 E-submission
E-submission TOTA
TOTA TOTS
TOTS
Articles
- Page Path
- HOME > J Musculoskelet Trauma > Volume 39(1); 2026 > Article
-
Original Article
- Surgical outcomes of the coracoid process fracture associated with the acromioclavicular joint injury in Korea: a case series
-
Dongju Shin1
 , Sung Choi2, Sangwoo Kim2, Byung Hoon Kwack2
, Sung Choi2, Sangwoo Kim2, Byung Hoon Kwack2 -
Journal of Musculoskeletal Trauma 2026;39(1):54-61.
DOI: https://doi.org/10.12671/jmt.2025.00346
Published online: January 14, 2026
1Department of Orthopedic Surgery, W General Hospital, Daegu, Korea
2Department of Orthopedic Surgery, Daegu Fatima Hospital, Daegu, Korea
- Correspondence to: Byung Hoon Kwack Department of Orthopedic Surgery, Daegu Fatima Hospital, 99 Ayang-ro, Dong-gu, Daegu 41199, Korea Tel: +82-53-940-7324 Email: kwackbyunghoon@nate.com
• Received: November 3, 2025 • Revised: November 19, 2025 • Accepted: November 25, 2025
© 2026 The Korean Orthopaedic Trauma Association
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/4.0/) which permits unrestricted noncommercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
- 1,234 Views
- 31 Download
Abstract
-
Background Excluding technical reports and isolated case reports, there are no published studies evaluating coracoid process fixation with or without an acromioclavicular joint (ACJ) stabilization procedure for coracoid process fractures associated with ACJ injury. The purpose of this study was to assess the surgical outcomes of coracoid process fractures associated with ACJ injuries and to determine the usefulness of coracoid process fixation with or without an ACJ stabilization procedure.
-
Methods From February 2006 to December 2015, patients with coracoid process fractures associated with ACJ injuries were enrolled. Radiological and clinical outcomes were analyzed in 12 patients who underwent coracoid process fixation with or without an ACJ stabilization procedure. A 3.5 mm cannulated screw with a washer or a 3.0 mm headless compression screw was used for coracoid process fixation, and either a clavicle hook plate or Kirschner (K)-wires were used for ACJ injuries when additional fixation was necessary.
-
Results Bone union was achieved in 11 patients (91.7%), while one case was determined to be a nonunion at 6 months. Radiological union occurred at an average of 3 months (range, 1.5–4 months) in all patients except the nonunion case. At the final follow-up, the average clinical scores were a visual analogue scale pain score of 1.5 (range, 0–4) and a University of California, Los Angeles score of 30.9 (range, 28–35). Clinical outcomes were satisfactory in all patients, including the patient with nonunion.
-
Conclusions The clinical and radiological outcomes of treating coracoid process fractures associated with ACJ injuries using coracoid process fixation with or without ACJ stabilization were favorable. A cannulated screw with a washer and clavicle hook plate fixation may provide sufficient stability for both the coracoid process fracture and the ACJ injury when feasible.
-
Level of evidence IV.
Introduction
Scapular fractures accounted for only 1% of all fractures, and coracoid process fractures were relatively rare, accounting for approximately 6% to 8.2% of all scapular fractures [1,2]. Coracoid fractures and ipsilateral shoulder injuries often occur concurrently. Ogawa et al. [3] reported that 21.3% (17 of 80 cases) of coracoid fractures were accompanied by acromioclavicular joint (ACJ) dislocation. The concomitant coracoid fracture and ACJ injury indicated a double disruption to the upper shoulder support complex (SSSC). Goss [4] suggested that if the displacement is unacceptable, surgical reduction and stabilization of one or more of the injury site may be necessary. Ogawa et al. [5] showed that symptoms were present in 45% of coracoid nonunions, but most of these symptoms were insignificant. They suggested that coracoid nonunion itself is frequently asymptomatic, and that even if coracoid nonunion remains, satisfactory results can be achieved simply by treating the concurrent injury. Wignadasan et al. [6] reported that the clavicle hook plate could be safely used to treat double disruption of the SSSC in the form of concomitant coracoid base fracture and ACJ dislocation. Ye et al. [7] showed that fixation using a clavicle hook plate was a feasible treatment for coracoid fractures with ACJ dislocation and that satisfactory results were obtained. However, they reported a nonunion rate of 16.7% (3 of 18 cases) in coracoid process fractures, suggesting that the healing of coracoid process fractures may be related to the fracture morphology.
Kim et al. [8] introduced a technical report of coracoid process fixation using a cannulated screw without acromioclavicular fixation in cases of displaced fracture of the coracoid process associated with ACJ dislocation, using an open approach to the coracoid process and coracoclavicular ligament under fluoroscopic guidance. Bhatia [9] presented a technical report on percutaneous cannulated screw fixation and stabilization of coracoid base fracture associated with ACJ dislocation using coracoid fixation via indirect ACJ reduction under fluoroscopic guidance. To the best of our knowledge, no studies, excluding technical and case reports, have reported on coracoid process fixation with or without ACJ stabilization procedure in coracoid process fractures associated with ACJ injury.
The purpose of this study was to evaluate the surgical outcomes of the coracoid process fracture associated with ACJ injury and to determine the usefulness of coracoid process fixation with or without ACJ stabilization procedure.
Methods
This study was approved by the Institutional Review Board (IRB) of Daegu Fatima Hospital (IRB No. 2025-10-001), and the requirement for informed consent was waived.
This study was a retrospective single-center case series evaluating surgically treated coracoid process fractures associated with ACJ injury. We reviewed medical records and imaging studies to describe radiologic union, clinical outcomes, and postoperative complications after coracoid fixation with or without ACJ stabilization at Daegu Fatima Hospital (Daegu, Korea) among those treated between February 2006 and December 2015.
With the patient in the beach-chair position under general anesthesia, an oblique incision was made along Langer’s lines between the coracoid process and the ACJ. Under C-arm fluoroscopic guidance, the lateral end of the clavicle was gently depressed to restore the AC joint alignment, and temporary fixation was achieved with a Kirschner (K)-wire. This maneuver reduced the tensile force transmitted through the coracoclavicular ligament, thereby allowing adequate compression during coracoid screw fixation.
After palpating the coracoid process, a guidewire was advanced through the fracture site toward the glenoid under orthogonal biplanar fluoroscopic control, following the technique described by Bhatia [9]. Once the position and depth of the guidewire were confirmed, a 3.5 mm partially threaded cannulated screw with a washer or a 3.0-mm headless compression screw (HCS; DePuy Synthes) was inserted along the guidewire. When sufficient compression and fixation stability were achieved and the ACJ reduction appeared satisfactory, the wound was closed.
In cases with minimal preoperative ACJ displacement, the temporary K-wire was removed before closure. However, when residual instability remained, the K-wire was left in situ with its tip exposed outside the skin, and the wound was sutured around it.
If adequate compression could not be achieved with screw fixation alone, the ACJ was first stabilized with a locking compression hook plate (clavicle hook plate; DePuy Synthes). After sufficient relaxation of the coracoclavicular ligament was ensured, screw fixation was repeated to obtain firm compression at the fracture site. Postoperative radiographs were obtained to assess fracture reduction and fixation (Fig. 1).
After the surgery, a Kenny-Howard brace was used for a duration of 6 weeks. During the second week post-surgery, patients began gentle passive forward flexion arm exercises. At 6 weeks, patients initiated passive range of motion exercises in all directions, as well as active mobilization. Patients were prohibited from carrying heavy objects for three postoperative months.
We retrospectively studied the records of 12 patients with coracoid process fractures associated with ACJ injury who underwent coracoid process fixation with or without ACJ stabilization procedure and could be followed up for more than 6 months. The surgical indications were coracoid process fractures associated with ACJ injury as observed in either simple radiography or three-dimensional computed tomography (CT). All fractures were evaluated with the anteroposterior (AP), Grashey and scapular Y view throughout the follow-up period. ACJ injury was evaluated using simple radiography according to Tossy classification [10]. All patients underwent CT scans to assess the pattern of fracture of the coracoid process according to Ogawa and Eyres classification [11,12]. Exclusion criteria encompassed (1) individuals without a minimum 6-month follow-up post-surgery, (2) those with a prior history of shoulder surgery, (3) participants with additional injuries necessitating separate surgical interventions, (4) individuals experiencing neurovascular injuries preoperatively, and (5) patients with preexisting (chronic) coracoid process nonunion.
The primary outcome was the radiographic union of the coracoid fracture. Secondary outcomes included time to union, visual analogue scale (VAS) pain score at final follow-up, University of California, Los Angeles (UCLA) shoulder score at final follow-up, device-related complications, and the need for and timing of implant removal. Baseline variables included age, sex, affected side, injury mechanism, associated injuries, and fracture/ACJ classifications (Tossy, Ogawa, Eyres).
In this study, union was determined as the point when cortical continuity was observed on one of the three planes of plain radiography (anteroposterior, Grashey, or scapular Y view), and when tenderness at the fracture site subsided. Coracoid fracture nonunion was defined as a fracture that had not united or mostly disconnected more than 6 months after surgery [6,7]. For all surgically treated patients, follow-up imaging was conducted at least up to 6 months postoperatively, with evaluations scheduled at 1, 2, 3, and 6-month intervals. Clinical outcomes were assessed based on the degree of pain and the restoration of daily functional activities. At the final follow-up, the following clinical outcome parameters were evaluated: VAS score and the shoulder rating scale of the UCLA score. Postoperative complications were also carefully assessed.
To reduce selection bias, we included all eligible patients during the study period who met the minimum follow-up criterion of six months. Measurement bias was minimized by using standardized radiographic views and predefined union criteria. Because fixation devices and ACJ stabilization were selected based on intraoperative stability and/or fracture characteristics, confounding by indication is possible; therefore, the results are reported descriptively without causal inference.
No sample size estimation was done because coracoid process fractures associated with ACJ injuries are rare; therefore, we included all eligible surgically treated cases during the study period.
Given the small sample size and noncomparative design, the analyses were primarily descriptive.
Results
A total of 12 patients with coracoid process fracture associated with the ACJ injury underwent open reduction and internal fixation using 3.5 mm cannulated screw with washer or 3.0 mm HCS. The average age of the patients was 51 years (range, 19‒74 years), and the average follow-up period was 15.7 months (range, 6‒70 months). Among the patients, 11 were men and one was a woman. The right and left sides were equal.
The fractures occurred due to various mechanisms, including simple falls, sports injury, motor vehicle accidents, being hit by a heavy object, and falls from height. Six patients had accompanying multiple rib fractures, and four of them had a hemopneumothorax. According to Tossy's classification [10] of ACJ injuries, there were five cases of type 2 and seven cases of type 3. According to Ogawa's classification [11] for coracoid process fracture, all cases were type 1, but according to Eyres' classification [12], there were four cases of type 3, five cases of type 4, and three cases of type 5 (Table 1).
Radiological union was achieved at a mean of 3 months (range, 1.5‒4 months) in all patients except one case. The time to removal of K-wire fixation for ACJ injuries was 1.7 months (range, 1.5–2 months) and for clavicle hook plates it was 5.9 months (range, 3–7.5 months), with K-wire removal occurring earlier. At the final follow-up, the average clinical scores were as follows: a VAS for pain of 1.5 (range, 0‒4) and a UCLA score of 30.9 (range, 28–35). Clinical outcomes in all patients were satisfactory [13] (Table 2).
No postoperative infections or neurovascular complications were observed in any of the patients. However, one patient experienced nonunion. The K-wire for ACJ fixation was removed at 6 weeks after the operation, and nonunion of the coracoid fixation was confirmed at the final follow-up of 6 months, but the patient's clinical outcome was good (Fig. 2).
Discussion
Coracoid fractures resulted from various mechanisms. Six patients had multiple rib fractures, and four had hemopneumothorax. ACJ injuries were classified as Tossy type II (n=5) or type III (n=7). All coracoid fractures were Ogawa type I, with Eyres classifications ranging from types 3 to 5. Radiologic union occurred in 11 of 12 cases, with a mean time to union of 3 months. K-wires were removed earlier than hook plates. The final VAS score was 1.5, and the UCLA shoulder score was 30.9. One case of nonunion retained functional use.
This study aimed to evaluate the usefulness of coracoid process fixation with or without ACJ stabilization procedure. Wignadasan et al. [6] reported that they achieved all bone union using a clavicle hook plate in six patients with concomitant coracoid base fracture and ACJ disruption, with a mean age of 39.8 years and a mean union time of 3.75 months. Ye et al. [7] showed that among 18 patients of coracoid process fractures combined with ACJ dislocation, bone union was achieved in 15 patients (83.3%) when only ACJ fixation using a clavicle hook plate was performed, and the mean age was 38 years. In our study, we demonstrated bone union in 11 out of 12 cases (91.7%) using coracoid process fixation with or without ACJ stabilization procedure for coracoid process fracture associated with the ACJ injury, with a mean age of 51 years and a mean union time of 3 months. Compared to the indirect reduction of the coracoid process fracture by performing ACJ fixation alone using a clavicle hook plate, the mean age was older and the bone union time and nonunion rate were lower in this study. We believe that coracoid process fixation with or without ACJ stabilization procedure may be considered a good alternative technique that appeared favorable than ACJ fixation alone.
In a comparative study of scaphoid screws, Shaw [14] reported that screws with larger head diameters and thread sizes showed greater compressive forces than headless screws. The mean maximum compressive forces were 12.8 kg for the 4.0 mm cancellous screw, 11.7 kg for the 3.5 mm cancellous screw, 7.6 kg for the 2.7 mm cortical screw, and 2.7 kg for the Herbert screw. In a comparative study of 6.5 mm Herbert screws and headed screws, Marshall et al. [15] showed that a cancellous lag screw with a washer was significantly better compressive force and pullout resistance than Herbert screw of same size. In this study, a 70-year-old patient (case 1) achieved bone union using only a cannulated screw with washer for coracoid fixation without acromioclavicular fixation. In cases of nonunion (case 12), a HCS was used for coracoid fixation. Coracoid fixation using a cannulated screw with a washer appears to be more beneficial than a headless screw in achieving sufficient fracture stability.
Ogawa et al. [3] reported that among 80 cases of coracoid base fracture with concurrent injuries, 62 cases underwent surgical treatment and achieved bone union in all cases, resulting in satisfactory results. Of these, 17 cases were coracoid base fracture associated with the ACJ injury, and the mean age was 36 years. Fixation with screw and washer for coracoid fractures and transacromial fixation with K-wire for the ACJ dislocation was performed. Rhee et al. [16] showed in a comparative study on ACJ stabilization using K-wires transfixation versus locking hook plates fixation in the treatment of acute ACJ dislocation that the locking hook plate provided more stable than the K-wires. In this study, deformation and loosening of K-wires occurred in patients with nonunion, and clavicle hook plates were thought to be more effective than K-wires in preventing nonunion.
In ACJ injury, Tossy classification grade III includes Rockwood classification type III and V, so this classification system applies to high-grade injuries [17]. In this study, Tossy classification grade 2 was observed in five of 12 cases. In coracoid process fractures associated with ACJ injuries, the Tossy classification, which is evaluated solely on plain radiography, is considered insufficient for assessing ACJ injuries. If a coracoid process fracture is confirmed, additional radiographic examinations, such as weighted, cross-arm AP, Zanca views, or magnetic resonance imaging (MRI), may be required.
Ye et al. [7] reported three cases of coracoid process nonunion that showed satisfactory functional outcomes despite nonunion. This study achieved satisfactory clinical results in all cases, including nonunion.
The present study has certain limitations that should be acknowledged. Firstly, the small number of included patients underscores the necessity for future comparative studies with a larger sample size and extended follow-up periods. Secondly, coracoclavicular and acromioclavicular ligament damage could not be confirmed because there was no MRI scan that could detect surrounding soft tissue damage. Thirdly, the absence of biomechanical studies is also a challenge that needs to be addressed. Fourth, it is important to note that the present study is retrospective. However, the strength of this study is that the surgeries were performed at a single center using the same surgical technique and products from the same company, although there were some differences in fixation devices.
We were able to achieve bony union in all but one case of coracoid process fracture associated with ACJ injury by fixation of the coracoid process with or without ACJ stabilization procedure. The use of a cannulated screw with washer for coracoid fixation appears to be more beneficial than a headless screw in achieving sufficient fracture stability. For ACJ stabilization procedures, clavicle hook plates have been considered more effective than K-wires in preventing nonunion. Tossy classification is based solely on plain radiography, which are considered insufficient to evaluate ACJ injuries, and further examination is considered necessary to definitively confirm the presence of an injury. Fortunately, satisfactory clinical results were achieved in all cases, including nonunion.
As a small, retrospective single-center case series, findings generalize mainly to surgically treated coracoid fractures with ACJ injury in similar trauma settings using CT-based evaluation and comparable implants/rehabilitation.
Coracoid process fixation with or without ACJ stabilization for coracoid process fractures associated with ACJ injury is an effective method that provides clinically beneficial fixation. If possible, a cannulated screw with a washer that has strong coracoid compression and pullout resistance and sufficient fracture stability is considered to be a good choice when performing both ACJ stablizationi and coracoid fixation. If possible, a clavicle hook plate that provides sufficient fracture stability as an ACJ stabilization is considered to be a good choice when performing both ACJ and coracoid process fixation.
-
Author contributions
Conceptualization: DS. Data curation: DS, SC. Formal analysis: BHK. Investigation: DS, SC, SK. Supervision: DS, BHK. Visualization: SC, BHK. Writing-original draft: DS, BHK. Writing-review & editing: DS, SC, SK, BHK. All authors read and approved the final manuscript.
-
Conflicts of interest
No potential conflict of interest relevant to this article was reported.
-
Funding
None.
-
Data availability
Contact the corresponding author for data availability.
-
Acknowledgments
None.
-
Supplementary materials
None.
Article Information
Fig. 1.
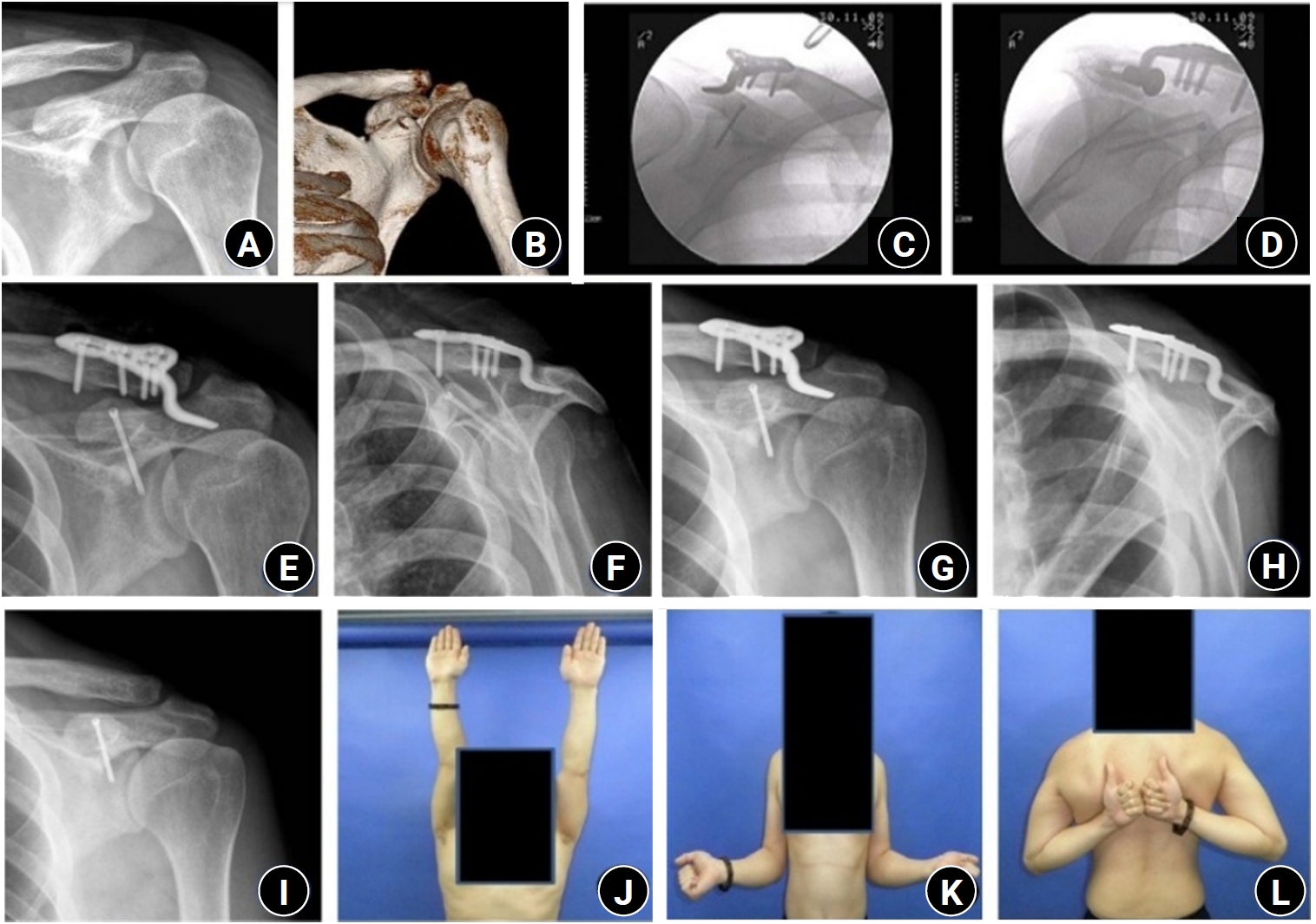
(A, B) Initial shoulder anteroposterior (AP) radiograph and three-dimensional computed tomography images of a 33-year-old male patient show a coracoid process fracture associated with an acromioclavicular joint (ACJ) injury. (C, D) Immediate postoperative C-arm images demonstrate open reduction and internal fixation using a 3.0-mm headless compression screw (HCS) for the coracoid process fracture and a clavicle hook plate for the ACJ injury. (E, F) Immediate postoperative shoulder AP and scapular Y radiographs show fixation using a 3.0-mm HCS for the coracoid process and a clavicle hook plate for the ACJ injury. (G, H) Postoperative 2-month AP and scapular Y radiographs show union of the coracoid process. (I–L) At the final follow-up, the patient demonstrated satisfactory radiographic and clinical outcomes, including full active range of motion.
Fig. 2.
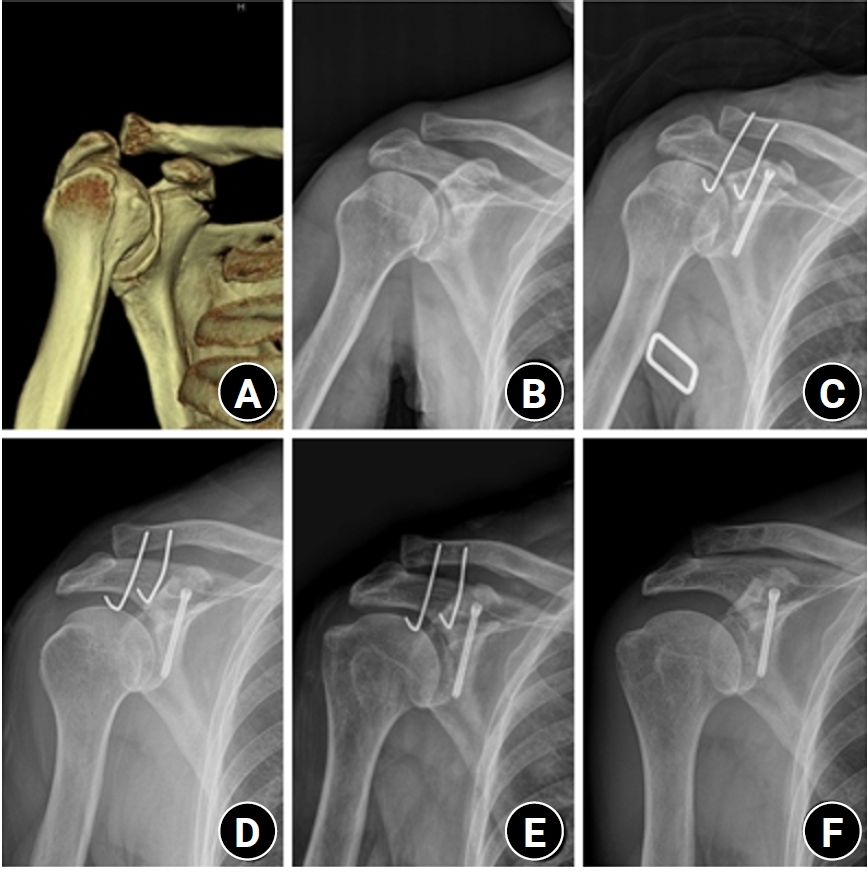
Three-dimensional computed tomography (A) and shoulder anteroposterior (AP) radiograph (B) of a 74-year-old male patient show a coracoid process fracture associated with an acromioclavicular joint (ACJ) injury. (C) A 3.0-mm headless compression screw was used for the coracoid process fracture, and two Kirschner (K)-wires were used for the ACJ injury. (D) Postoperative 2-week radiographs show K-wire deformation. (E) Postoperative 6-week radiographs show K-wire loosening. (F) Postoperative 6-month AP radiographs show nonunion of the coracoid process.
Table 1.
Summary of demographic data
Table 2.
The results of coracoid process fixation with or without acromioclavicular joint stabilization
- 1. Zlowodzki M, Bhandari M, Zelle BA, Kregor PJ, Cole PA. Treatment of scapula fractures: systematic review of 520 fractures in 22 case series. J Orthop Trauma 2006;20:230-3.ArticlePubMed
- 2. Lantry JM, Roberts CS, Giannoudis PV. Operative treatment of scapular fractures: a systematic review. Injury 2008;39:271-83.ArticlePubMed
- 3. Ogawa K, Matsumura N, Ikegami H. Coracoid fractures: therapeutic strategy and surgical outcomes. J Trauma Acute Care Surg 2012;72:E20-6.PubMed
- 4. Goss TP. Double disruptions of the superior shoulder suspensory complex. J Orthop Trauma 1993;7:99-106.ArticlePubMed
- 5. Ogawa K, Matsumura N, Yoshida A. Nonunion of the coracoid process: a systematic review. Arch Orthop Trauma Surg 2021;141:1877-88.ArticlePubMedPDF
- 6. Wignadasan W, Al-Obaedi O, Chambers A, Lee M, Rajesparan K, Rashid A. Concomitant coracoid base fracture and acromioclavicular joint disruption: a series of patients treated with a clavicle hook plate and review of the literature. J Orthop Surg (Hong Kong) 2022;30:10225536221139888.ArticlePubMedPDF
- 7. Ye CX, Guo YB, Zheng YH, et al. Treatment of coracoid process fractures combined with acromioclavicular joint dislocation using clavicular hook plate. J Shoulder Elbow Surg 2023;32:e548-55.ArticlePubMed
- 8. Kim KC, Rhee KJ, Shin HD, Kim DK, Shin HS. Displaced fracture of the coracoid process associated with acromioclavicular dislocation: a two-bird-one-stone solution. J Trauma 2009;67:403-5.ArticlePubMed
- 9. Bhatia DN. Orthogonal biplanar fluoroscopy-guided percutaneous fixation of a coracoid base fracture associated with acromioclavicular joint dislocation. Tech Hand Up Extrem Surg 2012;16:56-9.ArticlePubMed
- 10. Tossy JD, Mead NC, Sigmond HM. Acromioclavicular separations: useful and practical classification for treatment. Clin Orthop Relat Res 1963;28:111-9.PubMed
- 11. Ogawa K, Yoshida A, Takahashi M, Ui M. Fractures of the coracoid process. J Bone Joint Surg Br 1997;79:17-9.ArticlePubMedPDF
- 12. Eyres KS, Brooks A, Stanley D. Fractures of the coracoid process. J Bone Joint Surg Br 1995;77:425-8.ArticlePubMedPDF
- 13. Ellman H, Kay SP. Arthroscopic subacromial decompression for chronic impingement: two- to five-year results. J Bone Joint Surg Br 1991;73:395-8.ArticlePubMedPDF
- 14. Shaw JA. A biomechanical comparison of scaphoid screws. J Hand Surg Am 1987;12:347-53.ArticlePubMed
- 15. Marshall PD, Evans PD, Richards J. Laboratory comparison of the cannulated Herbert bone screw with ASIF cancellous lag screws. J Bone Joint Surg Br 1993;75:89-92.ArticlePubMedPDF
- 16. Rhee YG, Park JG, Cho NS, Song WJ. Clinical and radiologic outcomes of acute acromioclavicular joint dislocation: comparison of Kirschner’s wire transfixation and locking hook plate fixation. Clin Shoulder Elb 2014;17:159-65.Article
- 17. Williams G, Nguyen V, Rockwood C. Classification and radiographic analysis of acromioclavicular dislocations. Appl Radiol 1989;18:29-34.
References
Figure & Data
REFERENCES
Citations
Citations to this article as recorded by 
 ePub Link
ePub Link Cite
CiteSurgical outcomes of the coracoid process fracture associated with the acromioclavicular joint injury in Korea: a case series
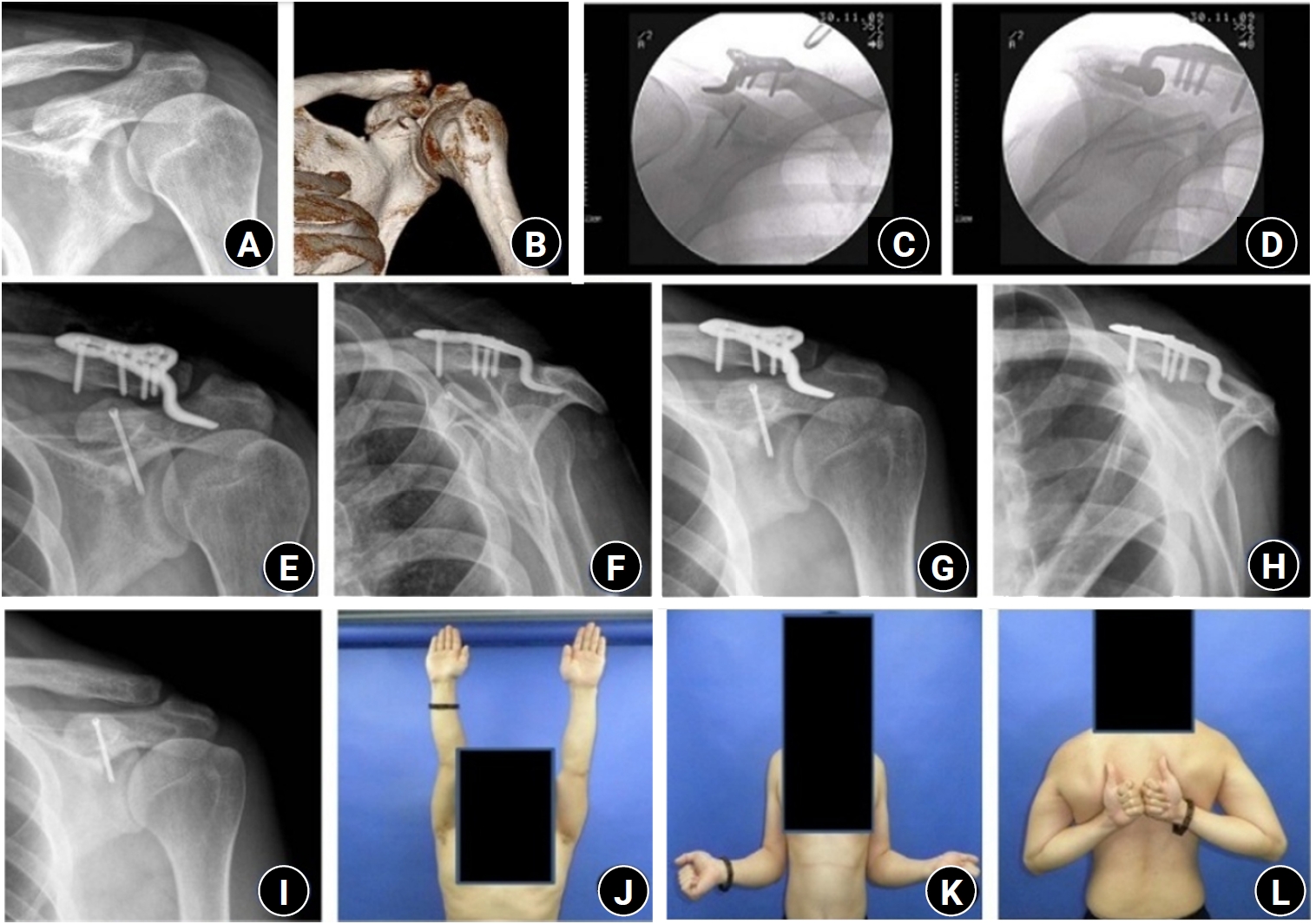
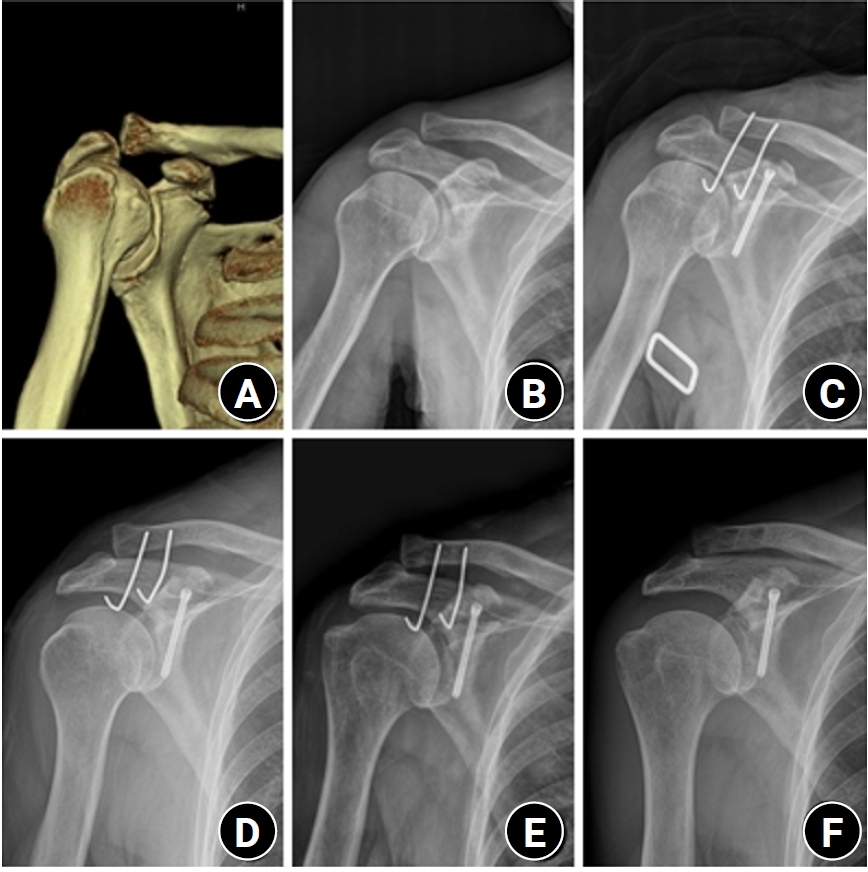
Fig. 1. (A, B) Initial shoulder anteroposterior (AP) radiograph and three-dimensional computed tomography images of a 33-year-old male patient show a coracoid process fracture associated with an acromioclavicular joint (ACJ) injury. (C, D) Immediate postoperative C-arm images demonstrate open reduction and internal fixation using a 3.0-mm headless compression screw (HCS) for the coracoid process fracture and a clavicle hook plate for the ACJ injury. (E, F) Immediate postoperative shoulder AP and scapular Y radiographs show fixation using a 3.0-mm HCS for the coracoid process and a clavicle hook plate for the ACJ injury. (G, H) Postoperative 2-month AP and scapular Y radiographs show union of the coracoid process. (I–L) At the final follow-up, the patient demonstrated satisfactory radiographic and clinical outcomes, including full active range of motion.
Fig. 2. Three-dimensional computed tomography (A) and shoulder anteroposterior (AP) radiograph (B) of a 74-year-old male patient show a coracoid process fracture associated with an acromioclavicular joint (ACJ) injury. (C) A 3.0-mm headless compression screw was used for the coracoid process fracture, and two Kirschner (K)-wires were used for the ACJ injury. (D) Postoperative 2-week radiographs show K-wire deformation. (E) Postoperative 6-week radiographs show K-wire loosening. (F) Postoperative 6-month AP radiographs show nonunion of the coracoid process.
Fig. 1.
Fig. 2.
Surgical outcomes of the coracoid process fracture associated with the acromioclavicular joint injury in Korea: a case series
| Patient no. | Age (yr) | Sex | Affected side | Injury mechanism | Classification | Combined injury | Follow-up (mo) | ||
|---|---|---|---|---|---|---|---|---|---|
| Tossy type | Ogawa type | Eyres type | |||||||
| 1 | 70 | M | Lt | MVA | 3 | 1 | 5 | MRF, HPT | 17 |
| 2 | 52 | M | Rt | Hit by mass | 3 | 1 | 5 | MRF, HPT | 70 |
| 3 | 56 | M | Lt | MVA | 2 | 1 | 5 | MRF, HPT | 7 |
| 4 | 33 | M | Lt | MVA | 2 | 1 | 4 | - | 18 |
| 5 | 45 | M | Lt | Sports injury | 3 | 1 | 4 | - | 8 |
| 6 | 56 | F | Lt | Simple fall | 3 | 1 | 4 | - | 7 |
| 7 | 51 | M | Rt | Hit by mass | 2 | 1 | 4 | MRF, HPT | 9 |
| 8 | 19 | M | Rt | MVA | 2 | 1 | 3 | MRF | 12 |
| 9 | 43 | M | Rt | Sports injury | 3 | 1 | 3 | - | 7 |
| 10 | 64 | M | Lt | Fall from height | 3 | 1 | 3 | MRF | 8 |
| 11 | 49 | M | Rt | Simple fall | 3 | 1 | 3 | - | 19 |
| 12 | 74 | M | Rt | Fall from height | 2 | 1 | 4 | - | 6 |
| Patient no. | Union (mo) | Coracoid fixation | Acromioclavicular fixation | Time to removal (mo) | VAS score | UCLA score | UCLA grade | Complication |
|---|---|---|---|---|---|---|---|---|
| 1 | 3 | Cannulated screw | - | - | 0 | 32 | Good | |
| 2 | 4 | Cannulated screw | K-wire | 2 | 0 | 32 | Good | |
| 3 | 4 | HCS | K-wire | 1.5 | 2 | 30 | Good | |
| 4 | 2 | HCS | Hook plate | 7.5 | 0 | 35 | Excellent | |
| 5 | 3 | HCS | Hook plate | 5 | 0 | 33 | Good | |
| 6 | 4 | HCS | Hook plate | 6.5 | 2 | 29 | Good | |
| 7 | 2 | HCS | Hook plate | 3 | 2 | 29 | Good | |
| 8 | 1.5 | Cannulated screw | Hook plate | 11 | 0 | 31 | Good | |
| 9 | 4 | HCS | Hook plate | 7 | 2 | 32 | Good | |
| 10 | 3 | HCS | Hook plate | 4.5 | 2 | 31 | Good | |
| 11 | 2.5 | HCS | Hook plate | 3 | 4 | 29 | Good | |
| 12 | - | HCS | K-wire | 1.5 | 4 | 28 | Good | Nonunion at 6 mo |
Table 1. Summary of demographic data
M, male; Lt, left; MVA, motor vehicle accident; MRF, multiple rib fractures; HPT, hemopneumothorax; Rt, right; F, female.
Table 2. The results of coracoid process fixation with or without acromioclavicular joint stabilization
VAS, visual analogue scale; UCLA, University of California, Los Angeles; HCS, headless compression screw; K-wire, Kirschner wire.

