 E-submission
E-submission TOTA
TOTA TOTS
TOTS
Articles
- Page Path
- HOME > J Musculoskelet Trauma > Volume 38(3); 2025 > Article
-
Original Article
- Computational simulation of coracoclavicular screw insertion through the superior distal clavicular plate for clinical applications in Korean cadavers
-
Hyung-Lae Cho, MD1
 , Ji Han Choi, MD1, Se-Lin Jeong, BS2, Gu-Hee Jung, MD2,3
, Ji Han Choi, MD1, Se-Lin Jeong, BS2, Gu-Hee Jung, MD2,3 -
Journal of Musculoskeletal Trauma 2025;38(3):143-151.
DOI: https://doi.org/10.12671/jmt.2025.00122
Published online: July 22, 2025
1Department of Orthopedic Surgery, Good Samsun Hospital, Busan, Korea
2Department of Orthopedic Surgery, Gyeongsang National University Changwon Hospital, Gyeongsang National University College of Medicine, Changwon, Korea
3Institute of Medical Sciences, Gyeongsang National University, Jinju, Korea
- Correspondence to: Gu Hee Jung, MD Department of Orthopedic Surgery, Gyeongsang National University Changwon Hospital, 11 Samjeongja-ro, Seongsan-gu, Changwon 51472, Korea Tel: +82-55-214-3822 Email: jyujin2001@hotmail.com
• Received: February 19, 2025 • Revised: April 17, 2025 • Accepted: May 15, 2025
© 2025 The Korean Orthopaedic Trauma Association
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/4.0/) which permits unrestricted noncommercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
- 973 Views
- 23 Download
Abstract
-
Background The study was conducted to determine the practical area for inserting the coracoclavicular (CC) screw through the plate by analyzing three-dimensional (3D) shoulder models featuring virtually implanted, actual-size plates and screws.
-
Methods Ninety cadaveric shoulders (41 males and 49 females) underwent continuous 1.0-mm slice computed tomography scans. The data were imported into image-processing software to generate a 3D shoulder model, including the scapula and clavicle. The overlapping area between the clavicle and the horizontal portion of the coracoid process (horizontal portion_CP) was analyzed in the cranial view. A curved pelvic recon plate was virtually placed on the upper surface of the distal clavicle, and an actual-size (3.5 mm) CC screw was inserted through the plate.
-
Results The distal clavicle directly overlapped with the horizontal portion_CP in the vertical direction. The overlapping area was sufficient to place the 3.5 mm and 4.5 mm-sized screws. In all shoulder models, the CC screw could be inserted through the plate into the vertical direction, with an average length of 35.5 mm (range, 26.2–62.5 mm; standard deviation, 1.2 mm). In 87 models, the CC screw was inserted through the third hole from the lateral end of the plate. Two models were inserted through the second hole, and one model through the fourth hole.
-
Conclusions The upper surface of the clavicle has sufficient overlapping area to place CC screws through the plate in the vertical direction in the corresponding hole. Supplemental CC screw fixation through the plate can be performed without additional or special equipment.
-
Level of evidence IV.
Introduction
Surgical treatment of distal clavicular fractures can be challenging because of the deforming forces on the proximal clavicle and characteristically small distal fragments that limit quality fixation. Numerous surgical options have been reported. These have yielded varying results, with diverse rates of associated complications and reoperation [1]. No consensus has been reached on the optimal treatment, especially in Neer type IIB fractures. In managing an unstable distal clavicular fracture, if fixation of the distal fragment is judged to be inadequate, fixation may need to be augmented using a hook plate with fixation under the acromion or supplemental coracoclavicular (CC) fixation combined with the superior distal clavicular plate fixation to prevent superior migration of the proximal fragment [2-4].
Considering the complications related with hook plate fixation for the distal clavicular fractures [5-7], although contentious, supplemental CC fixation combined with the superior plating has more advantages and has been performed using various options when there is insufficient bony purchase in the distal fragment with multiple screws [8-12]. Among the various options, supplemental CC screw fixation through the plate could be performed into the coracoid process without additional implant and instruments whenever needed. However, practically, most surgeons have been concerned with the proper and safe screw trajectory into the coracoid process due to the complicated three-dimensional (3D) anatomy. Although the horizontal portion of coracoid process (horizontal portion_CP) has long been used as the osseous site to achieve the fixation constructs including the CC ligament reconstruction, Bosworth screw fixation, and others, there was no detailed information on safe zone and ideal entry point for screw fixation on the upper surface of clavicle. Therefore, the primary purpose of this computational study was to verify the practical area for inserting the CC screw through the plate and introduce the landmark for clinical application by analyzing the 3D shoulder models featuring virtually implanted, actual size plate and screws.
Methods
Digital images of the Korean human body were obtained from the Korean Institute of Science and Technology Information (KISTI) and used under an official agreement. As this study utilized anonymized cadaveric CT data, additional institutional review board approval and informed consent were not required.
Adult cadavers (n=105) who underwent continuous 1.0 mm slice computed tomography (CT) scans (Pronto) in the supine position were included. None of the cadavers had scapular and clavicular problems based on the analysis of medical records. CT data in Digital Imaging and Communications in Medicine format were imported into Mimics software (Materialise Interactive Medical Image Control System, Materialise) to reconstruct the 3D shoulder models including the scapula and clavicle.
After obtaining a 3D shoulder model, the straight distance on the upper surface of clavicle was measured using the distant measuring tool of the Mimics software. The distance averaged 141.6 mm (range, 120.7–163.5 mm; standard deviation [SD], 11.2) (Fig. 1). The transparency mode was controlled to differentiate the overlapping area between the upper clavicular surface and the horizontal portion_CP in the cranial view. The straight distance on clavicle between the elevated ridge of horizontal portion_CP and lateral end of clavicle was measured on the upper surface of clavicle and defined as distance_CP (Fig. 1). For the computer-assisted simulation of CC screw fixation through the plate, a virtual 3D model of curved pelvic recon plate (Depuy-Synthes, GmbH) and 3.5 mm cortical screw were created using a 3D sensor (Comet5, Carl Zeiss) in actual size, and placed on the upper surface of distal clavicle using Mimics as with the distal clavicular superior plate fixation (Fig. 2). The ideal position of curved pelvic recon plate (plate) was defined as when the lateral end of plate corresponded to the lateral end of clavicle, the plate was centrally placed on the upper surface of clavicle in the cranial view, and the plate fit well in the anteroposterior (AP) view of the shoulder. After the definitive position of plate was fine-tuned and verified by an experienced surgeon (GHJ), the mutual location of plate holes, horizontal portion_CP and its elevated ridge, and medial border of coracoid process was assessed by controlling the rotation of shoulder model in the cranial and caudal views of the shoulder model. Virtual CC screw fixation through the plate with purchase of the horizontal portion_CP was performed using the Mimics software with a 3.5 mm cortical screw. The corresponding hole and relationship with the adjacent structure were identified.
IBM SPSS ver. 23.0 (IBM Corp.) was used and statistical significance was set at P<0.05. The univariate and multivariate analyses were performed using logistic regression and linear regression models.
Results
Fifteen cadavers were not enrolled due to poor image quality. The 90 enrolled adult cadavers (41 males and 49 females) had a mean age of 52.9 years (range, 22–60 years; SD, 2.8) and a mean height of 160.5 cm (range, 146–176 cm; SD, 7.8). On the cranial view of the clavicle, the upper surface of the distal clavicle overlapped with the horizontal portion_CP in a crossed direction. The overlapping area was sufficient to place the 3.5 mm and 4.5 mm screws in all models (Fig. 3). After magnifying and freely rotating the 3D model, the elevated ridge was easily identified just medial to the ascending portion and was roughly placed in the central area of upper surface of clavicle. Distance_CP averaged 30.6 mm (range, 23.0–42.0 mm; SD, 1.1) and was statistically significant just with the clavicular length (P<0.001).
Compared with the virtually placed plate in the ideal position, on the cranial view, the elevated ridge of 51 models was centrically matched with a central point of plate hole (third hole in 48 models, second hole in two models, and fourth hole in one model) and 39 models, eccentrically with the third hole (Table 1). On an AP view of the shoulder, the intersection point between the imaginary vertical line from the medial border of coracoid process and distal clavicle was always placed in the medial to the third hole of plate regardless of the degree of horizontal rotation of scapula (Fig. 4). On the lower surface of clavicle, the conoid tubercle was in accord with the possibility of three screws fixation in all models (Fig. 5). The findings clearly demonstrated that the distal clavicular fragment, which corresponded to the medial border of coracoid process and conoid process, had fixability of at least three screws through the plate.
In all shoulder models, the CC screw could be inserted through the plate into the horizontal portion_CP just in the vertical direction. The average length was an average 35.5 mm (range, 26.2–62.5 mm; SD,2). The CC screw of 87 models was inserted through the third hole from the lateral end of the plate. Two models were through the second hole and through the fourth hole in one model (Fig. 6). Among 87 models, ten had sufficient overlapping area to place the two vertical and parallel CC screws through the third and fourth holes, which were assigned as the two screws model.
Ten models with two vertical CC screws were exclusively males and displayed statistically significant clavicular length (P<0.001) and distance_CP (P<0.001). Based on the independent-sample T-test, the two groups were statistically different (P<0.001) (Table 2). When the Hosmer-Lemeshow test for goodness of fit was performed with the possibility of two CC screw fixation through the plate, the value of χ2 was 2.291 (P=0.971). So, the logistic regression model was statistically significant. Among the anatomic variables, the sex (P=0.001), clavicular length (P<0.001), and distance_CP (P<0.001) were statistically significant. By multiple logistic regression model analysis, distance_CP was the only variable with a statistical significance (P<0.001). Receiver operating characteristic curve analysis using the distance_CP revealed an area under the curve of 0.976 (95% confidence interval [CI], 0.946–1.00), which indicated the suitability of distance_CP to predict the possibility of two CC screw placement through plate. The cut-off value of distance_CP was 33.6 mm (sensitivity, 0.90; specificity, 0.91). If distance_CP exceeded 33.6 mm, the distal clavicle would likely have sufficient osseous site on the upper clavicular surface for placing the two CC screws inside the horizontal portion_CP.
Discussion
For unstable distal clavicular fractures, the horizontal portion_CP has been used for the osseous site to achieve supplemental fixation constructs including the CC ligament surgeries, CC screw fixation, suture anchor insertion, and others [8-12]. However, these techniques need an additional procedure and implantation techniques for coracoid fixation, and are expensive. If the supplemental fixation is performed just by placing a screw through the plate on the upper surface of the clavicle, this fixation construct might be so convenient and useful in some injuries including poor bone quality and distal clavicular fractures with unexpected comminution [13,14]. Presently, we introduce the practical landmark and safe area for placing the CC screw through the plate and have identified the information for clinical application by virtually placing actual size plate and screws. This 3D anatomy study has a descriptive character, since the non-fractured clavicle of cadavers was analyzed. However, we anticipate that the results have practical value for several reasons: First, to the best of our knowledge, this is the only computational simulation study that has used actual size (3.5 mm) CC screw and plate. Second, the use of Mimics 3D rendering software to allow free 360° rotation with magnification in any plane allowed verification of the overlapping area (safe zone) and direct comparison with the plate holes. Third, it was clearly demonstrated that the CC screw through the plate could be inserted just by vertical direction in all models without additional procedure and special equipment.
Owing to the complications related with hook plate fixation for the distal clavicular fractures [5-7], the precontoured superior locking plating has been performed and good outcomes have been reported [4,15]. But, in practice, some distal clavicular fracture showed the unexpected comminuted fragments when using the open method, and is difficult to achieve sufficient bony purchase [16]. In these circumstances, despite some controversy, supplemental CC fixation combined with plate fixation has been viewed as the most preferred of the various options [17-19]. Unlike other techniques, the supplemental CC screw fixation through the plate can theoretically be performed without additional devices, implants, and instruments, and can be done as the occasion requires. However, we are not aware of anatomical information concerning the ideal entry point and safe zone. Although Andersen et al. [4] reported the advantages on the CC screw through the plate for distal clavicular fracture, they did not describe the technical reference. Tiefenboeck et al. [14] claimed that the clavicle was drilled by aiming the guide wire centrally towards the base of the coracoid process after manually identifying the coracoid tip. However, our computational simulation clearly found that the direct palpation of coracoid process was not required in this supplemental CC screw fixation technique. Once the clavicle was drilled through the hole of ideally-placed plate and aimed vertically, the CC screw of all models could purchase the osseous site around the elevated ridge of the horizontal portion_CP without an additional step. Even 10 models of male cadavers had sufficient overlapping area to place the two vertical and parallel CC screws through the third and fourth plate holes. Thus, in the unplanned and extemporary circumstance in which the lateral fragment was unexpectedly comminuted and even osteopenia in elderly patients and so did not seem to achieve the sufficient bony purchase, supplemental CC screw fixation through the plate could be undertaken. As well, since the simulated CC screw purchased the osseous site around the elevated ridge in which the trapezoid ligament was attached, anatomic reduction of the CC space might be achieved.
Considering that supplemental CC screw fixation through the plate is usually performed with fluoroscopic guidance, the intraoperative landmark or guideline might be important to verify the safe screw trajectory and prevent the neurovascular complications in practice. Since the scapula is not oriented in a true coronal plane, but lies in a coronal oblique plane, radiographic imaging of the entire coracoid process is difficult [20,21]. Although several radiographic views have been described, none can visualize each coracoid process in its entirety [21]. By our analysis of overlapping area on the cranial view, the practical landmark for CC screw insertion to place the plate centrally on the upper surface of clavicle was identified. AP view of the shoulder revealed the lack of necessity to aim the drill bit towards the base of the coracoid process to achieve the osseous purchase of the elevated ridge, since the CC screw could be inserted through the plate into the horizontal portion_CP in the vertical direction. Once the drill bit was placed just lateral to the ascending portion of coracoid process, there was an obvious screw purchase to the horizontal portion_CP in the AP view, regardless of the patient’s position and radiographic projection. Therefore, the imaginary vertical line from the medial border of the coracoid process could be used as the intraoperative guideline without special equipment. If the fracture line is medial to the intersection point between the clavicle and the imaginary vertical line during the fluoroscopic surgery, it would mean the lateral fragment had a fixability of at least three screws. Therefore, the imaginary vertical line might be useful for preoperative planning and the intraoperative procedure. Presently, the CC screw of 87 models (97%) was inserted through the third hole from the lateral end of the plate, which was easily identified by comparison between the plate and the imaginary vertical line. Henceforth, the corresponding hole for CC screw could be verified just by intraoperative fluoroscopic view (Fig. 4). These informative landmarks could be utilized to classify the fracture and choose the implant based on the fixability of distal clavicular fragments (Fig. 7).
Through this study, we found theoretically that 10 models (11%) had sufficient overlapping area to place the two vertical and parallel CC screws through the third and fourth plate holes. If the distance_CP exceeded 33.6 mm, the overlapping area would likely be sufficient osseous site for placement of two CC screws. However, although the distance_CP variable was utilized as preoperative radiologic marker, it could not be identified in the conventional CT scans. Thus, preferentially, the relationship between distance_CP and the imaginary vertical line had to be verified in the AP view of the shoulder. By free 360° rotations with magnification in any plan of 3D shoulder model, the elevated ridge was easily recognizable as the convex surface just after the ascending portion. Considering that the lateral end of the distal clavicle and elevated ridge of the horizontal portion_CP were conveniently localized during the operation, distance_CP might be of practical value in predicting the possibility of two vertical CC screws and locating the corresponding hole for the supplemental CC screw in the various kinds of precontoured distal clavicular plate (Fig. 8).
This computational simulation study has several fundamental limitations. First, the indication of CC screw fixation through the plate was not clear, because the biomechanical and clinical advantages on CC screw fixation has not been proven. Second, considering the variables were manually measured, interobserver errors could occur. Third, owing to the small number of enrolled clavicles, our results cannot be generalized to all Asian people. Nevertheless, the findings indicate that supplemental CC screw fixation through the plate is an entirely safe and practically easy way to be placed without additional procedure and special equipment. Further studies on the clinical outcomes of supplemental CC screw through the plate and comparative study with other implant to augment fixation in distal clavicular fracture should be conducted in future.
Conclusions
This is the only study verifying the safe zone/trajectory, intraoperative landmark of vertical line, fixability of three screws on the distal clavicular fragment by simulating the supplemental CC screw through the plate in actual size. Considering the topographic features of overlapping area between the clavicle and horizonal portion, supplemental CC screw insertion through the plate could be placed safely over the horizontal portion_CP in the vertical direction in the corresponding hole without additional preparation, whenever the occasion requires.
-
Author contributions
Data curation: JHC, SLJ. Formal analysis: HLC. Methodology: HLC. Visualization: SLJ, GHJ. Writing-original draft: SLJ, GHJ. Writing-review & editing: HLC, JHC, GHJ. All authors read and approved the final manuscript.
-
Conflicts of interest
None.
-
Funding
None.
-
Data availability
Contact the corresponding author for data availability.
Article Information
Fig. 1.
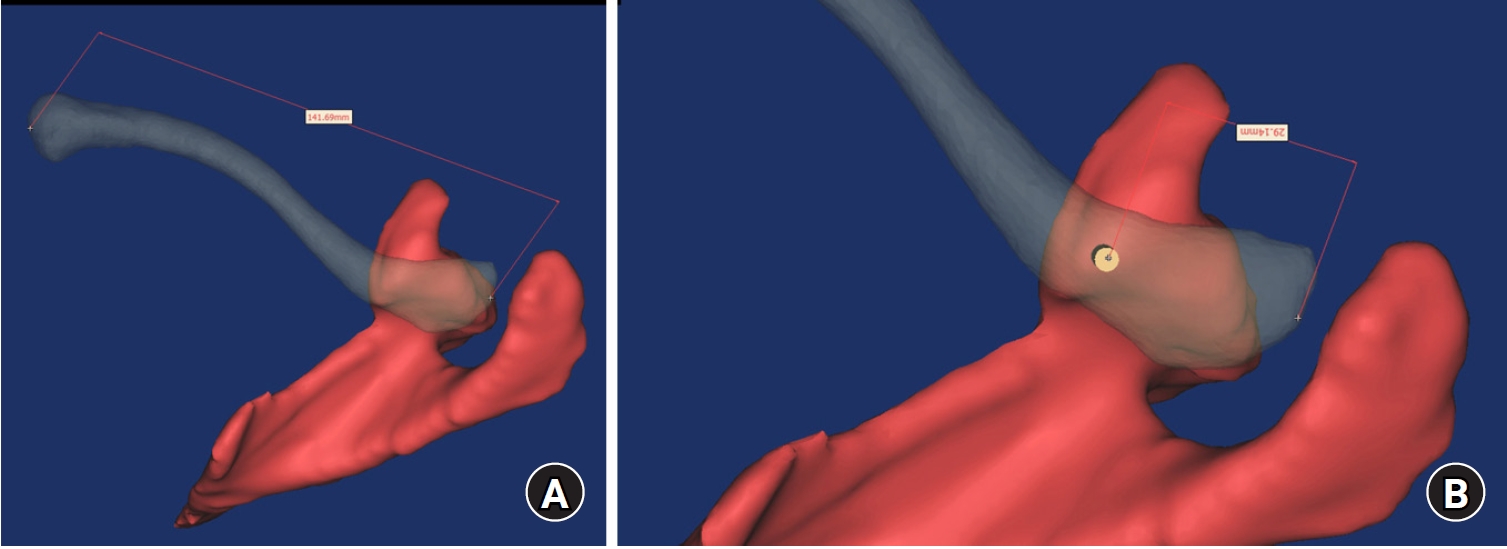
Mimics software was used to reconstruct 3-dimentional models of the scapula and clavicle, and the transparency mode was controlled to identify the overlapping area between the clavicle and the coracoid process. The straight distance of the clavicle (A) and the distance between the lateral end of the clavicle and the elevated edge of the coracoid process (B) were measured using software.
Fig. 2.
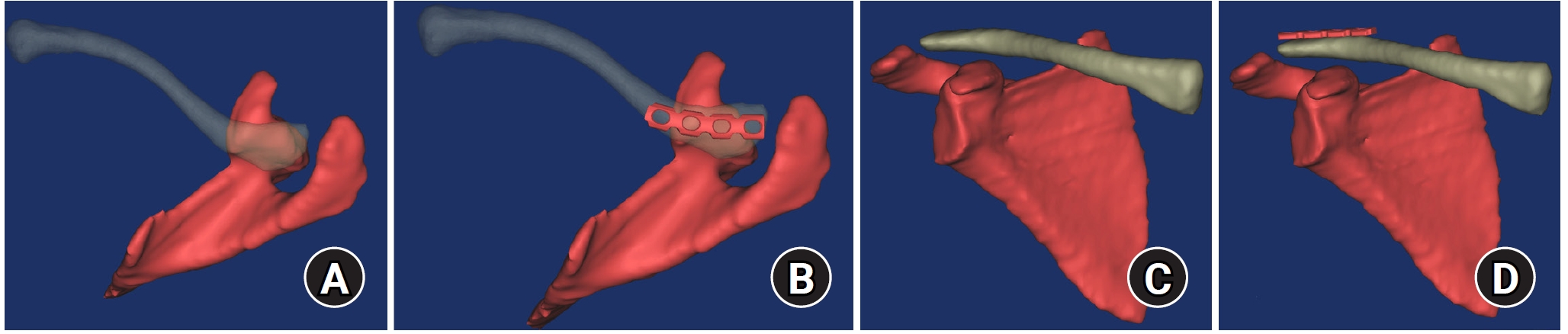
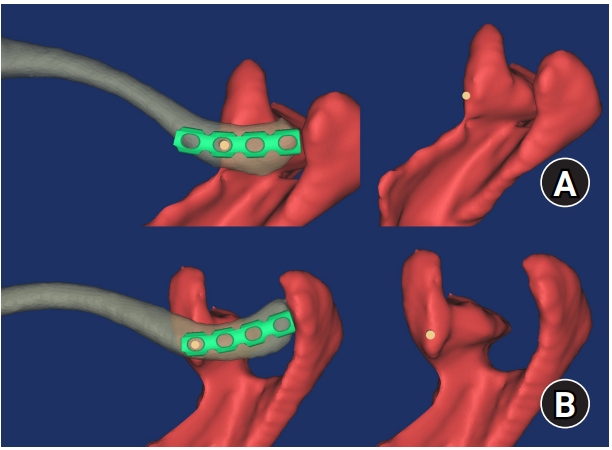
The optimally positioned pelvic recon curved plate was defined as the central area being on the upper surface of the clavicle in the cranial view (A, B) and well fitted in the anteroposterior view (C, D).
Fig. 3.
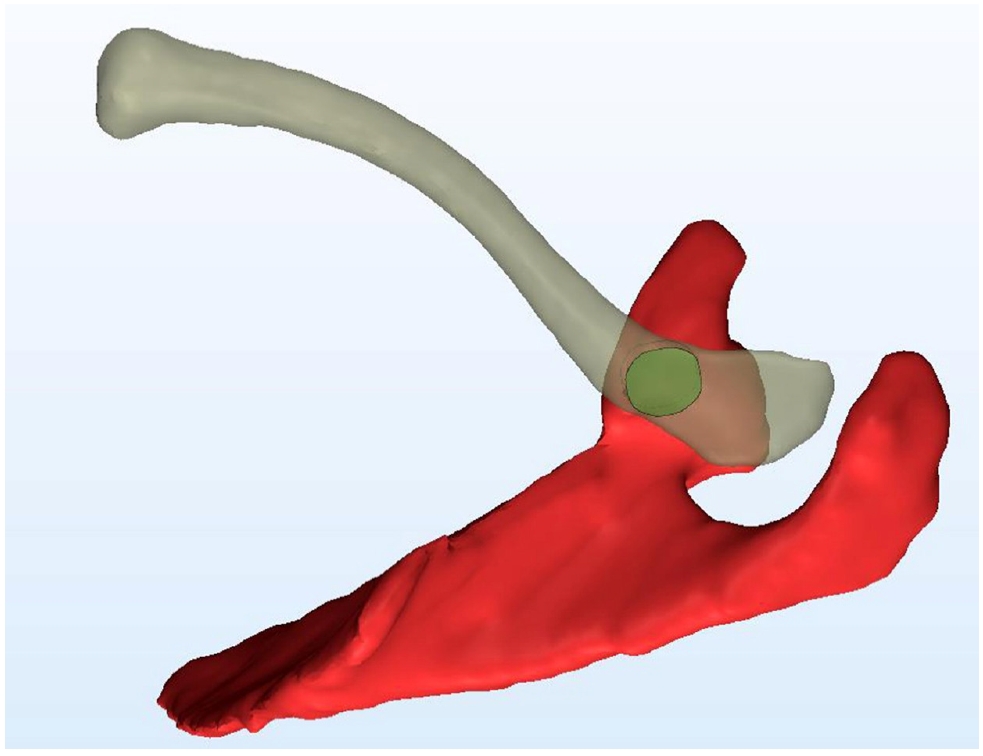
On the cranial view of the clavicle, the upper surface of distal clavicle overlapped with the horizontal portion_coracoid process in a crossed direction. The overlapping area was located around the elevated edge and was sufficient to place the 3.5-mm and 4.5-mm screws.
Fig. 4.
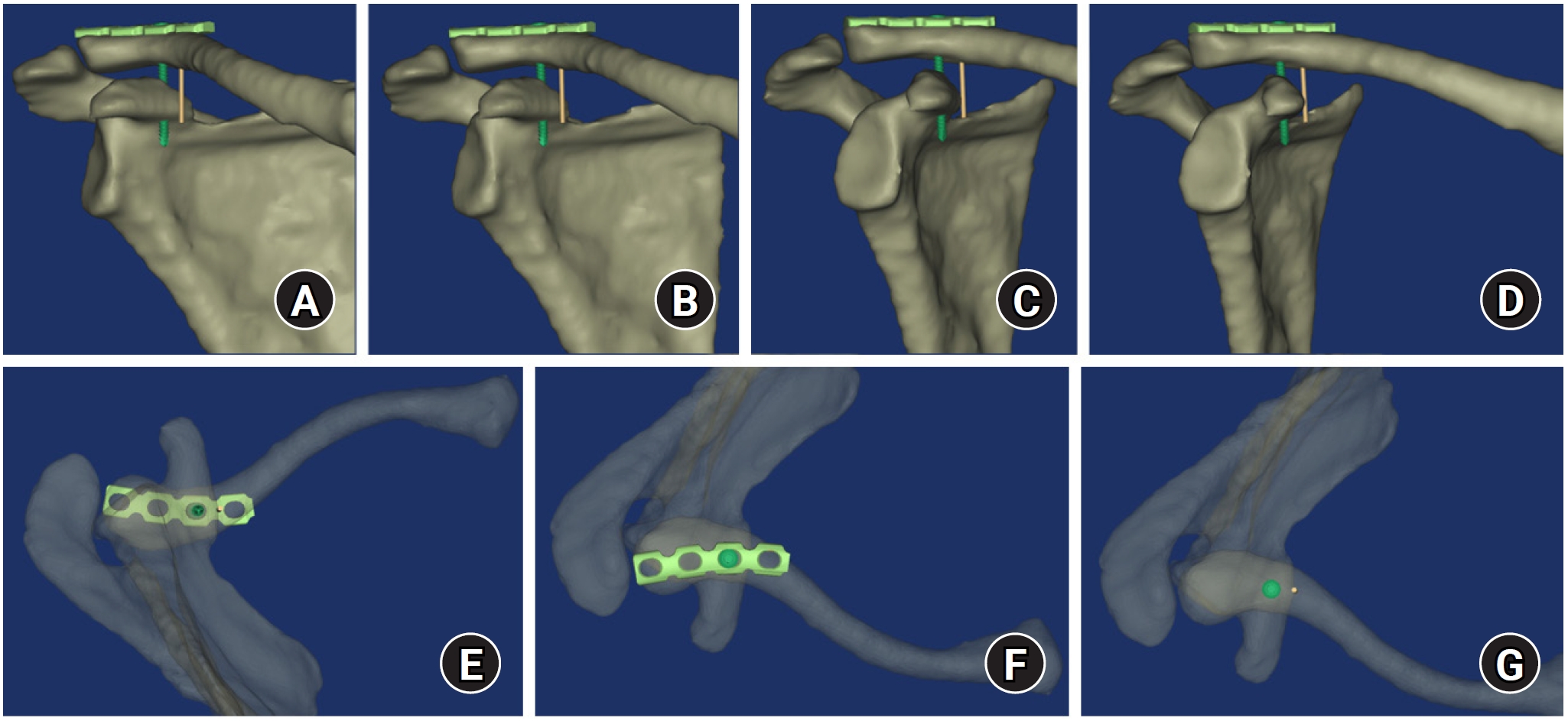
On an anteroposterior view of the shoulder, the intersection point between the imaginary vertical line from the medial border of coracoid process and distal clavicle was always placed medial to the third hole of the plate regardless of the degree of horizontal rotation of the scapula (A–D). In the cranial view, the imaginary vertical line corresponded to the medial border of the overlapping area (E–G).
Fig. 5.
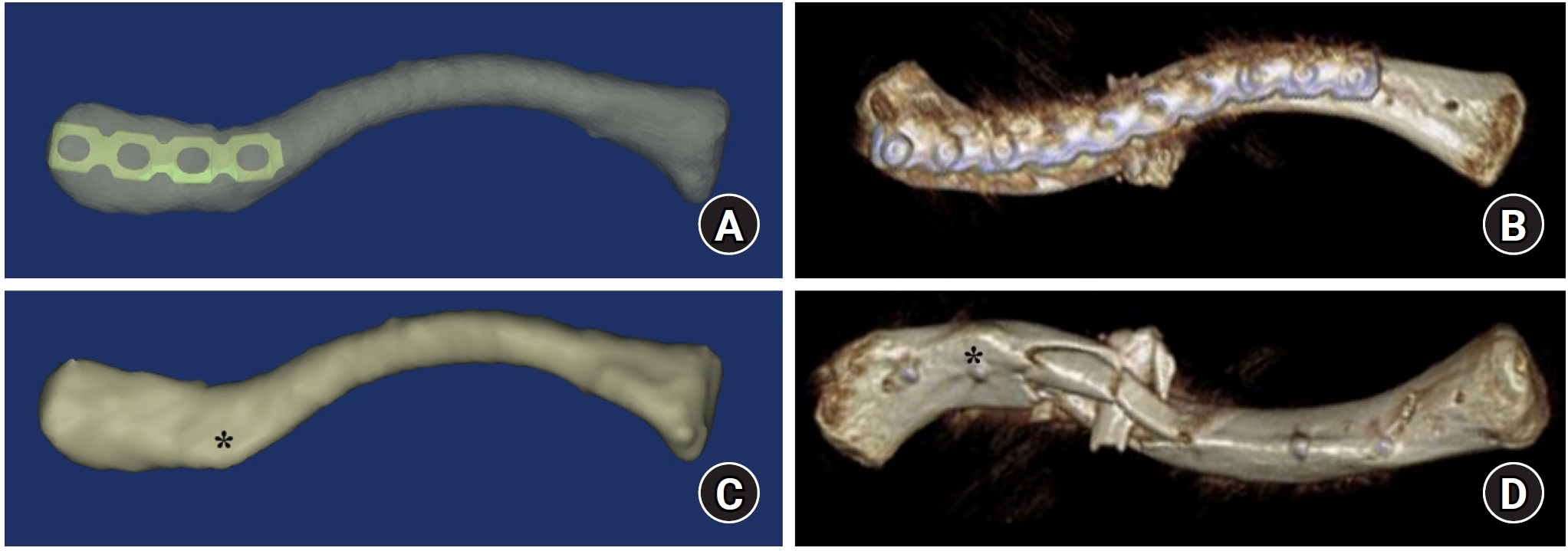
On a caudal view of the clavicle, the conoid tubercle (asterisk) of the lower surface of the clavicle was in accordance with the possibility of three-screw fixation in all models (A, B). In the comminuted clavicular fracture, which was fixed with a pelvic curved recon plate through the bridge plating technique, a postoperative biplanar 3-dimentional image shows that the lateral fragment lateral to the conoid tubercle (asterisk) could be fixed with three screws (C, D).
Fig. 6.
Supplemental coracoclavicular screw fixation through the plate was inserted from the second hole in two models (A) and through the fourth hole in one model (B).
Fig. 7.
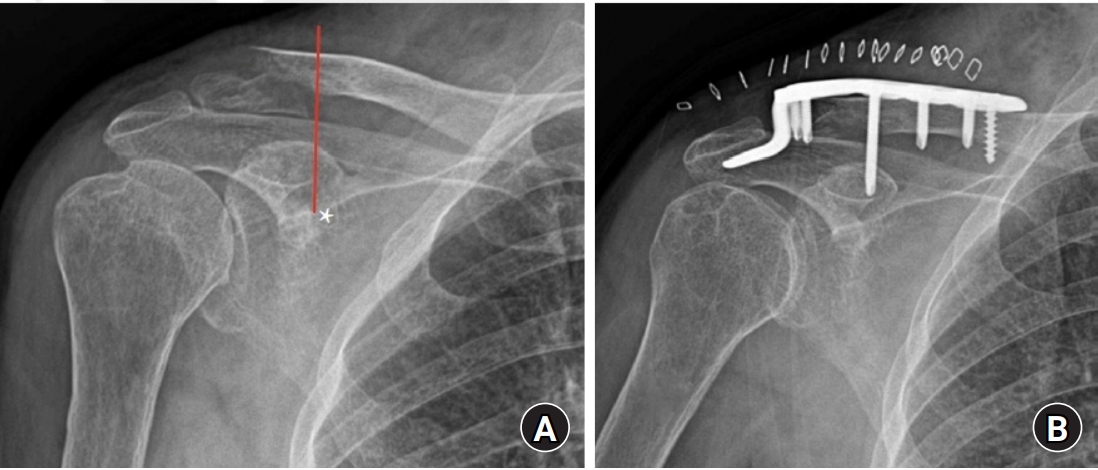
An imaginary vertical line (asterisk) of preoperative radiograph could be utilized to classify the fracture and choose the implant based on the fixability of distal clavicular fragments (A, B).
Fig. 8.
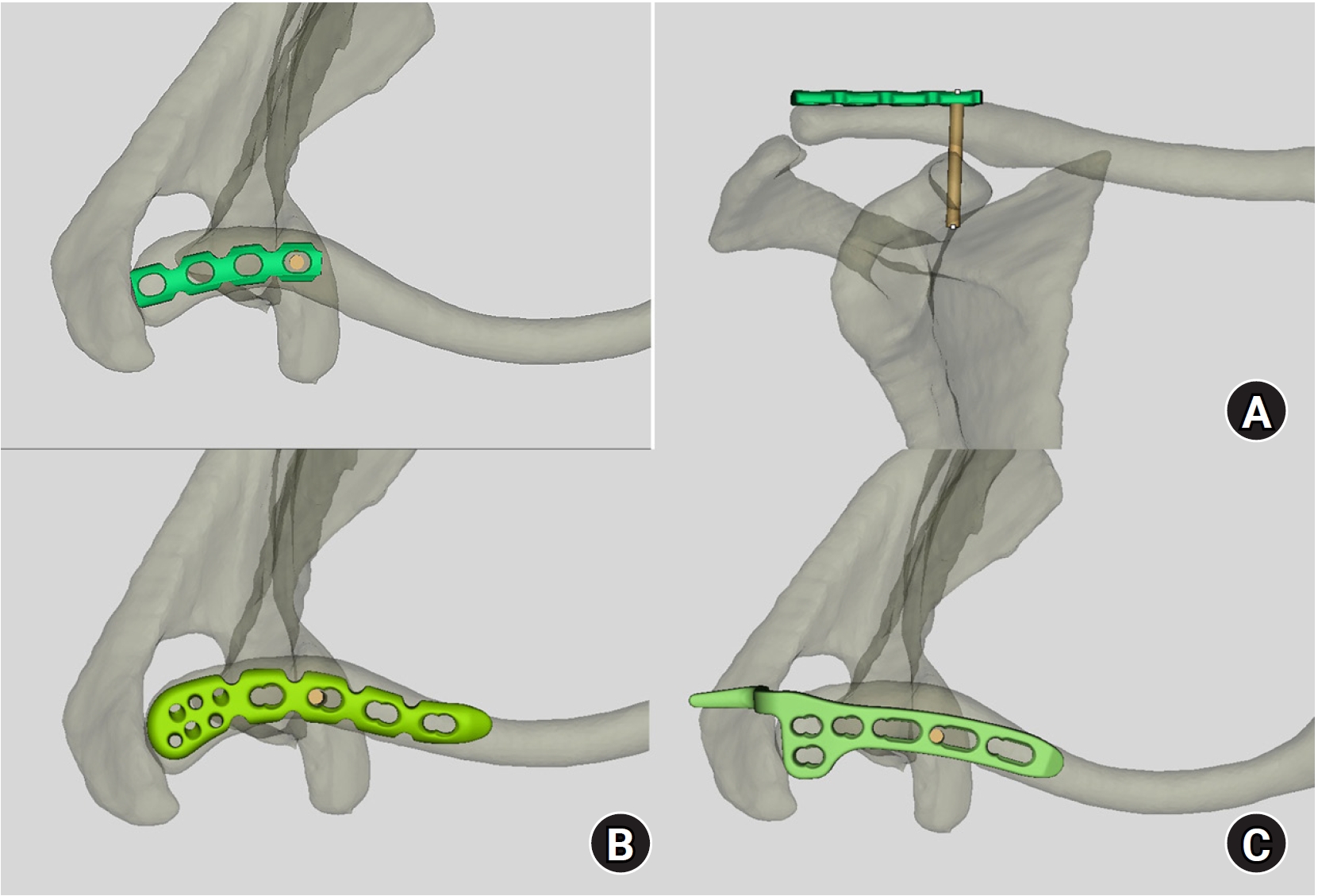
Considering the convex surface of horizontal portion_coracoid process and imaginary vertical line, the corresponding hole for the supplemental coracoclavicular screw through the plate could be fixed in the various kinds of precontoured distal clavicular plate: (A) pelvic curved recon plate, (B) precontoured distal clavicular plate, and (C) distal clavicular hook plate.
Table 1.
Differences in distance_CP
Table 2.
Comparison of two groups
| Group | Mean | Standard deviation | T | P-value |
|---|---|---|---|---|
| Two CCS group | 29.96 | 2.74 | 6.812 | 0.000 |
| One CCS group | 36.20 | 2.67 |
- 1. Johnston PS, Sears BW, Lazarus MR, Frieman BG. Fixation of unstable type II clavicle fractures with distal clavicle plate and suture button. J Orthop Trauma 2014;28:e269-72.ArticlePubMed
- 2. Hohmann E, Hansen T, Tetsworth K. Treatment of Neer type II fractures of the lateral clavicle using distal radius locking plates combined with TightRope augmentation of the coraco-clavicular ligaments. Arch Orthop Trauma Surg 2012;132:1415-21.ArticlePubMedPDF
- 3. Kaipel M, Majewski M, Regazzoni P. Double-plate fixation in lateral clavicle fractures-a new strategy. J Trauma 2010;69:896-900.ArticlePubMed
- 4. Andersen JR, Willis MP, Nelson R, Mighell MA. Precontoured superior locked plating of distal clavicle fractures: a new strategy. Clin Orthop Relat Res 2011;469:3344-50.ArticlePubMedPMC
- 5. Lee W, Choi CH, Choi YR, Lim KH, Chun YM. Clavicle hook plate fixation for distal-third clavicle fracture (Neer type II): comparison of clinical and radiologic outcomes between Neer types IIA and IIB. J Shoulder Elbow Surg 2017;26:1210-5.ArticlePubMed
- 6. Sun S, Gan M, Sun H, Wu G, Yang H, Zhou F. Does subacromial osteolysis affect shoulder function after clavicle hook plating. Biomed Res Int 2016;2016:4085305.ArticlePubMedPMCPDF
- 7. Lin HY, Wong PK, Ho WP, Chuang TY, Liao YS, Wong CC. Clavicular hook plate may induce subacromial shoulder impingement and rotator cuff lesion: dynamic sonographic evaluation. J Orthop Surg Res 2014;9:6.ArticlePubMedPMCPDF
- 8. Flinkkilä T, Heikkilä A, Sirniö K, Pakarinen H. TightRope versus clavicular hook plate fixation for unstable distal clavicular fractures. Eur J Orthop Surg Traumatol 2015;25:465-9.ArticlePubMedPDF
- 9. Shin SJ, Ko YW, Lee J, Park MG. Use of plate fixation without coracoclavicular ligament augmentation for unstable distal clavicle fractures. J Shoulder Elbow Surg 2016;25:942-8.ArticlePubMed
- 10. Seyhan M, Kocaoglu B, Kiyak G, Gereli A, Turkmen M. Anatomic locking plate and coracoclavicular stabilization with suture endo-button technique is superior in the treatment of Neer Type II distal clavicle fractures. Eur J Orthop Surg Traumatol 2015;25:827-32.ArticlePubMedPDF
- 11. Struhl S, Wolfson TS. Closed-loop double endobutton technique for repair of unstable distal clavicle fractures. Orthop J Sports Med 2016;4:2325967116657810.ArticlePubMedPMCPDF
- 12. Mirbolook A, Sadat M, Golbakhsh M, Mousavi MS, Gholizadeh A, Saghari S. Distal clavicular fracture treatment with suture anchor method. Acta Orthop Traumatol Turc 2016;50:298-302.ArticlePubMed
- 13. Green DP, Rockwood CA, Bucholz RW, Heckman JD, Tornetta P. Rockwood and Green's fractures in adults. 8th ed. Lippincott Williams & Wilkins; 2015.
- 14. Tiefenboeck TM, Boesmueller S, Binder H, et al. Displaced Neer Type IIB distal-third clavicle fractures-Long-term clinical outcome after plate fixation and additional screw augmentation for coracoclavicular instability. BMC Musculoskelet Disord 2017;18:30.ArticlePubMedPMCPDF
- 15. Herrmann S, Schmidmaier G, Greiner S. Stabilisation of vertical unstable distal clavicular fractures (Neer 2b) using locking T-plates and suture anchors. Injury 2009;40:236-9.ArticlePubMed
- 16. Jung GH, Park CM, Kim JD. Biologic fixation through bridge plating for comminuted shaft fracture of the clavicle: technical aspects and prospective clinical experience with a minimum of 12-month follow-up. Clin Orthop Surg 2013;5:327-33.ArticlePubMedPMC
- 17. Bishop JY, Roesch M, Lewis B, Jones GL, Litsky AS. A biomechanical comparison of distal clavicle fracture reconstructive techniques. Am J Orthop (Belle Mead NJ) 2013;42:114-8.PubMed
- 18. Madsen W, Yaseen Z, LaFrance R, et al. Addition of a suture anchor for coracoclavicular fixation to a superior locking plate improves stability of type IIB distal clavicle fractures. Arthroscopy 2013;29:998-1004.ArticlePubMed
- 19. Rieser GR, Edwards K, Gould GC, Markert RJ, Goswami T, Rubino LJ. Distal-third clavicle fracture fixation: a biomechanical evaluation of fixation. J Shoulder Elbow Surg 2013;22:848-55.ArticlePubMed
- 20. Foerter JA, O'Brien SD, Bui-Mansfield LT. A systematic approach to the interpretation of the shoulder radiograph to avoid common diagnostic errors. Contemp Diagn Radiol 2017;40:1-7.Article
- 21. Bhatia DN, de Beer JF, du Toit DF. Coracoid process anatomy: implications in radiographic imaging and surgery. Clin Anat 2007;20:774-84.ArticlePubMed
References
Figure & Data
REFERENCES
Citations
Citations to this article as recorded by 
 ePub Link
ePub Link Cite
CiteComputational simulation of coracoclavicular screw insertion through the superior distal clavicular plate for clinical applications in Korean cadavers
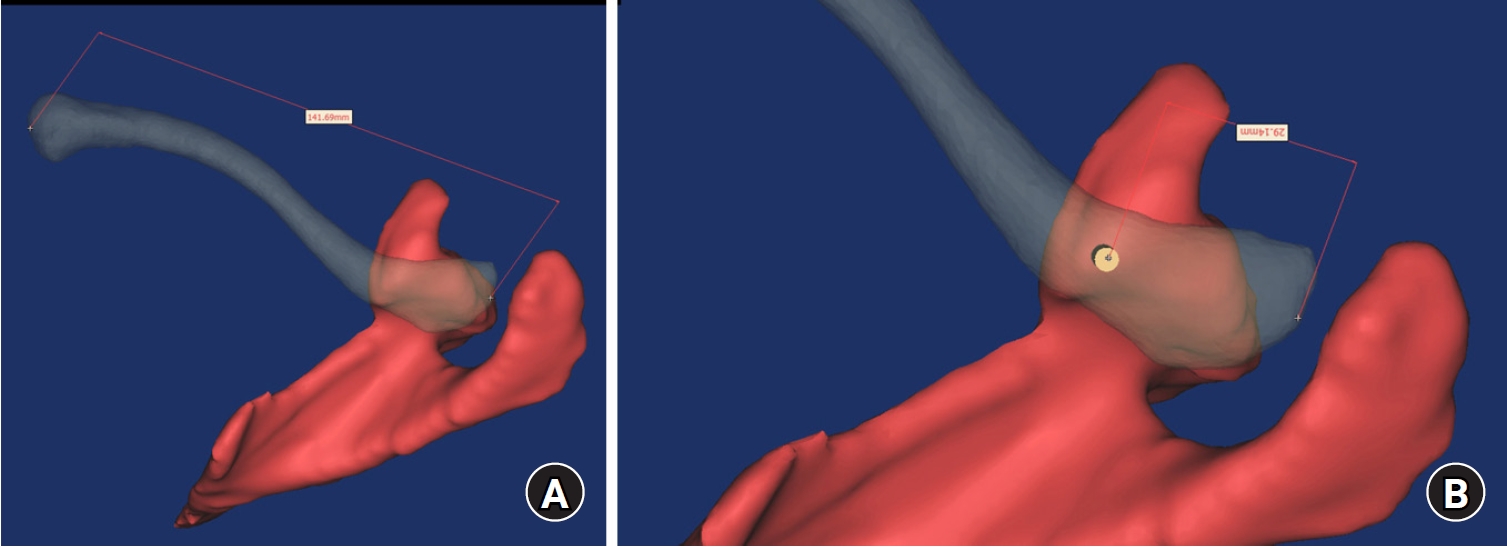
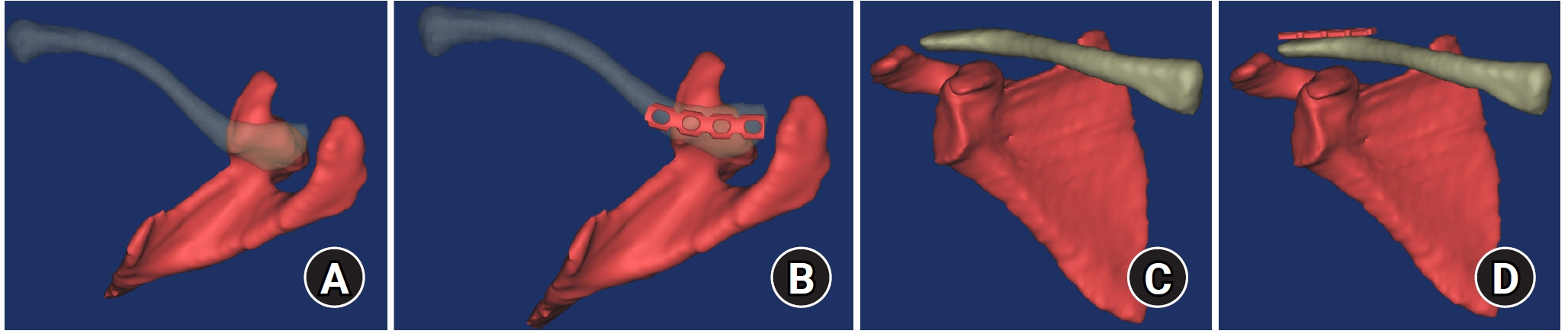
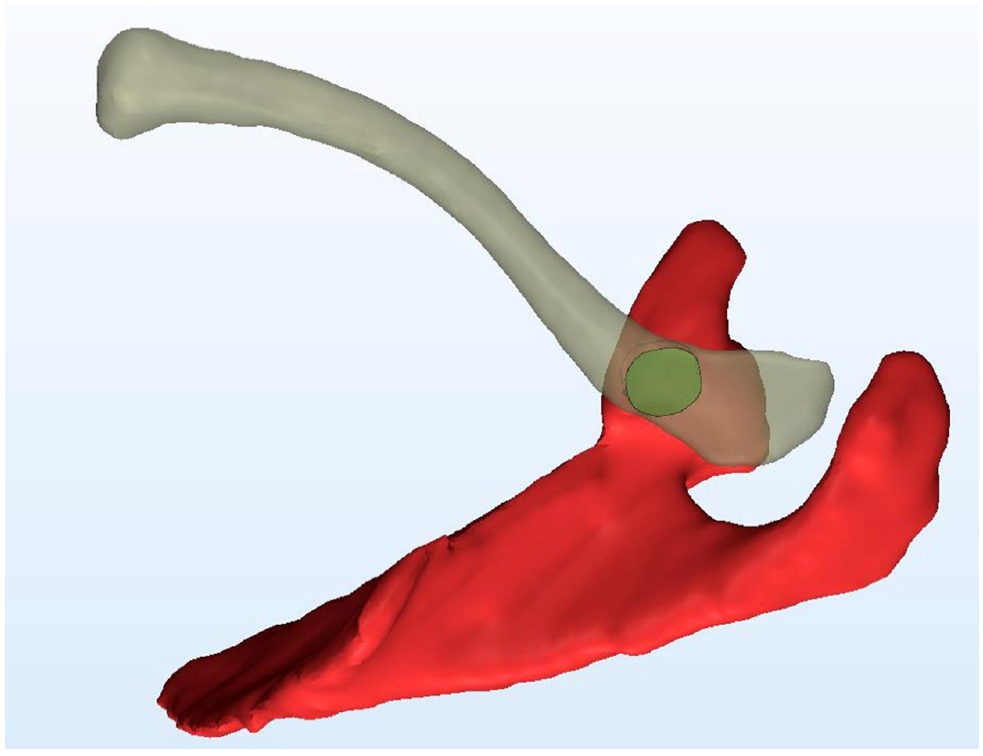
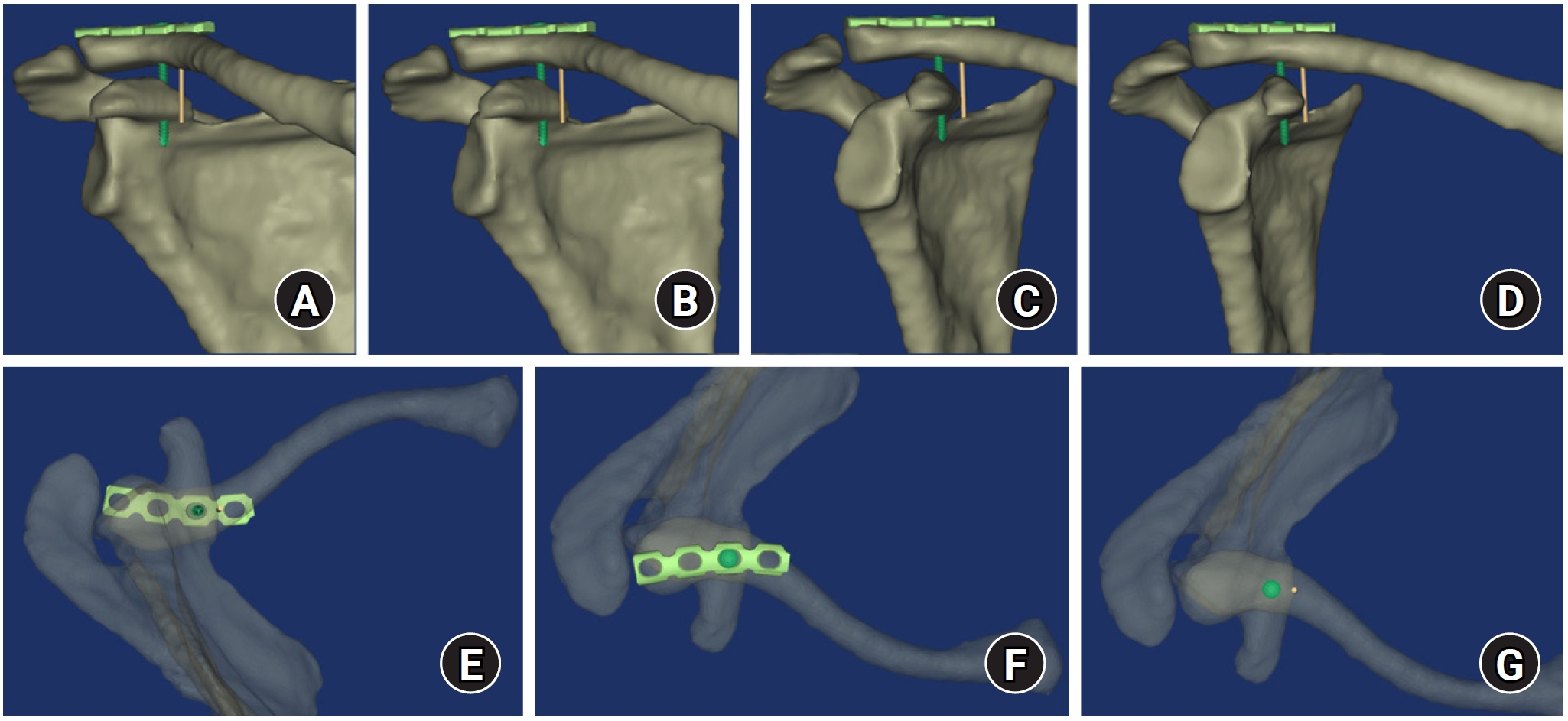
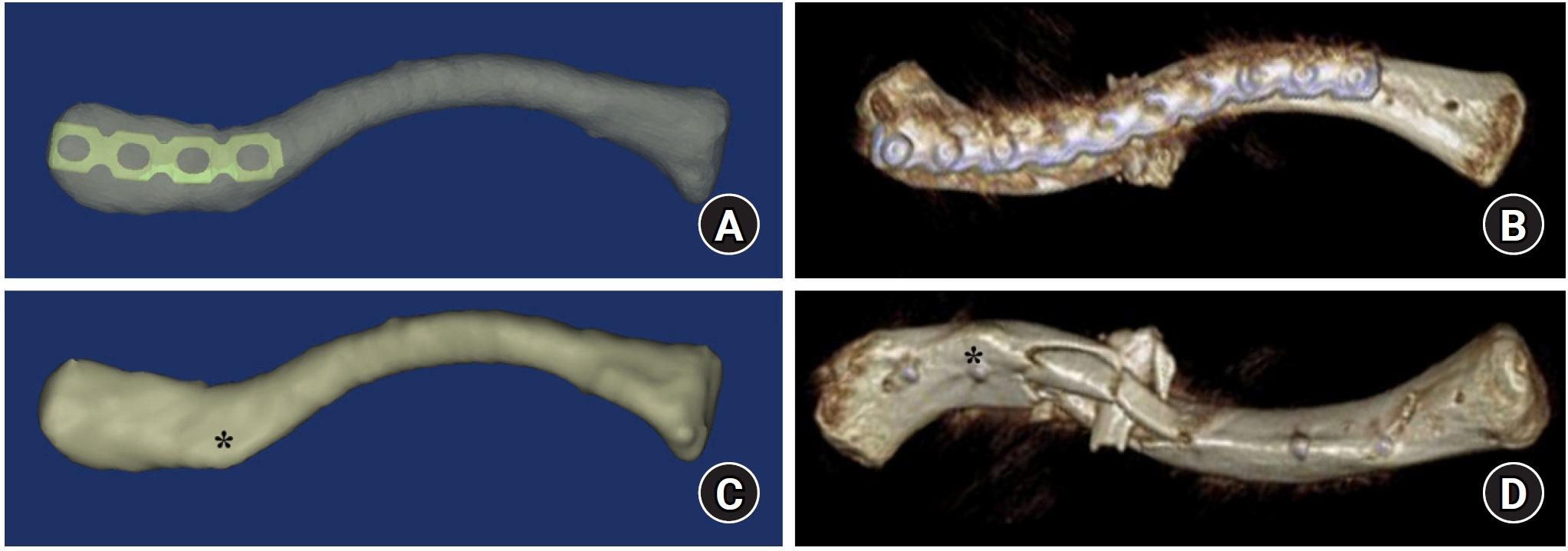
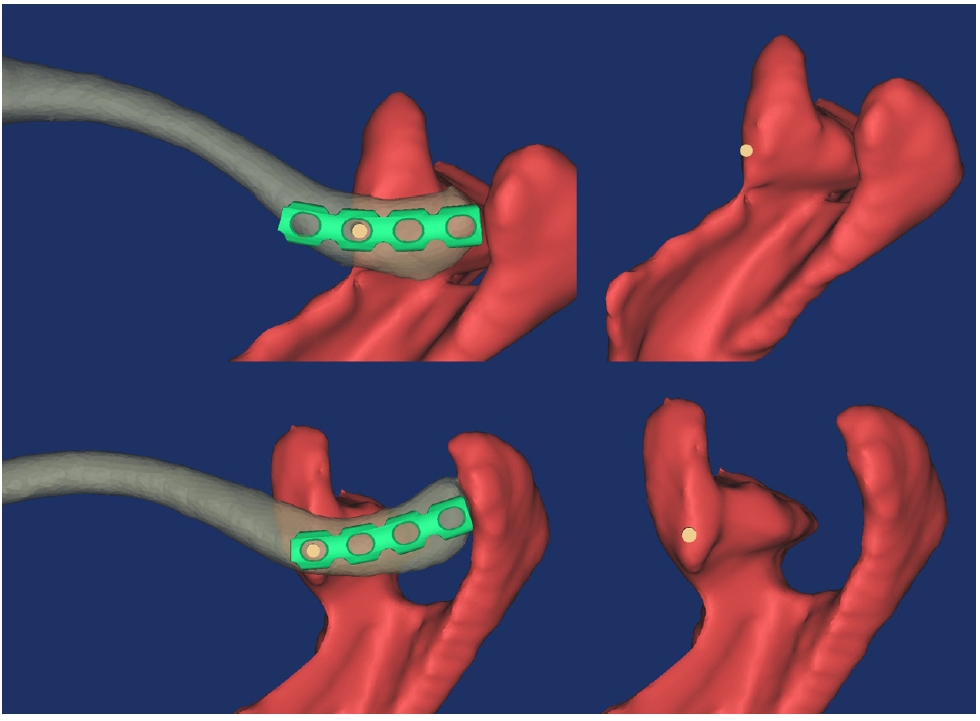
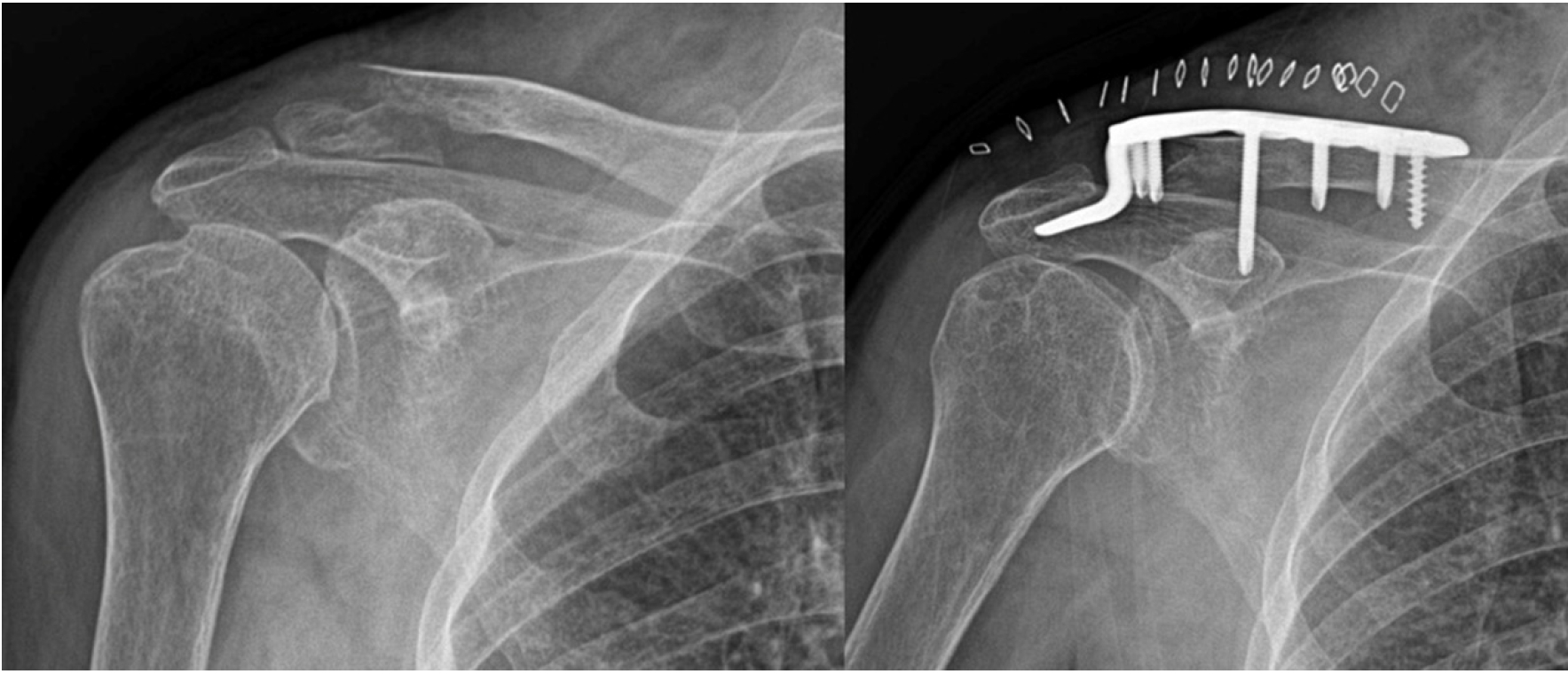
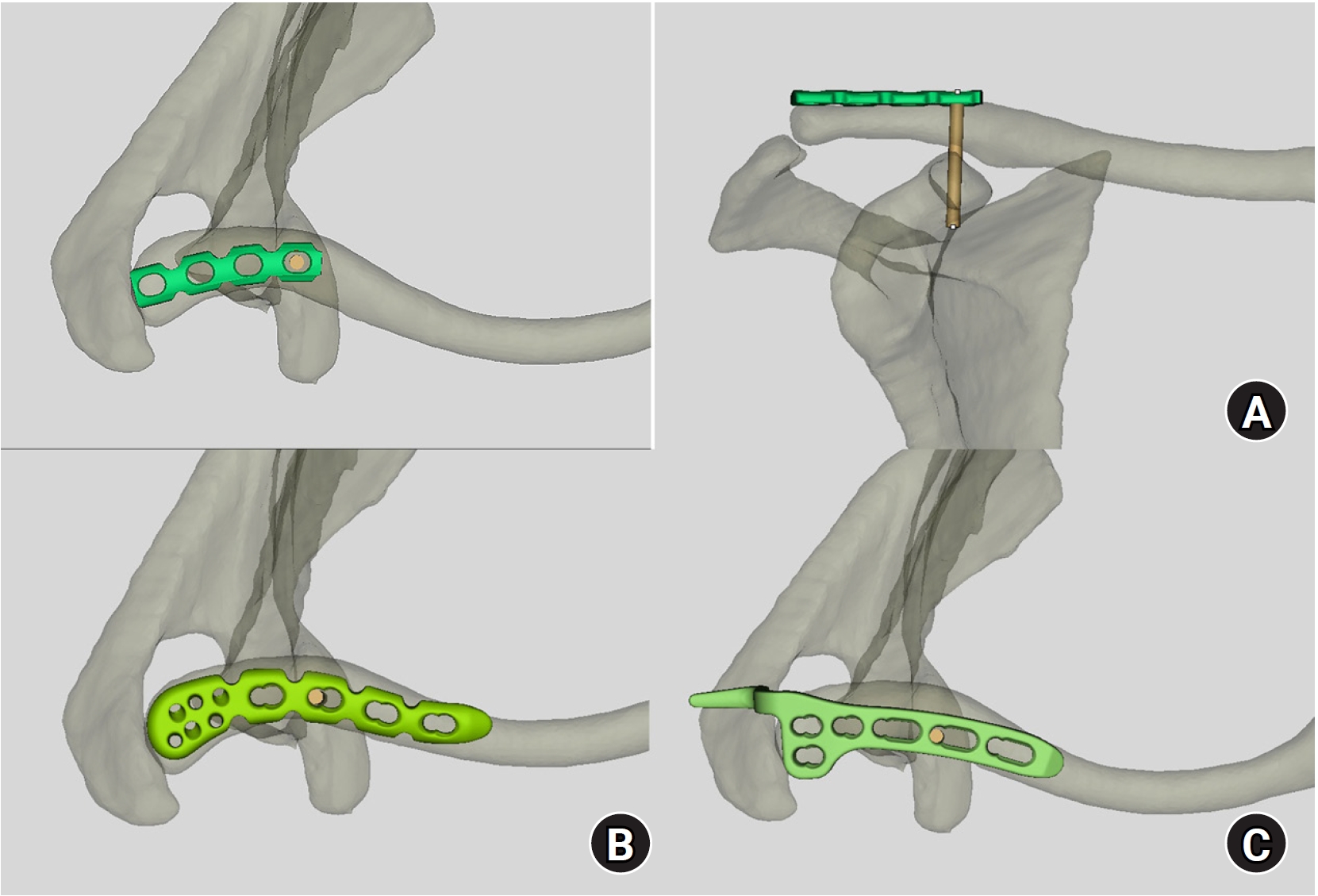
Fig. 1. Mimics software was used to reconstruct 3-dimentional models of the scapula and clavicle, and the transparency mode was controlled to identify the overlapping area between the clavicle and the coracoid process. The straight distance of the clavicle (A) and the distance between the lateral end of the clavicle and the elevated edge of the coracoid process (B) were measured using software.
Fig. 2. The optimally positioned pelvic recon curved plate was defined as the central area being on the upper surface of the clavicle in the cranial view (A, B) and well fitted in the anteroposterior view (C, D).
Fig. 3. On the cranial view of the clavicle, the upper surface of distal clavicle overlapped with the horizontal portion_coracoid process in a crossed direction. The overlapping area was located around the elevated edge and was sufficient to place the 3.5-mm and 4.5-mm screws.
Fig. 4. On an anteroposterior view of the shoulder, the intersection point between the imaginary vertical line from the medial border of coracoid process and distal clavicle was always placed medial to the third hole of the plate regardless of the degree of horizontal rotation of the scapula (A–D). In the cranial view, the imaginary vertical line corresponded to the medial border of the overlapping area (E–G).
Fig. 5. On a caudal view of the clavicle, the conoid tubercle (asterisk) of the lower surface of the clavicle was in accordance with the possibility of three-screw fixation in all models (A, B). In the comminuted clavicular fracture, which was fixed with a pelvic curved recon plate through the bridge plating technique, a postoperative biplanar 3-dimentional image shows that the lateral fragment lateral to the conoid tubercle (asterisk) could be fixed with three screws (C, D).
Fig. 6. Supplemental coracoclavicular screw fixation through the plate was inserted from the second hole in two models (A) and through the fourth hole in one model (B).
Fig. 7. An imaginary vertical line (asterisk) of preoperative radiograph could be utilized to classify the fracture and choose the implant based on the fixability of distal clavicular fragments (A, B).
Fig. 8. Considering the convex surface of horizontal portion_coracoid process and imaginary vertical line, the corresponding hole for the supplemental coracoclavicular screw through the plate could be fixed in the various kinds of precontoured distal clavicular plate: (A) pelvic curved recon plate, (B) precontoured distal clavicular plate, and (C) distal clavicular hook plate.
Fig. 1.
Fig. 2.
Fig. 3.
Fig. 4.
Fig. 5.
Fig. 6.
Fig. 7.
Fig. 8.
Computational simulation of coracoclavicular screw insertion through the superior distal clavicular plate for clinical applications in Korean cadavers
| Group | No. | Mean | SD | 95% CI | Minimum | Maximum |
|---|---|---|---|---|---|---|
| Second hole | 2 | 23.1 | 0.07 | 22.41–23.69 | 23.0 | 23.1 |
| Third hole | 77 | 30.0 | 2.17 | 29.49–30.48 | 25.0 | 35.1 |
| Fourth hole | 11 | 36.7 | 3.04 | 34.67–38.75 | 35.2 | 42.0 |
| Total | 90 | 30.7 | 3.36 | 29.95–31.36 | 23.0 | 42.0 |
| Group | Mean | Standard deviation | T | P-value |
|---|---|---|---|---|
| Two CCS group | 29.96 | 2.74 | 6.812 | 0.000 |
| One CCS group | 36.20 | 2.67 |
Table 1. Differences in distance_CP
All measurements were expressed as millimeters (mm). CP, horizontal portion; SD, standard deviation; CI, confidence interval.
Table 2. Comparison of two groups
CCS, coracoclavicular screw.

