 E-submission
E-submission TOTA
TOTA TOTS
TOTS
Previous issues
- Page Path
- HOME > Browse articles > Previous issues
- Volume 39(2); April 2026
-


Review Articles
- Definitive fixation for traumatic pelvic ring injuries: a dynamically informed, posterior-referenced framework
- Jeong-Hyun Koh, Seungyeob Sakong
- J Musculoskelet Trauma 2026;39(2):73-82. Published online March 24, 2026
- DOI: https://doi.org/10.12671/jmt.2026.00045
-
 Abstract
Abstract
 PDF
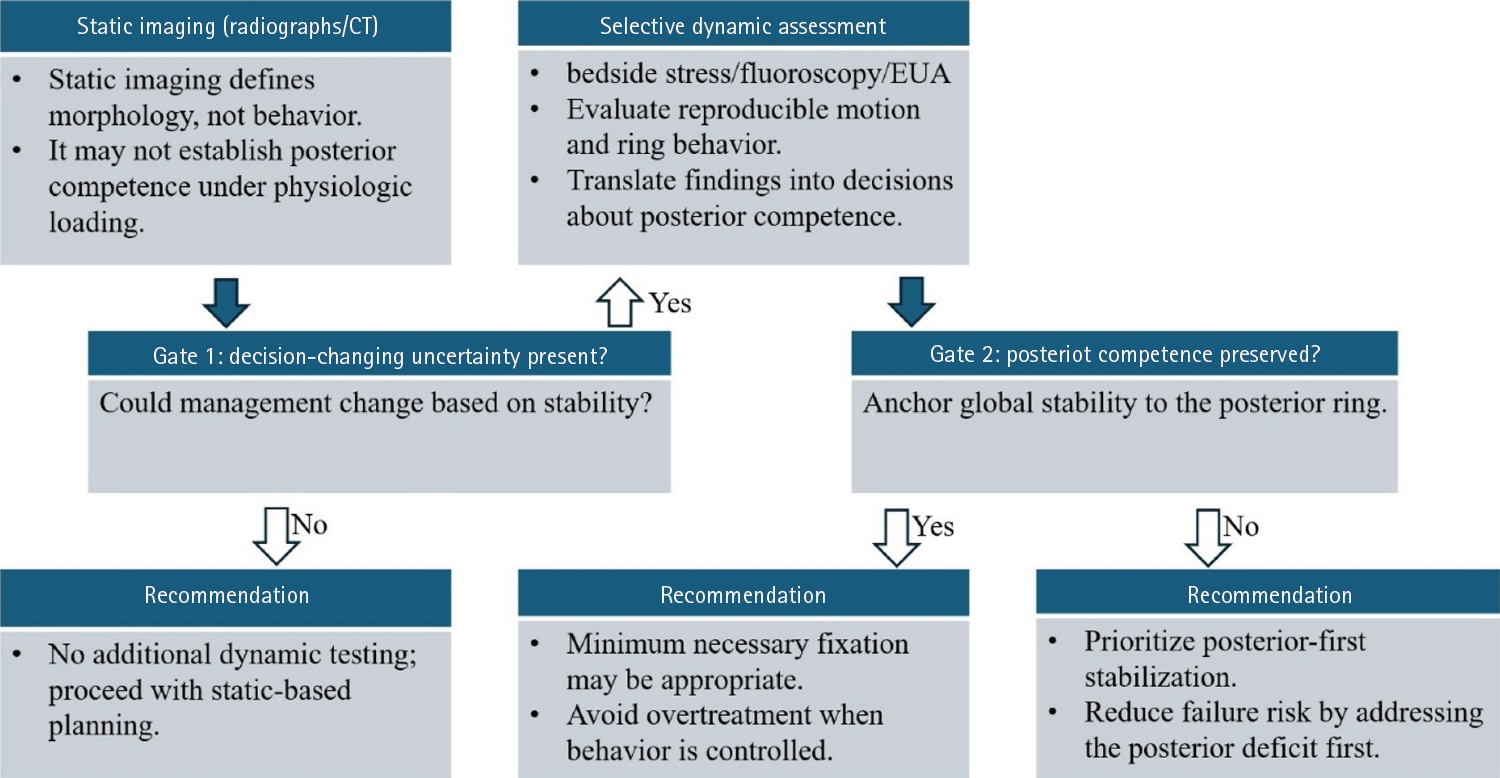
PDF - Optimal definitive fixation for traumatic pelvic ring injuries remains challenging because static radiographs and computed tomography, although essential for defining morphology, do not consistently predict load-dependent behavior during early mobilization. This uncertainty contributes to substantial practice variation and continued reliance on simplified displacement thresholds, such as the 2.5 cm rule. Such rules can misclassify instability by underrepresenting posterior competence and by privileging static measurements over functional behavior. In this narrative review, we propose a dynamically informed, posterior- referenced framework composed of three linked elements: (1) decision-linked terminology that explicitly distinguishes dynamic instability, radiographic change, and clinical failure; (2) selective stress-based assessment when uncertainty is likely to alter management; and (3) escalation along a fixation continuum that weighs incremental stability against operative burden. When static imaging cannot establish posterior competence with confidence, we outline selective stress-based approaches to assess pelvic ring behavior and to translate demonstrated instability into fixation selection along a defined continuum. Across all steps, the framework emphasizes minimum necessary fixation and explicitly incorporates the cost of selection as a primary decision variable. The operative question, therefore, shifts from gap width alone to clinically relevant motion and preservation of posterior competence. In doing so, this approach aims to reduce both undertreatment and overtreatment and to improve the consistency and defensibility of definitive fixation strategies across diverse practice environments.
- 1,651 View
- 37 Download

- Combined acetabular and pelvic ring injuries: a reference-frame algorithm for definitive fixation sequencing
- Jeong-Hyun Koh, Seungyeob Sakong
- J Musculoskelet Trauma 2026;39(2):83-92. Published online April 9, 2026
- DOI: https://doi.org/10.12671/jmt.2026.00031
-
Abstract
PDF
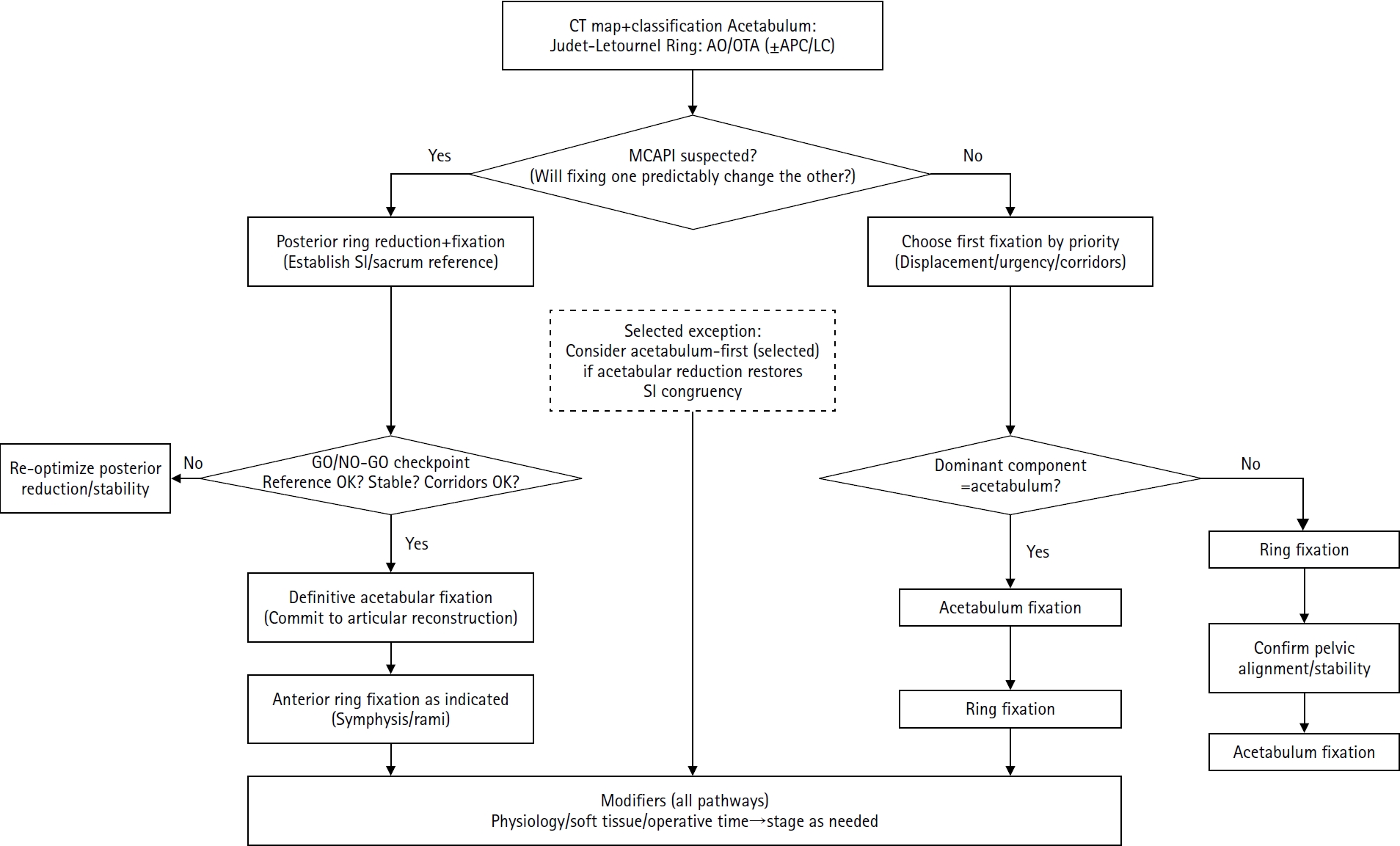
- Combined acetabular and pelvic ring injuries are not simply “two fractures in one patient.” Reduction and fixation of one component can alter the alignment and reducibility of the other, rendering operative sequencing a primary decision variable rather than a secondary consideration. These injuries typically result from high-energy trauma, frequently occur in patients with polytrauma, and are further influenced by physiological tolerance and the feasibility of available operative corridors. The existing evidence base remains constrained by retrospective study designs, inconsistent definitions, variable classification systems, and heterogeneous outcome reporting, all of which limit the strength of comparative recommendations. This state-of-the-art review presents a surgeon-facing, algorithmic approach grounded in a reference-frame mindset. We emphasize computed tomography (CT)-based mapping and the use of consistent terminology to characterize acetabular morphology, pelvic ring instability, deformity vectors, suspicion of mechanical coupling, and feasible operative corridors. Mechanically connected acetabular and pelvic ring injuries (MCAPI) are introduced as a working framework for identifying patterns in which reduction or fixation of one injury predictably influences the other. In cases of suspected MCAPI, a posterior ring-based sequence is generally preferred, typically consisting of posterior ring reduction and fixation, definitive acetabular reconstruction, and subsequent anterior ring fixation. We propose an explicit intraoperative “GO/NO-GO” checkpoint (reference acceptable, stable, corridors feasible) to prevent acetabular reconstruction on a moving target. Acetabulum-first strategies may be appropriate only in selected anteroposterior compression- type configurations in which acetabular fixation plausibly restores sacroiliac congruency and posterior stabilization remains technically feasible. We summarize key outcome domains and complication patterns, highlighting hip dislocation as an important risk factor associated with both neurologic deficits and overall complications. Standardized CTbased definitions and outcome instruments, together with multicenter cohorts employing predefined decision pathways, are required to test sequencing strategies and to determine whether improved radiographic reduction translates into durable functional benefit.
- 2,603 View
- 37 Download
- Nonoperative management of distal radius fractures: when and how?
- Shin Woo Choi, Jae Kwang Kim
- J Musculoskelet Trauma 2026;39(2):93-102. Published online March 10, 2026
- DOI: https://doi.org/10.12671/jmt.2026.00024
-
Abstract
PDF
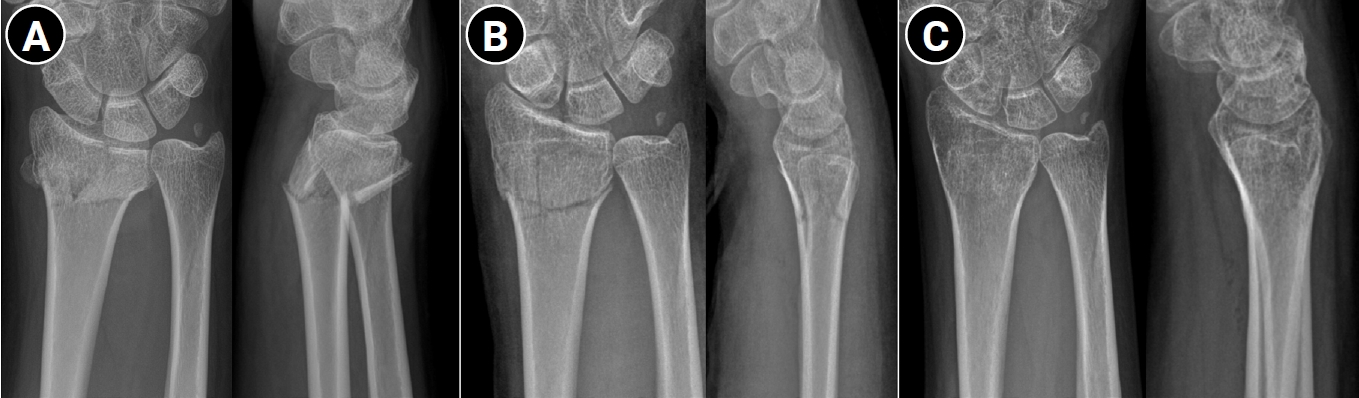
- Distal radius fractures are among the most common injuries of the upper extremity, particularly in the elderly population. Although the use of volar locking plate fixation has increased in recent years, evidence from randomized and prospective studies demonstrates that, while operative treatment may achieve superior radiographic alignment and enable more rapid early recovery, these advantages tend to diminish over time and do not result in superior long-term patient-reported functional outcomes in elderly patients. In addition, radiographic parameters show only a limited correlation with functional recovery. Consequently, nonoperative treatment remains a valid and important treatment option for distal radius fractures. The decision to pursue nonoperative management should be based on a comprehensive assessment of radiographic parameters—including dorsal tilt, radial shortening, and intraarticular displacement—together with patient-specific factors such as age, activity level, comorbidities, and functional expectations. For stable or minimally displaced fractures, an immobilization period of 3‒4 weeks is generally recommended, whereas displaced fractures typically require immobilization for 5‒6 weeks. In cases requiring manual reduction, traditional treatment protocols recommend weekly radiographic follow-up during the first 2‒3 weeks to monitor for secondary displacement. Successful nonoperative management should also emphasize effective swelling control through limb elevation, as well as the initiation of early finger exercises to prevent hand stiffness. After removal of the cast or splint, active wrist mobilization is essential for restoring optimal range of motion and achieving functional recovery.
- 10,478 View
- 65 Download
Original Articles
- Sex-specific bottlenecks and risk zones in the retrograde superior pubic ramus screw corridor: a 3D CT-based morphometric cadaver study
- Ji Won Jeong, Jung Tae Ahn, Gu Hee Jung, Kun Tae Kim
- J Musculoskelet Trauma 2026;39(2):103-116. Published online March 26, 2026
- DOI: https://doi.org/10.12671/jmt.2026.00066
-
Abstract
PDF
 Supplementary Material
Supplementary Material - Background
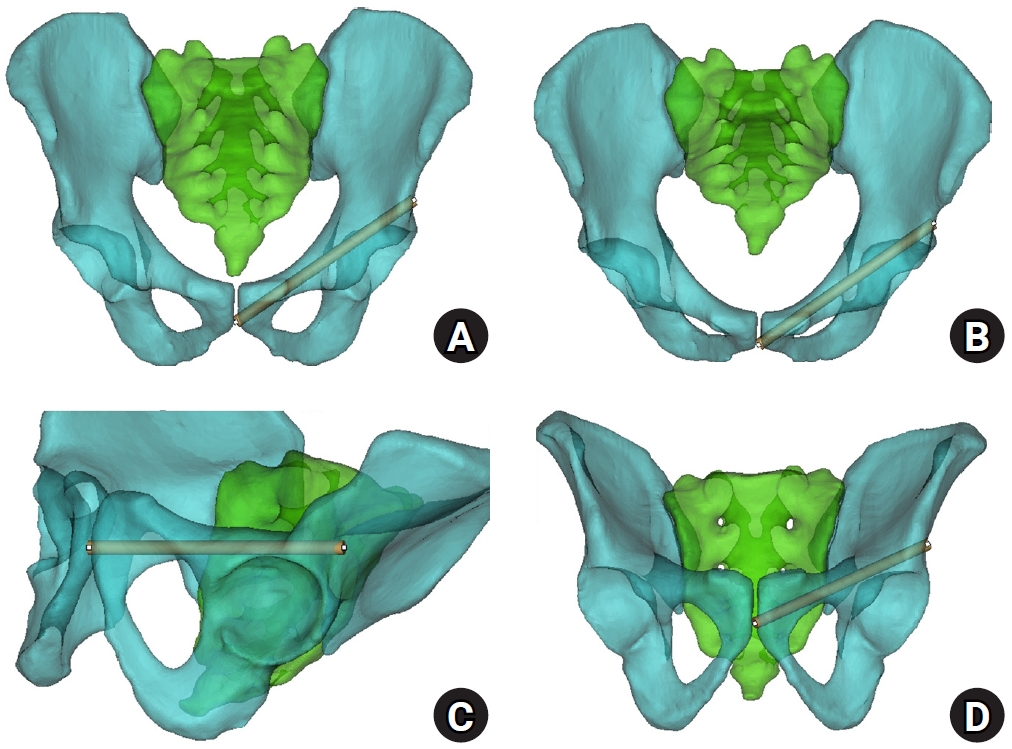
Superior ramus screw fixation is commonly used to stabilize anterior pelvic ring injuries but is constrained by a narrow, irregular, and curved intraosseous corridor. Trajectory-based morphometric analysis may assist in screw diameter selection and enable identification of reproducible anatomic constriction zones.
Methods
We conducted a cross-sectional computed tomography (CT)-based morphometric study of 82 cadaveric pelvises (42 males, 40 females). Bottleneck diameter was defined as the diameter of the largest fully contained virtual cylinder along the planned trajectory, and cylinder length was recorded. Orthogonal cross-sections at 9.5-mm intervals (up to 12 segments) were generated to measure segment-wise effective diameter (defined as twice the minimum centerline-to-cortex distance) and cortical clearance, which was used as a diameter-based safety margin. Segments were realigned to the acetabular start segment to define relative segment positions (Δ seg). Feasibility was assessed for prespecified screw diameters ranging from 3.5 to 7.3 mm.
Results
Mean bottleneck diameter was larger in males than in females (7.34±1.10 vs. 5.93±0.98 mm), whereas trajectory length was similar between sexes (127.85±8.54 vs. 128.85±8.20 mm). Δ seg realignment localized corridor constriction to two discrete zones: a preacetabular zone (Δ seg −6 to −4) and a periacetabular zone (Δ seg 1 to 2), where effective diameter and cortical clearance were most limited. Feasibility rates were 100% at 3.5–4.5 mm, 95.2% vs. 82.5% at 5.0 mm, 81.0% vs. 27.5% at 6.5 mm, and 59.5% vs. 10.0% at 7.3 mm in males and females, respectively.
Conclusions
Female models demonstrated smaller trajectory-wide bottleneck diameters and segment-wise effective diameters than male models. Acetabular-referenced Δ seg realignment identified two reproducible anatomic risk zones: a preacetabular zone adjacent to the obturator neurovascular bundle and a periacetabular zone near the external iliac vessels. At diameters ≥6.5 mm, cortical proximity increased more prominently in females than in males. Level of evidence: III.
- 1,078 View
- 29 Download
- Percutaneous anterior leverage technique for anteromedial cortical support in intertrochanteric femur fractures: a computed tomography-based validation study
- Whee Sung Son, Bum Jin Shim, Oog-jin Shon
- J Musculoskelet Trauma 2026;39(2):117-129. Published online March 27, 2026
- DOI: https://doi.org/10.12671/jmt.2025.00311
-
Abstract
PDF
- Background
Anteromedial cortical support (AMCS) enhances stability in intertrochanteric femur fractures. However, reproducible, validated methods of achieving AMCS have not previously been reported. This study introduces a percutaneous anterior leverage technique and validates its AMCS effects using computed tomography (CT).
Methods
We retrospectively reviewed patients treated by a single surgeon between March 2022 and December 2024. The inclusion criteria were an AO/OTA classification of A1–A3, application of the percutaneous anterior leverage technique, available pre- and postoperative CT, and ≥6 months follow-up. Outcomes included CT-based AMCS (anterior on axial and medial on coronal images, classified as positive, neutral, or negative), time to union, union rate, changes in neck-shaft angle, and treatment failure (varus collapse, blade cut-through, or nonunion without the former two). The risk factors for failure were analyzed.
Results
Of 273 patients reviewed, 53 met the inclusion criteria. Follow-up was at least 6 months in all cases. Positive anterior support was achieved in 37 patients (69.8%) and positive medial support in 42 (79.25%). No patient demonstrated negative anterior support; one (1.9%) had negative medial support. Cortical support improved significantly after surgery. CT images demonstrated significant postoperative improvements (anterior P=0.026; medial P<0.001). Bone union was achieved in 50 patients (94.34%) at a mean of 3.93±1.48 months. The mean change in the neck-shaft angle at last follow-up was 1.75°±2.34° varus. Three patients (5.66%) experienced treatment failure. Anteromedial cortical breakage during follow-up differed between failure and nonfailure groups (P=0.002), but regression identified no independent predictors. No technique-related complications were observed.
Conclusions
Our percutaneous anterior leverage technique produced favorable CT-confirmed AMCS and high union with low failure, supporting its safety and effectiveness in intertrochanteric femur fractures. Level of evidence: IV.
- 1,214 View
- 42 Download
- Biomechanical comparison of anatomically precontoured patellar plate, anterior tension wiring through cannulated screws, and double-sided plating in patellar fractures using a synthetic bone model
- Abdullah M. Aljeaid, Wonseok Choi, Jeong-Seok Choi, Youngsig Choi, Jiyeon Bae, Jong-Keon Oh, Jae-Woo Cho
- J Musculoskelet Trauma 2026;39(2):130-139. Published online April 7, 2026
- DOI: https://doi.org/10.12671/jmt.2025.00353
-
Abstract
PDF
- Background
Patellar fractures are common injuries that require stable fixation to achieve optimal healing and restoration of knee function. This study aimed to analyze the mechanical properties of an anatomically precontoured patellar plate and to compare its maximum tensile load-bearing capacity with that of anterior tension wiring through cannulated screws and double-sided plating for the fixation of patellar fractures.
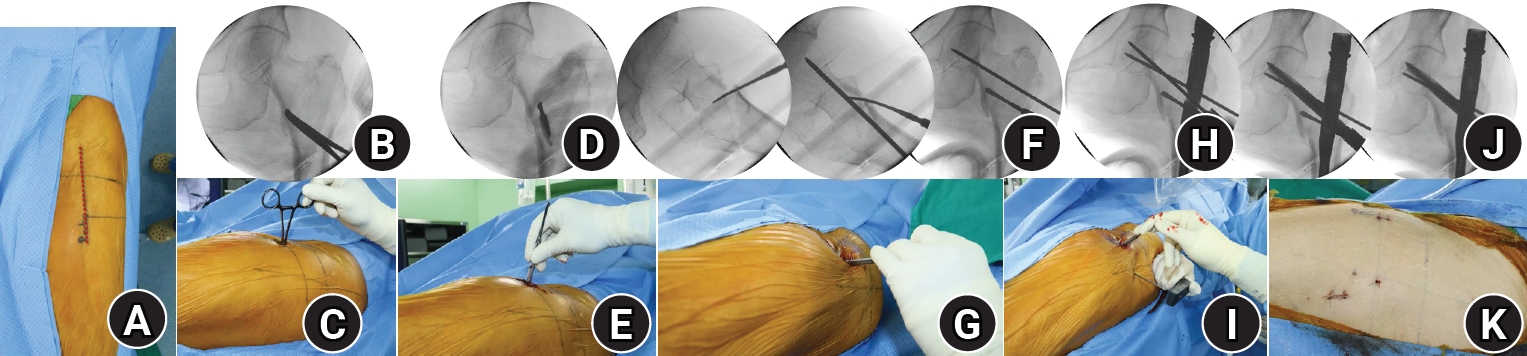
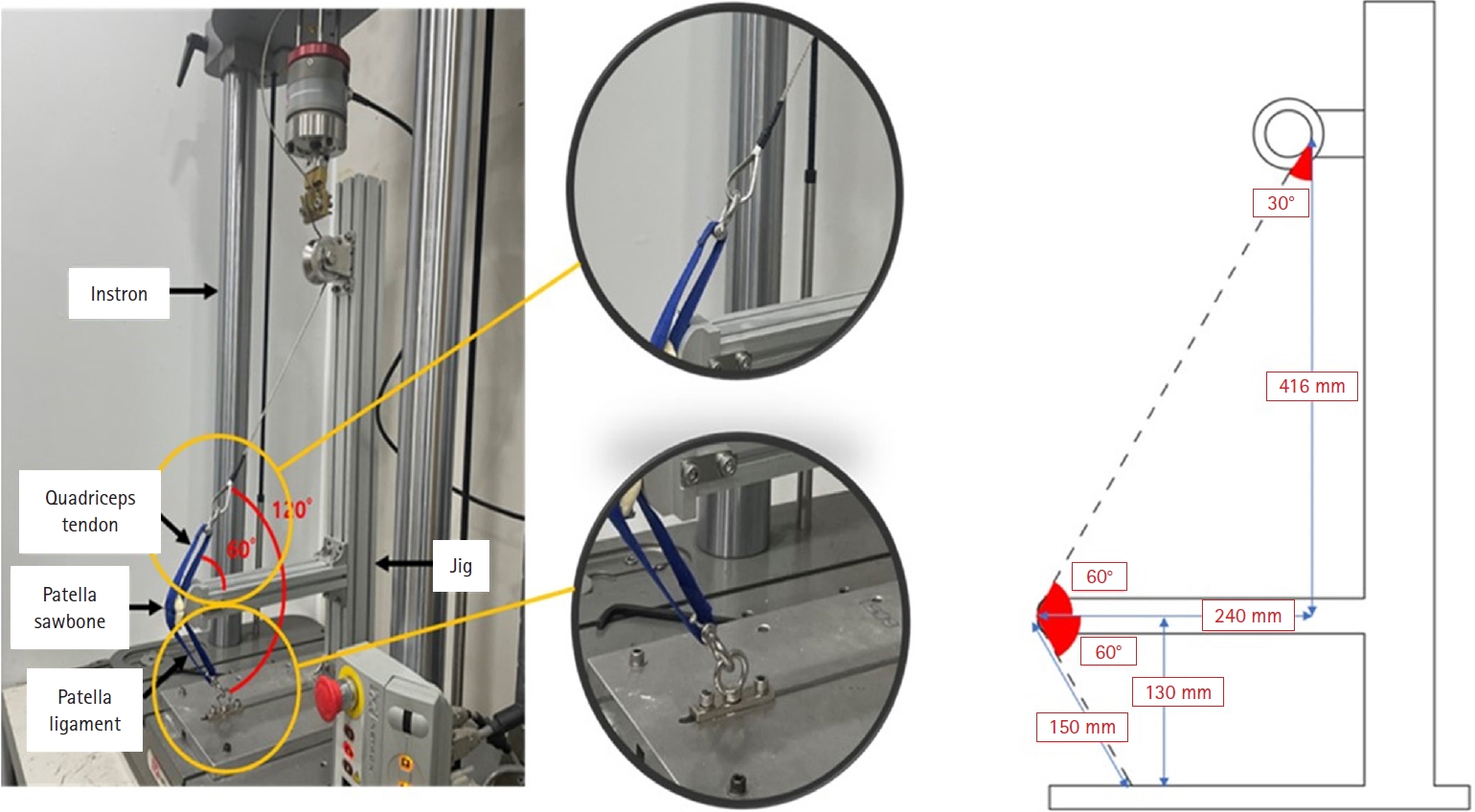
Methods
Artificial Sawbones with a standardized transverse fracture line were used to simulate patellar fractures. Each sawbone was attached to polyester bands, and this fracture model was applied consistently across all test samples. To evaluate mechanical properties of the anatomically precontoured patellar plate (model code 25-ANPA-209) made of ASTM F67 titanium, static tensile strength testing and dynamic tensile strength testing were performed, with seven samples prepared for each test. For comparison of maximum tensile load capacity among the anatomically precontoured patellar plate, anterior tension wiring through cannulated screws, and double-sided plating, five samples were prepared for each fixation group. All specimens were tested using a tension/compression testing machine.
Results
In the static tensile strength test, all seven samples exhibited a maximum tensile load capacity above 844 N without any fractures or failure points. The dynamic tensile strength test showed that all seven samples completed 10,000 cycles without deformation or damage to the anatomically precontoured patellar plate. When comparing maximum tensile load capacity, the anatomically precontoured patellar plate exhibited a significantly higher maximum tensile load-bearing capacity than anterior tension wiring through cannulated screws and double-sided plating.
Conclusions
The anatomically precontoured patellar plate demonstrated satisfactory mechanical performance, successfully meeting the criteria of both static and dynamic tensile strength testing, and showed superior maximum tensile load-bearing capacity compared with the other fixation methods evaluated. These findings suggest that the anatomically precontoured patellar plate may represent a reliable fixation option for the management of patellar fractures. Level of evidence: V.
- 1,008 View
- 25 Download
- Biomechanical analysis of medial distal tibial locking plate fixation for distal-third spiral tibial shaft fractures
- Yao-Jen Liu
- J Musculoskelet Trauma 2026;39(2):140-146. Published online April 10, 2026
- DOI: https://doi.org/10.12671/jmt.2026.00094

-
Abstract
PDF
- Background
Distal spiral fractures of the tibial shaft present fixation challenges, particularly in patients who are not suitable candidates for intramedullary nailing. This study evaluated the biomechanical stability of medial minimally invasive percutaneous plating osteosynthesis (MIPO) under various physiological loading conditions.
Methods
A finite-element model of a distal AO/OTA 42-A1.1c spiral fracture of the tibia was created using computed tomography data. A precontoured titanium medial distal tibia locking compression plate with nine locking screws was simulated. Material properties were assigned to cortical and cancellous bone. The loading conditions included axial compression (750 N), varus/valgus bending (300 N at a 9° offset), and internal/external torsion (7.5 N·m). von Mises stress and fracture displacement were analyzed.
Results
Axial loading produced a peak plate stress of 508.06 MPa and a displacement of 2.17 mm. Valgus and varus loading generated stresses of 490.17 MPa and 324.08 MPa, respectively, with corresponding displacements of 3.86 mm and 2.01 mm. External and internal torsion resulted in stresses of 354.23 MPa and 358.9 MPa, respectively, with corresponding displacements of 2.64 mm and 2.22 mm.
Conclusions
Medial distal tibial plating demonstrated favorable biomechanical performance in this finite-element model; however, clinical extrapolation should be made cautiously. Level of evidence: V.
- 475 View
- 18 Download
- Clinical and radiographic outcomes of hemiarthroplasty for proximal humeral fractures in Korea with three or more years of follow-up: a retrospective cohort study
- Sang Jin Cheon, Kyu-Hak Jung, Min Hyeok Choi, Suk-Woong Kang
- J Musculoskelet Trauma 2026;39(2):147-155. Published online February 26, 2026
- DOI: https://doi.org/10.12671/jmt.2025.00325

-
Abstract
PDF
- Background
Shoulder hemiarthroplasty (HA) is an established treatment option for complex proximal humeral fractures, particularly in cases involving severe comminution or osteoporotic bone. This study investigated the clinical and radiographic outcomes of HA with a minimum follow-up of 3 years and aimed to identify prognostic factors associated with postoperative function.
Methods
We retrospectively reviewed 44 patients (16 males and 28 females; mean age, 61.2 years; range, 23–83 years) who underwent shoulder HA for complex proximal humeral fractures between 2005 and 2018. The mean follow-up duration was 70.4 months (range, 36–168 months). Clinical evaluations included the Constant score, visual analog scale pain score, patient satisfaction, and range of motion. Radiographic assessments examined tuberosity healing, radiolucent lines, acromiohumeral distance (AHD), and glenoid arthrosis.
Results
At the 3-year follow-up, 64% of patients reported being satisfied or very satisfied. The mean Constant score was 46.6 (range, 13–71), and the age- and sex-adjusted Constant score was 53.5 (range, 19–92). Radiographically, 23% of patients demonstrated radiolucent lines, and 41% showed evidence of glenoid arthrosis. Tuberosity absorption occurred in 39% of patients, with a mean onset of 11.2 months postoperatively, and was significantly associated with lower Constant scores and reduced range of motion. Patients younger than 60 years demonstrated better functional outcomes and lower rates of tuberosity absorption. The mean AHD decreased from 8.4 mm postoperatively to 4.4 mm at the 3-year follow-up (P<0.001).
Conclusions
Shoulder HA for complex proximal humeral fractures yielded satisfactory pain relief and functional outcomes, particularly when tuberosity healing was preserved. However, elderly patients with diminished bone quality were more likely to develop tuberosity absorption and experience poorer functional recovery. Meticulous surgical technique and careful postoperative surveillance remain essential to achieving optimal results. Level of evidence: III.
- 899 View
- 24 Download
- Clinical and radiographic outcomes of elastic stable intramedullary nailing for pediatric humeral shaft fractures: a retrospective case series
- Kang-San Lee, Dongju Shin, Sang Hee Kim, Il Seo, Tae-Hoon Kim, Sung Jung Kim
- J Musculoskelet Trauma 2026;39(2):156-161. Published online March 10, 2026
- DOI: https://doi.org/10.12671/jmt.2025.00381
-
Abstract
PDF
- Background
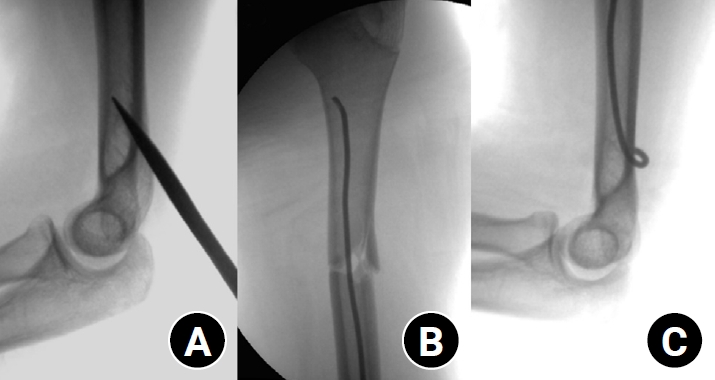
Pediatric humeral shaft fractures are uncommon and are generally treated conservatively, with satisfactory clinical outcomes reported in most cases. However, conservative management often necessitates prolonged immobilization and frequent outpatient follow-up visits, and it carries an inherent risk of residual angular or translational deformity. Elastic stable intramedullary nailing (ESIN) provides a simple and minimally invasive method of fracture fixation that offers adequate stability without disrupting the periosteal blood supply, thereby permitting early mobilization and promoting rapid bone union. The purpose of this study was to evaluate the clinical and radiological outcomes of ESIN fixation in pediatric patients with humeral shaft fractures.
Methods
The medical records of pediatric patients with humeral shaft fractures who underwent ESIN fixation between January 2015 and November 2025 were retrospectively reviewed. Data collected included patient demographics, mechanism of injury, fracture location, number of elastic nails used, time to union, degree of residual angulation, range of motion (ROM), and postoperative complications.
Results
The mean age of the patients was 10.0 years (range, 7 to 15 years). The mean time to radiographic union was 5.4 weeks (range, 2.4 to 10.4 weeks). The mean coronal angulation was 0.2° (range, −9.1° to 5.8°), while the mean sagittal angulation was −1.3° (range, −6.9° to 5.3°). No cases of infection, nerve injury, or nail migration were observed during the follow-up period. At the final follow-up assessment, all patients demonstrated full shoulder and elbow ROM, with no residual deformity or pain reported.
Conclusions
In this small retrospective case series, ESIN fixation resulted in favorable union rates and excellent functional outcomes in pediatric humeral shaft fractures. Level of evidence: IV.
- 638 View
- 22 Download
-
NSAID-induced suppression of type X collagen and VEGF expression in the early phase of rat femoral fracture healing

- Maria Zafar, Rana Mohammad Zeeshan, Safia Tasawar, Muhammad Saad Ilyas, Amer Aziz, Uruj Zehra
- J Musculoskelet Trauma 2026;39(2):162-173. Published online April 10, 2026
- DOI: https://doi.org/10.12671/jmt.2025.00367
-
Abstract
PDFSupplementary Material
- Background
The current literature presents conflicting evidence regarding the effects of nonsteroidal anti-inflammatory drugs (NSAIDs) on fracture healing. This experimental study aimed to evaluate and compare the histological and immunohistochemical changes during femoral fracture healing in rats treated with a nonselective cyclooxygenase (COX) inhibitor (diclofenac sodium) and a selective COX-2 inhibitor (celecoxib).
Methods
Thirty-six male Wistar (standard outbred) albino rats weighing 200–400 g underwent standardized mid-diaphyseal femoral fracture surgery. The animals were randomized into three groups (n=12 per group): group 1 received diclofenac sodium, group 2 received celecoxib, and group 3 served as the control group and received 1 mL of distilled water orally once daily. Six rats from each group were euthanized at the end of the 2nd and 7th weeks after fracture for sample collection. Histological examination was complemented by immunohistochemical analysis, and the expression of type X collagen and vascular endothelial growth factor (VEGF) was assessed using the immunoreactive score (IRS) method.
Results
Healing scores were significantly higher in the control group at both time points (2nd week, P=0.01; 7th week, P=0.03). At the 2nd week, rats treated with diclofenac sodium demonstrated significantly greater fibrosis (P=0.01), and by the 7th week, they exhibited impaired bone formation (P=0.003) along with increased bone defects (P=0.01). IRS values for type X collagen and VEGF were significantly higher in the control group than in both treatment groups during the 2nd week (P=0.01 and P=0.005, respectively).
Conclusions
These findings suggest that, in this rat model, NSAIDs, particularly nonselective COX inhibitors, may disrupt the early phases of bone repair by affecting hypertrophic chondrocyte differentiation and reducing angiogenic activity. Although these results indicate a potential risk to optimal healing, they are preclinical observations, and their relevance to clinical fracture management should be interpreted with caution. Level of evidence: V.
- 893 View
- 20 Download
Case Report
- Paradoxical hypertrophy as a cause of femoral insufficiency fractures analyzed through differences in force application in Korea: three case reports
- Yong-Uk Kwon, Dae-Hyun Park, Hyoung-Gu Kang
- J Musculoskelet Trauma 2026;39(2):174-180. Published online April 23, 2026
- DOI: https://doi.org/10.12671/jmt.2025.00388
-
Abstract
PDF
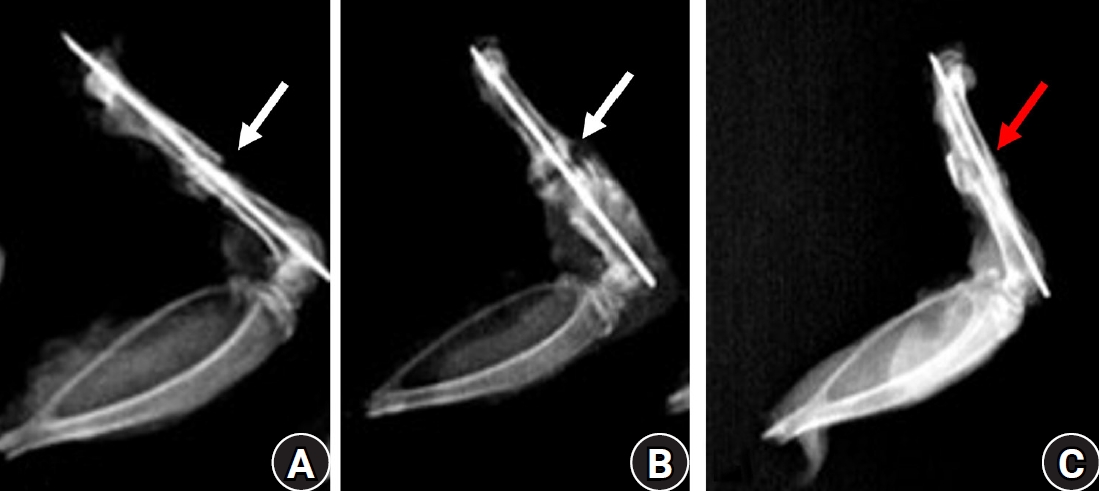
- Previous studies have extensively examined the association between femoral insufficiency fractures and prolonged bisphosphonate therapy. However, alternative etiologies remain insufficiently characterized. This study aimed to analyze nonpharmacologic factors associated with femoral insufficiency fractures, with particular emphasis on paradoxical cortical hypertrophy and altered biomechanical load distribution. We reviewed three cases of femoral insufficiency fracture that were surgically treated at our institution between January 2018 and January 2022. None of the patients had a history of bisphosphonate use. Clinical histories—including underlying comorbidities, prior surgical procedures, and radiographic findings—were evaluated. Serial radiographs obtained before and after fracture occurrence were analyzed to characterize fracture morphology and associated cortical changes. Case 1 involved a patient with posttraumatic hip synostosis; case 2 involved a patient with osteogenesis imperfecta; and case 3 involved a patient who had previously undergone intramedullary nailing for an intertrochanteric fracture. Lateral femoral bowing and cortical hypertrophy preceded fracture development in two cases, whereas focal cortical hypertrophy at the distal locking screw site was observed in the third case. No history of bisphosphonate therapy was identified in any patient. Fractures developed at sites characterized by increased cortical remodeling and abnormal load concentration. Femoral insufficiency fractures can occur in the absence of bisphosphonate therapy. Paradoxical cortical hypertrophy and altered biomechanical force distribution appear to be important contributing factors. Level of evidence: IV.
- 355 View
- 16 Download
Letter to the Editor
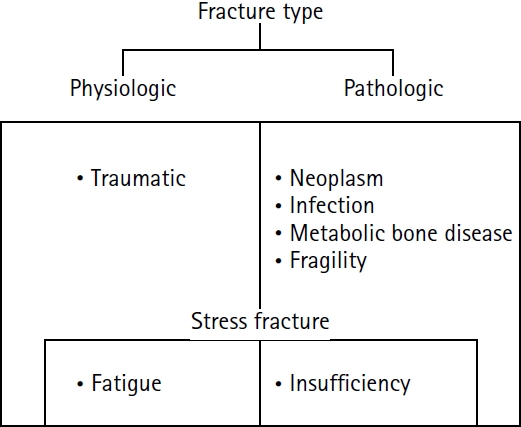
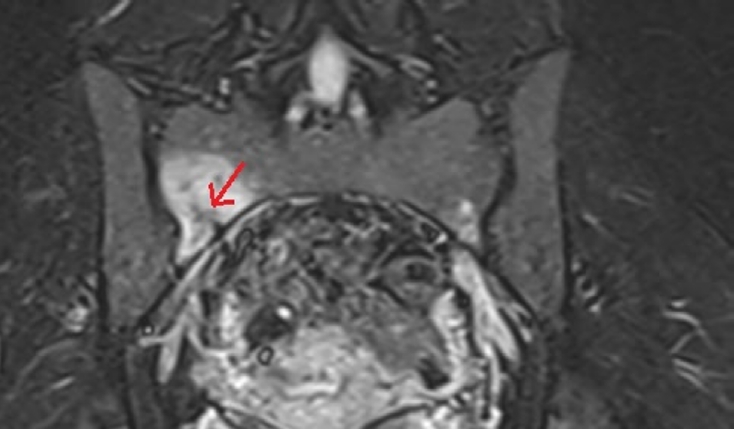
- Sacral stress fracture mimicking sacroiliac pathology in two young adults: a reminder to systematically review the sacrum on hip/sacroiliac magnetic resonance imaging
- Nihal Karayer Özgül, Sami Özgül
- J Musculoskelet Trauma 2026;39(2):181-183. Published online February 25, 2026
- DOI: https://doi.org/10.12671/jmt.2026.00038
- 503 View
- 12 Download
 First
First Prev
Prev

