceptable radiologic angle after initial manual reduction were classified as Group A. The patients who showed reduction loss out of an acceptable radiologic angle and finally malunited or converted to surgical treatments were classified as Group B. The patient’s age and bone marrow density were used as demographic data. The initial X-ray images were evaluated to determine the fracture type. Various radiological parameters were measured. Results The 78-patient study cohort consisted of nine men and 69 women with a mean age of 67 years. Forty-eight cases were sorted into Group A, and 30 cases into Group B. On logistic regression analysis, the age of 80 or older was a risk factor for later fracture displacement among the demographic factors (p=0.037, odds ratio=4.937). Among the radiographic factors, the presence of distal ulnar fracture and dorsal cortical comminution were disclosed as risk factors of later displacement (p=0.049, 0.003, odds ratio=3.429, 7.196). Conclusion When conservative management for distal radius fracture is decided in patients more than 80 years of age or accompanied by a distal ulnar fracture or with dorsal cortical comminution, the possibility of later displacement of the distal radius should be considered.
- 515 View
- 2 Download
Review Article
- Fragility Fractures of the Pelvis and Sacrum
- Se-Won Lee, Ju-Yeong Kim
- J Korean Fract Soc 2023;36(1):29-38. Published online January 31, 2023
- DOI: https://doi.org/10.12671/jkfs.2023.36.1.29
-
Abstract
PDF
- The incidence of fragility fractures of the pelvis (FFP) has increased significantly due to the aging popu-lation and improved diagnostic modalities. The evaluation and treatment of these patients differ from that of high-energy pelvic ring injuries typically seen in younger patients. Therefore, it is important to classify the FFP by patterns of the classification system to standardize optimal treatment criteria and appropriate treatment strategy. However, some cases are not classifiable according to the FFP classifi-cation. A newly proposed classification that can be verified by comparing existing FFP classifications is needed to overcome the weak points. Non-operative treatment is usually considered first and should focus on early mobilization. Operative fixation should focus on stabilizing the minimally invasive pelvic ring than the reduction of fractures to facilitate early mobilization and avoid complications that can arise from comorbidities associated with immobility.
- 1,908 View
- 33 Download
Case Reports
- Isolated Avulsion Fracture of the Subscapularis from the Lesser Tuberosity of the Humerus in a 12-Year-Old Boy - A Case Report -
- Shin Seung Park, Chung Shik Shin, Won Bin Song
- J Korean Fract Soc 2022;35(2):68-73. Published online April 30, 2022
- DOI: https://doi.org/10.12671/jkfs.2022.35.2.68
-
Abstract
PDF
- An isolated avulsion fracture of the subscapularis from the lesser tuberosity of the proximal humerus is rare in the pediatric population and only a couple of cases have been described in literature. A 12-yearold right-handed boy, was admitted to the hospital with left shoulder pain after falling down the previ-ous day. Physical examination revealed tenderness on the lesser tuberosity and intertubercular groove of the humerus and a limited range of motion. Ultrasonography, computed tomography, and magnetic resonance imaging showed an isolated avulsion fracture of the subscapularis tendon from the lesser tuberosity of the humerus, accompanied by medial subluxation of the long head of the biceps tendon. In this case, a subscapularis avulsion fracture which is rare in this age group was detected at an early stage, and surgical treatment resulted in positive outcomes. Subscapularis avulsion fractures in children are difficult to diagnose in the early stages, and if not treated on time, the symptomatic improvement may be delayed. Timely and accurate diagnosis and treatment can help faster return to normal activi-ties. We would therefore like to report this case with a literature review.
- 480 View
- 3 Download
- The Antibiotic Cement Coated Nail and Masquelet Technique for the Treatment of Infected Nonunion of Tibia with Bone Defect and Varus Deformity
- Min Gu Jang, Jae Hwang Song, Dae Yeung Kim, Woo Jin Shin
- J Korean Fract Soc 2022;35(1):26-30. Published online January 31, 2022
- DOI: https://doi.org/10.12671/jkfs.2022.35.1.26
-
Abstract
PDF
- Infective nonunion after fracture surgery can cause persistent pain and inflammatory exudate in patients, requiring long-term treatment. To treat infective nonunion, radical debridement of infective bone and soft tissue should be performed, followed by stable internal fixation and bone graft. Multiple treatment strategies need to be considered according to the classification of chronic osteomyelitis, size of the bone defect, degree of bone malalignment, and severity of the soft tissue injury. This paper reports a case of a patient treated with an antibiotic cement-coated nail and a Masquelet technique to treat the infected nonunion of the tibia with a bone defect and varus deformity.
- 374 View
- 4 Download
- Early Corrective Osteoclasis for Malunited Pediatric Medial Condylar Fracture of the Humerus
- Hong Jun Jung, Ho Youn Park, Yuna Kim
- J Korean Fract Soc 2022;35(1):21-25. Published online January 31, 2022
- DOI: https://doi.org/10.12671/jkfs.2022.35.1.21
-
Abstract
PDF
- Fractures of the medial condyle of the distal humerus in children are very rare, and the younger the age, the more difficult it is to diagnose. These fractures include an intra-articular fracture and a Salter–Harris type IV growth plate fracture. Therefore, the prognosis is poor if the fracture is neglected or misdiag-nosed because of the high incidence of complications such as nonunion, angular deformity, or joint contracture. This paper reports a case of a four-year-old child who presented with a malunion of the medial condyle of the humerus with good results after an early corrective osteoclasis.
- 420 View
- 0 Download
Review Article
- Denosumab (RANKL Inhibitor): A Potent Anti-Resorptive Agent
- Seong-Eun Byun
- J Korean Fract Soc 2021;34(4):142-147. Published online October 31, 2021
- DOI: https://doi.org/10.12671/jkfs.2021.34.4.142
-
Abstract
PDF
- Denosumab, a fully human monoclonal antibody to the receptor activator of nuclear factor-kappa B ligand, was introduced and used as an anti-osteoporotic agent. Denosumab prevents bone resorption by inhibiting the differentiation and action of osteoclasts, resulting in an increase of bone mineral density and broad-spectrum anti-fracture efficacy. Clinical studies, including FREEDOM (Fracture Reduction Evaluation of Denosumab in Osteoporosis Every Six Months) and its extension up to 10 years, FREEDOM Extension, demonstrated its long-term efficacy and safety in postmenopausal osteoporosis. In addition, the efficacy and safety of denosumab were confirmed in male osteoporosis and glucocorticoid- induced osteoporosis. Therefore, recent clinical guidelines recommend denosumab as an initial treatment. This review summarizes the mechanism of action, pharmacological characteristics, efficacy, and safety issue of denosumab.
- 872 View
- 5 Download
Technical Note
- Operative Positioning Technique for an Intertrochanteric Fracture in a Patient with an Ipsilateral Above-the-Knee Amputation - Technical Note -
- Dae-Hyun Park, Yong-Uk Kwon, Dong-Seok Kim
- J Korean Fract Soc 2021;34(4):137-141. Published online October 31, 2021
- DOI: https://doi.org/10.12671/jkfs.2021.34.4.137
-
Abstract
PDF
- A 45-year-old man with a remote history of a left above-the-knee amputation presented to the emergency department with left hip pain after a mechanical fall. This case was an operative challenge because commonly used intraoperative traction methods could not be applied to a patient with an above-the-knee amputation. We describe a rarely utilized surgical technique of applying traction to an amputated extremity via a Steinmann pin during closed reduction and internal fixation of an intertrochanteric fracture.
-
Citations
Citations to this article as recorded by- Periprosthetic Femur Fractures in Osseointegration Amputees
Jason Shih Hoellwarth, S. Robert Rozbruch
JBJS Case Connector.2022;[Epub] CrossRef
- Periprosthetic Femur Fractures in Osseointegration Amputees
- 810 View
- 2 Download
- 1 Crossref
Review Article
- Current Concepts of Vitamin D and Calcium in the Healing of Fractures
- Jihyo Hwang
- J Korean Fract Soc 2021;34(3):117-121. Published online July 31, 2021
- DOI: https://doi.org/10.12671/jkfs.2021.34.3.117
-
Abstract
PDF
- Fragile fractures, also known as osteoporosis fractures, insufficiency fractures, and senile fractures are a significant problem encountered by orthopedic surgeons. Calcium and vitamin D are essential for maintaining bone health and deficiencies in calcium and vitamin D are major risk factors for the development of osteoporosis. Sufficient amounts of calcium are also required for fracture-callus mineralization. Hence, compromised bone repair that is frequently observed in osteoporotic patients might be attributed to calcium and vitamin D deficiencies. Consequently, calcium and vitamin D supplementation represents a potential strategy for treating compromised fracture healing in osteoporotic patients. There is some clinical evidence of the positive effect of supplementation in fracture healing and posttraumatic bone turnover, but research in this area is ongoing. Calcium and vitamin D should be the primary treatment of choice in osteopenic patients with an insufficiency of calcium and vitamin D and for the prevention of secondary osteoporotic fractures. Calcium and vitamin D can also be used as addition to other primary osteoporotic medications such as antiresorptive or bone-forming agents. The role of calcium and vitamin D in fracture healing and the therapeutic potential of calcium and vitamin D supplementation is summarized in this context.
- 6,904 View
- 81 Download
Original Article
- Clinical and Radiologic Outcome of Intertrochanteric Fracture Treatment Using TFNA (Trochanteric Fixation Nail-Advanced)
- Hyeon Joon Lee, Hyun Bai Choi, Ba Rom Kim, Seung Hwan Jo, Sang Hong Lee
- J Korean Fract Soc 2021;34(3):105-111. Published online July 31, 2021
- DOI: https://doi.org/10.12671/jkfs.2021.34.3.105
-
Abstract
PDF
- Purpose
This study evaluated the clinical and radiological outcomes of TFNA (Trochanteric Fixation NailAdvanced; Depuy Synthes) for the treatment of proximal femur fractures.
Materials and Methods
This was a retrospective study of 64 patients diagnosed with a proximal femur fracture from January 2019 to November 2019. The patient’s demographic data, preoperatively and postoperatively Koval grade, modified Harris hip score, EQ-5D (Euro-Qol-5 Dimension), sliding and advancement of the blade, radiologic outcome, and complications were investigated.
Results
Fifty patients were available for evaluation at one year postoperatively. The patients reported the following: the Koval grade decreased after surgery; the modified Harris hip score decreased from 78.56±8.88 to 72.74±6.59 (p=0.149); the mean EQ-5D decreased from 0.75±0.09 to 0.72±0.06 (p=0.000). Satisfactory reduction was achieved on a postoperative radiographic examination in 47 patients in six months. Complications occurred in seven cases.
Conclusion
TFNA is considered an appropriate implant for treating intertrochanteric fractures of the femur with a minimum follow-up of one year. -
Citations
Citations to this article as recorded by- Outcomes of Intertrochanteric Fracture Fixation Using the Trochanteric Fixation Nail Advanced (TFNA): A Retrospective Analysis
Ramprasad Jasti, Prithvi Mohandas, Mahesh K Ragavan, Sunil D Magadam, Umesh Kannadasan
Cureus.2025;[Epub] CrossRef - GS Hip Nail versus Affixus Hip Fracture Nail for the Intramedullary Nailing of Intertrochanteric Fractures
Seungcheol Kwon, Minjae Lee, Heeyeon Lee, Jihyo Hwang
Journal of Clinical Medicine.2023; 12(21): 6720. CrossRef - Comparison of the Clinical and Radiological Outcomes of TFNA (Trochanteric Fixation Nail-Advanced) and PFNA-II (Proximal Femoral Nail Antirotation-II) Treatment in Elderly Patients with Intertrochanteric Fractures
Min Sung Kwon, Young Bok Kim, Gyu Min Kong
Journal of the Korean Fracture Society.2022; 35(4): 162. CrossRef
- Outcomes of Intertrochanteric Fracture Fixation Using the Trochanteric Fixation Nail Advanced (TFNA): A Retrospective Analysis
- 1,105 View
- 19 Download
- 3 Crossref
Review Article
- Pediatric Fractures around the Wrist
- Gihun Kim, Kun-Bo Park
- J Korean Fract Soc 2021;34(2):80-86. Published online April 30, 2021
- DOI: https://doi.org/10.12671/jkfs.2021.34.2.80
-
Abstract
PDF
- Fractures around the wrist are the third most common fracture among all pediatric fractures. Furthermore, distal radius fractures, a type of wrist fracture, are the most common fractures in children. Understanding pediatric fractures around the wrist is very important considering their prevalence. There is a specific belief that pediatric fractures can heal easily because of remodeling, but not all fractures can heal without proper treatment. Complications such as growth problems, nonunion can occur if the fracture is not treated properly. This paper reviewed recent articles about distal radius fractures, Galeazzi-equivalent fractures, and carpal bone fractures, including scaphoid fractures in children and adolescents. Successful treatment can be achieved without complications when an accurate diagnosis and proper non-surgical or surgical treatment are performed based on this article.
- 1,416 View
- 27 Download
Case Report
- Injury of the Ascending Branch of the Lateral Femoral Circumflex Artery Caused by a Spike of the Displaced Lesser Trochanter in an Intertrochanteric Femoral Fracture - A Case Report -
- Soon Ho Huh, Hong-Man Cho, Jiyeon Park
- J Korean Fract Soc 2021;34(2):71-75. Published online April 30, 2021
- DOI: https://doi.org/10.12671/jkfs.2021.34.2.71
-
Abstract
PDF
- Although vascular injuries associated with femoral intertrochanteric fractures have been reported infrequently, bleeding due to vascular injury can lead to severe complications that can be potentially life and limb-threatening. The authors report a case of an injury of the ascending branch of the lateral femoral convolutional artery in a patient who underwent surgical treatment for a femoral intertrochanteric fracture. Vascular injury occurred due to the sharp margin of displaced lesser trochanter five weeks after surgery. Percutaneous transcatheter embolization was done and improved without additional complications. Therefore, the surgeons need to be aware of possible associated vascular injuries caused by displaced lesser trochanter fragments in femoral intertrochanteric fractures.
-
Citations
Citations to this article as recorded by- Delayed Deep Femoral Artery Injury Secondary to Migrated Lesser Trochanter Fragment After Intertrochanteric Fracture Fixation: A Case Report and Updated Literature Review
Slavko Čičak, Josip Kocur, Vedran Farkaš, Petra Čičak, Stjepan Ištvanić, Marko Lovrić, Marko Perić, Nenad Koruga, Tomislav Ištvanić
Geriatric Orthopaedic Surgery & Rehabilitation.2025;[Epub] CrossRef - Vascular Complications Following Trans-Trochanteric Fracture: Case Report and Literature Review
Robert Bot, Adrian Tirla, Simona Daniela Cavalu
Reports.2025; 8(4): 191. CrossRef
- Delayed Deep Femoral Artery Injury Secondary to Migrated Lesser Trochanter Fragment After Intertrochanteric Fracture Fixation: A Case Report and Updated Literature Review
- 612 View
- 4 Download
- 2 Crossref
Review Article
- Pediatric Femoral Neck Fracture
- Joo Hyung Han, Hoon Park
- J Korean Fract Soc 2021;34(1):34-43. Published online January 31, 2021
- DOI: https://doi.org/10.12671/jkfs.2021.34.1.34
-
Abstract
PDF
- Pediatric femoral neck fracture is an uncommon injury with a high complication rate, regardless of the appropriate diagnosis and management. The bony anatomy and blood supply of the proximal femur in a skeletally immature patient differ from those in adult patients. Generally, these fractures result from high-energy trauma, but pathologic hip fractures also occur, usually from low-energy trauma. Pediatric femoral neck fractures are categorized using the Delbet classification system. This classification guides management and aids clinicians in determining the risk of avascular osteonecrosis. The ideal surgical treatment is determined by the fracture type and the age of the patient. Reduction, which is achieved using a closed or open procedure, combined with stable fixation and/or cast immobilization, is recommended for most of these fractures. Anatomical reduction within 24 hours from the injury may result in a good surgical outcome. Although the effects of capsular decompression after reduction and fixation have not been established, decompression is easy to perform and may reduce the risk of avascular necrosis. Despite appropriate management, osteonecrosis can occur after all types of pediatric femur neck fractures. Other complications include coxa vara, nonunion, and premature physeal arrest.
- 1,412 View
- 29 Download
Case Report
- Latent Superior Gluteal Artery Injury by Entrapment between the Fragments in Transverse Acetabular Fracture - A Case Report -
- Hyuk Jin Choi, Byung Chul Kim, Hoon Kwon, Jae Hoon Jang
- J Korean Fract Soc 2021;34(1):30-33. Published online January 31, 2021
- DOI: https://doi.org/10.12671/jkfs.2021.34.1.30
-
Abstract
PDF
- The superior gluteal artery is branched from the internal iliac artery and is located outside the pelvis through a greater sciatic notch. This anatomical characteristic makes the artery vulnerable to injury when pelvic fracture involves the sciatic notch. In the case of a superior gluteal artery injury, hemodynamic instability can occur, and appropriate evaluation and management are mandatory in the acute phase. On the other hand, if the initial detection of the injury is neglected due to a masked pattern, it can cause massive bleeding during surgery, resulting in difficult hemostasis. This paper reports an experience of a latent superior gluteal artery injury by entrapment between the fragments of a transverse acetabular fracture.
-
Citations
Citations to this article as recorded by- Superior gluteal artery injury in pelvic ring injury and acetabular fracture: Single center observational study
Hoon Kwon, Jae Hoon Jang, Nam Hoon Moon, Seung Joon Rhee, Dong Yeon Ryu, Tae Young Ahn
Journal of Orthopaedic Science.2024; 29(6): 1483. CrossRef
- Superior gluteal artery injury in pelvic ring injury and acetabular fracture: Single center observational study
- 771 View
- 5 Download
- 1 Crossref
Original Article
- Primary Open Reduction and Plate Fixation in Open Comminuted Intra-Articular Distal Radius Fracture
- Jun-Ku Lee, Soonchul Lee, Weon Min Cho, Minkyu Kil, Soo-Hong Han
- J Korean Fract Soc 2021;34(1):16-22. Published online January 31, 2021
- DOI: https://doi.org/10.12671/jkfs.2021.34.1.16
-
Abstract
PDF
- Purpose
There are no standard surgical treatments for open distal radius fractures (DRFs), and the fracture fixator is chosen by the surgeon’s own experience. This study compared the outcomes of open reduction and volar locking plating (OR VLP) between closed and open AO-OTA type C3 DRFs. Materials and Methods: Patient data were retrospectively collected between January 2010 and December 2018. Only patients aged >18 years with AO-OTA C3 DRFs were included. After further exclusion, the patients with DRFs were divided into two groups: 13 patients with open DRFs in Group 1 and 203 patients with closed DRFs in Group 2. Data on the patient characteristics and treatment-related factors were further investigated. For the radiological evaluation, the radial height, volar height, and volar titling were measured based on the final plain radiography, and the union time was measured. The wrist range of motion (ROM), pain visual analogue scale score, and modified Mayo wrist score for function were measured at the final outpatient follow-up. Finally, the complications associated with OR VLP fixa-tion were investigated. Results: In the demographic comparison, the patients with open fractures were older (mean age, 62years) than those with closed fractures (mean age, 57 years), without a statistically significant differ-ence. The patients with open DRFs had longer antibiotic therapy and hospital stay durations. Although they presented a higher radial inclination, with statistical significance, the clinical implication was low with a mean difference of 3°. No significant differences were observed for the remaining radiological parameters, wrist ROM, and functional scores. An open DRF did not increase the complication rates,including deep infection. Conclusion: Depending on the expertise of the operating surgeon, the primary OR VLP fixation in open intra-articular comminuted DRF did not increase the incidence of deep infections and yielded similar outcomes to a closed intra-articular comminuted DRF.
- 1,143 View
- 12 Download
Case Reports
- Sclerotherapy Using Abnobaviscum for the Extensive Recurrent Chronic Morel-Lavallée Lesions - A Case Report -
- Joon-Kuk Kim, Ji-Won Jung, Ki-Chul Park
- J Korean Fract Soc 2020;33(4):222-226. Published online October 31, 2020
- DOI: https://doi.org/10.12671/jkfs.2020.33.4.222
-
Abstract
PDF
- The Morel-Lavallée lesion (MLL) is a closed soft-tissue degloving injury, resulting in characteristic hemo-lymphatic fluid collection between the fascia and subcutaneous layers. The MLL was managed routinely with drainage and compression bandages, but sclerotherapy can be used in patients with chronic lesions refractory to first-line therapy. This paper presents a case of extensive recurrent chronic MLL treated with sclerotherapy using Abnobaviscum, which has been used to treat adhesion in malignant pleural effusion.
-
Citations
Citations to this article as recorded by- Seroma prevention with topical Abnobaviscum sclerotherapy following excision of giant cervical lipoma
Jun Ho Choi, Seung Yeon Choi, Jae Ha Hwang, Kwang Seog Kim, Sam Yong Lee
Archives of Craniofacial Surgery.2023; 24(1): 10. CrossRef
- Seroma prevention with topical Abnobaviscum sclerotherapy following excision of giant cervical lipoma
- 753 View
- 10 Download
- 1 Crossref
- Rendezvous Surgery for Peri-Implant Fractures around Locking Compression Plate on Anterolateral Bowed Femur - A Case Report -
- Hong Man Cho, Jiyeon Park
- J Korean Fract Soc 2020;33(3):159-163. Published online July 31, 2020
- DOI: https://doi.org/10.12671/jkfs.2020.33.3.159
-
Abstract
PDF
- An 84-year-old female visited with an intertrochanteric femoral fracture. The patient had undergone an open reduction and internal fixation with a compressive plate and elastic nail in an ipsilateral atypical diaphyseal femoral fracture in the past. Compressive plate and elastic nail remained, and anterolateral bowing was presented. To treat the periprosthetic trochanteric fracture, a proximal femoral nail was used without removing the previously inserted compressive plate. Under the “rendezvous” technique, using a combination of fixating intramedullary nail and compressive plate simultaneously, the distal screw was fixed, and a femoral head lag screw was inserted after reducing the fracture. Complete union of the fracture was achieved 16 months after the operation, and a decrease in mobility function was not found postoperatively. The authors report this case for the “rendezvous” technique as a treatment option for elderly patients with periprosthetic trochanteric fractures, who had previously undergone surgical treatment for ipsilateral atypical diaphyseal femoral fractures with anterolateral bowing.
- 487 View
- 3 Download
Original Articles
- Clinical Outcome after Treatment of Tibia Segmental Fracture with Intramedullary Nailing and Minimal Invasive Plate Osteosynthesis
- Jun Young Lee, Hyung Seok Park, Dong Hyuk Cha
- J Korean Fract Soc 2020;33(3):142-147. Published online July 31, 2020
- DOI: https://doi.org/10.12671/jkfs.2020.33.3.142
-
Abstract
PDF
- Purpose
This study examined the clinical outcomes after the treatment of a tibia segmental fracture with intramedullary nailing (IM nailing) and minimal invasive plate osteosynthesis (MIPO).
Materials and Methods
From July 2012 to December 2017, 14 out of 17 cases from a treatment cohort of 32 cases of AO type 42 C2 tibia segmental fractures with IM nailing and MIPO were studied retrospectively. Periodic radiographs were used to evaluate the presence of union, union time, and radiographic evaluation of bony union (varus-valgus deformity, anteroposterior angular deformity, shortening). To evaluate the postoperative clinical function, modified Rasmussen’s system was used for proximal fractures, and the American Orthopaedic Foot and Ankle Society functional score was used for distal fractures.
Results
Bony union was achieved in all 14 cases, and the average union time was 26 weeks. In one case of soil contamination, there were no other complications other than simple debridement after a soft tissue infection. The mean varus was two degrees; the mean anteroposterior angular deformity was three degrees of anterior oblique; the mean length shortening was 5 mm (2-9 mm). The mean functional score of the knee joint with the Modified Rasmussen’s system measured for the postoperative clinical function was relatively good (excellent 9, good 4, fair 1, and poor 0). The results of the Molander and Olerud Functional scores of the ankle joints were also good (excellent 8, good 3, fair 2, poor 0).
Conclusion
The treatment of tibia segmental fractures with IM nailing and MIPO can effectively reduce the gap of fracture sites. Hence, it is possible to increase the bony union probability and obtain relatively satisfactory alignment. Overall, the treatment of tibia segmental fractures with IM nailing and minimally invasive plate osteosynthesis appears to be a useful treatment, considering the preservation of the soft tissue and the alignment of the tibia.
- 648 View
- 4 Download
- Results of Single Small Incision Minimally Invasive Plate Osteosynthesis in the Treatment of the Distal Radius Fractures
- Young Sung Kim, Jong Pil Kim, Phil Hyun Chung, Ho Min Lee, Bo Sung Go
- J Korean Fract Soc 2020;33(2):72-80. Published online April 30, 2020
- DOI: https://doi.org/10.12671/jkfs.2020.33.2.72
-
Abstract
PDF
- Purpose
This study compared minimally invasive plate osteosynthesis (MIPO) using a single small skin incision and conventional open volar locking plate fixation (OP) for distal radius fracture to identify outcome difference.
Materials and Methods
Forty-three patients who underwent MIPO using a single small skin incision or OP for distal radius fractures were evaluated retrospectively. Of the patients, 21 were treated with MIPO using a single small skin incision and 22 with the OP method through the conventional volar approach. The postoperative radiographic results and clinical outcomes at the final follow-up in each group were compared.
Results
All patients achieved bone union in the MIPO and OP groups. No significant differences in the bone union time, alignment, range of motion, QuickDASH, or pain score were observed. On the other hand, the size of the incision was significant: 23 mm in the MIPO group and 55 mm in the OP group (p<0.001).
Conclusion
MIPO technique using a single small incision showed similar satisfactory radiographic and functional outcomes compared to conventional OP for distal radius fractures. The MIPO technique using a single small incision offered advantages, including cosmetic benefits and minimal soft tissue damage, is recommended, particularly in young women and high functional demand patients.
- 715 View
- 9 Download
- Analysis of the Changes in Femoral Varus Bowing and the Factors Affecting Nonunion for the Treatment of Femoral Shaft Fractures over 60 Years Old Using Piriformis Fossa Insertion Intramedullary Nailing
- Yonghan Cha, Chan Ho Park, Jun-Il Yoo, Jung-Taek Kim, WooSuk Kim, Ha-Yong Kim, Won-Sik Choy
- J Korean Fract Soc 2020;33(2):65-71. Published online April 30, 2020
- DOI: https://doi.org/10.12671/jkfs.2020.33.2.65
-
Abstract
PDF
- Purpose
This study examined the bony morphological changes to analyze the factors affecting bony union in the treatment of elderly femoral shaft fractures with varus bowing using piriformis fossa insertion intramedullary nailing.
Materials and Methods
This study included 26 patients over 60 years of age, who were admitted for femoral shaft fractures between January 2005 and December 2014 and treated with piriformis fossa insertion intramedullary nailing. Age, sex, height, weight, bone mineral density, injury mechanism, fracture type, diameter and length of the nail, postoperative lengthening of the femur, postoperative change in varus angle, contact between the lateral and anterior cortex, and the gap between the fracture line and the bony union were checked. The patients were divided into a varus group and nonvarus group, as well as a bone union group and nonunion group. Logistic regression analysis was performed to analyze the factors affecting nonunion.
Results
The patients were classified into 11 in the varus group and 15 in the non-varus group and 24 in the union group and 2 in the nonunion group. The varus group showed a larger increase in leg length and varus angle reduction than the non-varus group (p<0.05). The union group had more contact with the lateral cortical bone than that of the nonunion group (p<0.05). The factor affecting bone union in regression analysis was contact of the lateral cortical bone (p<0.05).
Conclusion
Treatment of a femoral shaft fracture in elderly patients with a varus deformity of the femur using piriformis fossa insertion intramedullary nail increases the length of the femur and decreases the varus deformity. For bony union, the most important thing during surgery is contact of the lateral cortical bone with the fracture site. -
Citations
Citations to this article as recorded by- Straight nail insertion through a laterally shifted entry for diaphyseal atypical femoral fractures with bowing: good indications and limitations of this technique
Seong-Eun Byun, Young-Ho Cho, Young-Kyun Lee, Jung-Wee Park, Seonguk Kim, Kyung-Hoi Koo, Young Soo Byun
International Orthopaedics.2021; 45(12): 3223. CrossRef
- Straight nail insertion through a laterally shifted entry for diaphyseal atypical femoral fractures with bowing: good indications and limitations of this technique
- 1,056 View
- 6 Download
- 1 Crossref
Review Article
- Treatment of Periprosthetic Femoral Fractures after Hip Arthroplasty
- Jung Hoon Choi, Jong Hyuk Jeon, Kyung Jae Lee
- J Korean Fract Soc 2020;33(1):43-51. Published online January 31, 2020
- DOI: https://doi.org/10.12671/jkfs.2020.33.1.43
-
Abstract
PDF
- Although the incidence of postoperative periprosthetic femoral fractures after hip arthroplasty is expected to increase, these complex fractures are still challenging complications. To obtain optimal results for these fractures, thorough clinical and radiographic evaluation, precise classification, and understanding of modern management principles are mandatory. The Vancouver classification system is a simple, effective, and reproducible method for planning proper treatments of these injuries. The fractures associated with a stable femoral stem can be effectively treated with osteosynthesis, though periprosthetic femoral fractures associated with a loose stem require revision arthroplasty. We describe here the principles of proper treatment for the patients with periprosthetic femoral fractures as well as how to avoid complications.
- 1,499 View
- 10 Download
Case Report
- Brachial Plexus Neuropathy after Revision of Clavicular Fracture Nonunion: A Case Report
- Youngwoo Kim, Suk Kyu Choo, Neunghan Jeon
- J Korean Fract Soc 2020;33(1):22-26. Published online January 31, 2020
- DOI: https://doi.org/10.12671/jkfs.2020.33.1.22
-
Abstract
PDF
- We performed a revisionary open reduction and internal fixation for treating nonunion of the mid-shaft of the left clavicle with an autogenous cancellous bone graft. On postoperative day 4, the patient presented with neurologic deficits in the left upper extremity. We removed the implant and made a superior angulation to decompress the brachial plexus. At 6 months postoperatively, callus bridging and consolidation were visible and all hand and elbow functions were fully recovered. Our case suggests that brachial plexus neuropathy may be caused by stretching and compression after reduction and straightening of the nonunion site around adhesions or scar tissue. Therefore, care should be taken whether there are the risk factors that can cause brachial plexus neuropathy when revision surgery is performed for treating nonunion of a clavicle shaft fracture.
-
Citations
Citations to this article as recorded by- Arcuate osteoplasty for brachial plexus paralysis after plate fixation of mid-clavicle fracture: a case report and literature review
Dongju Shin, Jae Hwi Han
Clinics in Shoulder and Elbow.2025; 28(3): 394. CrossRef
- Arcuate osteoplasty for brachial plexus paralysis after plate fixation of mid-clavicle fracture: a case report and literature review
- 1,142 View
- 1 Download
- 1 Crossref
Original Article
- Treatment of Isolated Lateral Malleolar Fractures Using Locking Compression Plate Fixation and Tension Band Wiring Fixation
- Woojin Shin, Seondo Kim, Jiyeon Park
- J Korean Fract Soc 2020;33(1):16-21. Published online January 31, 2020
- DOI: https://doi.org/10.12671/jkfs.2020.33.1.16
-
Abstract
PDF
- PURPOSE
The purpose of this study was to compare the clinical and radiological outcomes of locking compression plate (LCP)-screw fixation and tension band wiring (TBW) fixation in isolated lateral malleolar fractures.
MATERIALS AND METHODS
From May 2016 to August 2018, 52 patients with isolated lateral malleolar fracture were retrospectively reviewed. They were divided into 30 cases of the LCP fixation group (Group I) and 22 cases of the TBW fixation group (Group II). The clinical and radiological results of those groups were compared. Pearson chi-square tests and independent t-tests were used in the statistical analysis.
RESULTS
The mean length of the surgical incision was 8.3 cm in Group I and 4.9 cm in Group II. Radiological union was obtained at a mean of 8.4 weeks in both groups. The mean American Orthopaedic Foot and Ankle Society score was 90 (range, 85–97) and 92 (range, 85–100) in Groups I and II, respectively, at the last follow up.
CONCLUSION
Both the LCP-screw and TBW techniques revealed excellent results in isolated lateral malleolar fractures. The tension band technique may be a fine alternative method of fixation in the treatment of isolated lateral malleolar fracture.
- 1,026 View
- 8 Download
 First
First Prev
Prev

