 E-submission
E-submission TOTA
TOTA TOTS
TOTS
Articles
- Page Path
- HOME > J Musculoskelet Trauma > Volume 39(2); 2026 > Article
-
Original Article
- Biomechanical comparison of anatomically precontoured patellar plate, anterior tension wiring through cannulated screws, and double-sided plating in patellar fractures using a synthetic bone model
- Abdullah M. Aljeaid1,*, Wonseok Choi2,*, Jeong-Seok Choi2, Youngsig Choi3, Jiyeon Bae3, Jong-Keon Oh2, Jae-Woo Cho2
-
Journal of Musculoskeletal Trauma 2026;39(2):130-139.
DOI: https://doi.org/10.12671/jmt.2025.00353
Published online: April 7, 2026
1Department of Orthopedic Surgery, Prince Sultan Military Medical City, Riyadh, Saudi Arabia
2Department of Orthopedic Surgery, Korea University Guro Hospital, Korea University School of Medicine, Seoul, Korea
3Jeil Medical Corporation R&D Center, Seoul, Korea
- Correspondence to: Jae-Woo Cho Department of Orthopedic Surgery, Korea University Guro Hospital, 148 Gurodong-ro, Guro-gu, Seoul 08308, Korea Tel: +82-2-2626-1869 Email: jaewoocho@korea.ac.kr
- *Abdullah M. Aljeaid and Wonseok Choi contributed equally to this study as co-first authors.
• Received: November 14, 2025 • Revised: February 6, 2026 • Accepted: February 10, 2026
© 2026 The Korean Orthopaedic Trauma Association
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/4.0/) which permits unrestricted noncommercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
- 863 Views
- 23 Download
Abstract
-
Background Patellar fractures are common injuries that require stable fixation to achieve optimal healing and restoration of knee function. This study aimed to analyze the mechanical properties of an anatomically precontoured patellar plate and to compare its maximum tensile load-bearing capacity with that of anterior tension wiring through cannulated screws and double-sided plating for the fixation of patellar fractures.
-
Methods Artificial Sawbones with a standardized transverse fracture line were used to simulate patellar fractures. Each sawbone was attached to polyester bands, and this fracture model was applied consistently across all test samples. To evaluate mechanical properties of the anatomically precontoured patellar plate (model code 25-ANPA-209) made of ASTM F67 titanium, static tensile strength testing and dynamic tensile strength testing were performed, with seven samples prepared for each test. For comparison of maximum tensile load capacity among the anatomically precontoured patellar plate, anterior tension wiring through cannulated screws, and double-sided plating, five samples were prepared for each fixation group. All specimens were tested using a tension/compression testing machine.
-
Results In the static tensile strength test, all seven samples exhibited a maximum tensile load capacity above 844 N without any fractures or failure points. The dynamic tensile strength test showed that all seven samples completed 10,000 cycles without deformation or damage to the anatomically precontoured patellar plate. When comparing maximum tensile load capacity, the anatomically precontoured patellar plate exhibited a significantly higher maximum tensile load-bearing capacity than anterior tension wiring through cannulated screws and double-sided plating.
-
Conclusions The anatomically precontoured patellar plate demonstrated satisfactory mechanical performance, successfully meeting the criteria of both static and dynamic tensile strength testing, and showed superior maximum tensile load-bearing capacity compared with the other fixation methods evaluated. These findings suggest that the anatomically precontoured patellar plate may represent a reliable fixation option for the management of patellar fractures.
-
Level of evidence V.
Introduction
Patellar fractures are rare, comprising merely 0.5%–1.5% of total bone fractures [1]. The primary objective in managing patellar fractures is to achieve accurate anatomical alignment of the fracture and articular surface while providing stable fixation to enable early knee joint rehabilitation [2]. Several approaches have been used in recent decades to stabilize patellar fractures, with various clinical and biomechanical investigations comparing and evaluating these approaches [3,4]. Traditional tension-band wiring with K-wires has been commonly employed to treat patellar fractures by converting the tensile forces of the quadriceps on the anterior surface of the patella into compressive forces at the articular surface. Modified techniques using cannulated screws with anterior tension wiring have also been developed to provide enhanced stability [5]. Despite their potential to yield favorable clinical outcomes, these methods are associated with several drawbacks, including the possibility of pin migration, which can lead to soft tissue irritation, and low mechanical properties, which are a risk factor for loss of reduction and thus are not suitable for comminuted patellar fractures [6,7].
Nowadays, plates are a promising alternative for the fixation of patellar fractures. These implants are characterized by their relatively smaller size and versatile design, offering distinct advantages over traditional techniques (tension-band wiring with K-wires or cannulated screws). Multiple biomechanical studies have shown superior outcomes of patellar plates compared with traditional fixations. Besides being biomechanically robust, patellar plates offer further advantages. They are favorable for comminuted fractures, reducing complications and minimizing reoperation procedures [8]. The empty holes in the plate can be effectively used for suture fixation of the retinaculum or tendinous tissues (quadriceps and patellar tendons). However, there are concerns associated with their use. For example, low-profile mesh plates require extensive intraoperative contouring to fit the patella's anatomy, whereas locking plates, with their uniplanar anterior surface design, provide inadequate coverage for comminuted inferior pole fractures [9,10]. Similarly, with double-sided plating, collisions of the drill with already inserted screws on the opposite side might occur [11].
Therefore, we designed our plate to address the potential disadvantages of other patellar plates. Specifically, the plate was designed to fit the anterior surface of the patella with a low-profile so that bending of the plate would not be necessary and to cover the inferior pole of patella.
We hypothesized that anterior plating using an anatomically precontoured patellar plate would demonstrate comparable or superior maximum load-bearing capacity compared with other fixation methods, including anterior tension wiring using cannulated screws and double-sided plating.
This study aimed to perform a biomechanical analysis of the anatomically precontoured patellar plate and compare its maximum tensile load-bearing capacity to anterior tension wiring through cannulated screws and double-sided plating for patellar fractures.
Methods
This biomechanical study was conducted at the Jeil Medical Corporation Test Lab in Seoul, Korea. Institutional Review Board approval was not required as this study utilized artificial sawbone models.
Synthetic bone blocks with a density of 30 pound per cubic foot (PCF; Sawbones, model 1522-04, Pacific Research Laboratories) with dimensions of 130 mm×180 mm×40 mm were used for biomechanical testing. Thirty PCF was chosen to replicate the characteristics of the human patella, which has a compressive strength between 3 and 30 MPa, and a tensile strength of 2–20 MPa [12]. We developed an artificial patellar fracture model (width, 44 mm; thickness, 20 mm) composed of cortical and cancellous bone, attached to a polyester band (width, 24 mm; thickness, 12 mm) to simulate the quadriceps and patellar tendons, representing the knee joint's extensor mechanism. We created a transverse fracture line on the middle of the sawbone based on our previous study, which included using a three-dimensional computed tomography scan to analyze the location and frequency of fracture lines in patellar fractures [13]. This transverse fracture model was selected for several important clinical reasons. First, in comminuted patellar fractures (type C3 according to the AO/OTA classification), the surgical strategy involves converting the complex fracture pattern to a simplified configuration using auxiliary fixation methods such as screws and mini-plates before applying the main definitive fixation [2,13]. This approach neutralizes vertical fracture lines, coronal splits, or satellite fragments, effectively reducing a type C3 fracture to a type C1 pattern with a primary horizontal fracture line [13]. Second, the transverse fracture model allows for consistent and reproducible testing across all samples, eliminating variables associated with complex fracture geometries. Most importantly, this model represents the biomechanically critical condition where the main fixation construct must resist tensile forces along the primary horizontal fracture line—the predominant mechanism of clinical fixation failure, nonunion, and delayed union in patellar fractures [14-16].
The biomechanical tests were conducted using a tension/compression testing machine (Instron) via a custom-made jig designed to control the location and motion of the parts. The jig was fixed to the testing machine using screws. The lower part of the sample, representing the patellar tendon, was connected to the jig with an M-6 stainless steel D-type fixation ring. The upper part of the polyester band, representing the quadriceps tendon, was affixed to the jig using another M-6 stainless steel D-type fixation ring. This fixation ring was linked to a 3.3 mm metal cable, secured to the jig with screws. The polyester band angle connected to the sawbone was set at lower 60°, upper 60°, and final 120°, where maximum tension of the quadriceps muscle occurs (Fig. 1).
Our biomechanical test consisted of two parts. The first part analyzed the mechanical properties (static tensile strength test and dynamic tensile strength test) of our designed implant, the anatomically precontoured patellar plate (Jeil Medical Corp.) (Fig. 2). The second part compared the maximum tensile load-bearing capacity between the anatomically precontoured patellar plate, anterior tension wiring through cannulated screws, and double-sided plating.
The anatomically precontoured patellar plate was applied to the anterior surface of the patella, with two cortical screws (diameter, 2.8 mm; length, 46 mm) inserted from the inferior to the superior aspect of the patella, perpendicular to the transverse fracture line. One cortical screw was inserted in the proximal fragment (diameter, 2.5 mm; length, 12 mm) and two cortical screws in the distal fragment (diameter, 2.5 mm; length, 12 mm) to fit the plate against the anterior surface. Three locking screws (diameter, 2.5 mm; length, 12 mm) in the proximal fragment and one locking screw (diameter, 2.5 mm; length, 12 mm) in the distal fragment were added in the locking screw holes of the plate. The tension wiring through cannulated screws was performed with two headless cannulated screws (diameter, 4 mm; length, 36 mm) and a cerclage wire (diameter, 1 mm) used as a tension construct. In double-sided plating, following the technique described by Wild et al. [11,17,18], bilateral fixed-angle plates were applied to the medial and lateral borders of the patella. Specifically, two 2.8-mm small-fragment plates (Jeil Medical Corp.) with six holes were applied on both sides of the patella, which were placed to insert three locking screws perpendicular to the surface of the plate in the proximal and the distal fragment at each side (screw diameter, 2.8 mm; length, 20‒40 mm). Plates were placed in different sagittal planes to prevent screw collisions. Screws were inserted perpendicular to the screw holes and longest screws up to 40 mm were inserted. During instrumentation, screw trajectories from the medial and lateral plates occasionally intersected within the limited thickness of the patellar model. When screw collision was anticipated or encountered, screw length was reduced incrementally to avoid interference while maintaining bicortical or near-bicortical purchase when possible. This approach was applied consistently across all specimens to ensure reproducibility of the construct configuration (Fig. 3).
Seven samples of precontoured plates were tested. After applying a preload of 100 N, a tensile load was applied at a speed of 5 N/min. Testing protocol focused on construct survival as the endpoint. A threshold of 844 N was established as the minimum acceptable load-bearing capacity, reflecting a safety factor of two times the maximum load value of 422 N that the patellofemoral joint receives during walking [19]. Although the value reported by Matthews et al. represents patellofemoral joint reaction force, this value was used as a reference load because the quadriceps–patellar tendon complex transmits tensile forces across the patella during knee extension, and previous biomechanical studies have used comparable magnitudes to simulate physiologic loading conditions of the extensor mechanism [20,21]. These studies support the use of simplified tensile loading models to represent the forces transmitted through the patella during knee extension. The test was continued with progressively increasing load to evaluate the maximum load-bearing capacity of the construct. Failure was defined as fracture of the plate or sawbone, screw pull-out, or visible structural damage to the fixation construct. The maximum load reached during testing and the mode of failure, if present, were recorded for each specimen.
Seven samples of precontoured plates were tested, each subjected to a preload of 100 N. This preload was applied to remove slack and ensure consistent initial tension in the loop simulating the patellar tendon and quadriceps prior to cyclic loading. Each sample was then subjected to sinusoidal cyclic loading between 100 N and 300 N for 10,000 cycles at a frequency of 1 Hz (R-ratio, 0.33). The cyclic loading range of 100–300 N was selected based on previous biomechanical studies indicating that physiologic tensile loads across the patella during routine activities typically fall within this range [20,22]. After completion of cyclic loading, each patellar plate sample was examined for damage [22]. The testing protocol focused on construct survival as the endpoint. The acceptance criterion was no damage to the plate after 10,000 cycles. Assessment of construct integrity after cyclic loading was performed by visual inspection for plate deformation, screw loosening, or structural damage. Quantitative measurements of interfragmentary displacement or construct stiffness were not performed in this study.
Five samples were prepared for each fixation construct as follows: the anatomically precontoured patellar plate, anterior tension wiring through cannulated screws, and double-sided plating. The maximum tensile load was applied to each sample, and results were recorded using a tension/compression testing machine. Normality was assessed using the Shapiro-Wilk test (anterior tension wiring: W=0.8506, P=0.1963; anatomical plate: W=0.6983, P=0.0092; double-sided plating: W=0.9517, P=0.7494). Homogeneity of variance was confirmed using Levene’s test (F(2,12)=1.3139, P=0.3048). Given the robustness of one-way ANOVA to moderate deviations from normality in balanced experimental designs, one-way ANOVA was used to compare the maximum tensile load-bearing capacity among the three fixation methods, followed by Tukey’s honestly significant difference (HSD) post-hoc testing.
To ensure the robustness of the statistical inference, a nonparametric sensitivity analysis was additionally performed. The Kruskal-Wallis test demonstrated a significant difference in maximum tensile load among fixation constructs (H=12.50, P=0.0019). Post-hoc pairwise comparisons using Dunn’s test with Bonferroni correction confirmed significant differences between all fixation methods (adjusted P=0.0238 for all comparisons). Importantly, the nonparametric analysis demonstrated the same pattern of significant differences among fixation constructs as observed in the parametric one-way ANOVA with Tukey’s HSD test, supporting the robustness of the primary findings.
Results
All seven samples passed the static tensile strength test and were capable of bearing a load above 844 N. The maximum tensile load applied was 1,360.2 N, and the minimum was 1,216.2 N, with a standard deviation of 56.51. No construct failure was observed within the loading range achieved during testing, which was a failure criterion for this test. No deformation of the fixation constructs or fracture models was observed in any of the samples.
All seven samples completed 10,000 cycles without deformation or structural damage. Visual inspection after cyclic loading revealed no evidence of plate deformation, screw loosening, or construct failure. Quantitative measurements of interfragmentary displacement or stiffness were not performed. All plates maintained their original contour without evidence of plastic deformation. The screw-plate interfaces showed no signs of loosening or toggle. No gross displacement or separation was evident at the fracture interface that would indicate construct instability.
The individual maximum tensile loads for each sample and the corresponding mean (SD) values for each group are provided in Table 1. One-way analysis of variance results for maximum tensile load among study groups are summarized in Table 2. The results revealed significant differences in the maximum tensile load between the different fixation groups. The anatomically precontoured patellar plate group had the highest mean maximum tensile load at 2,242.93 N (SD, 120.56), followed by the anterior tension wiring through cannulated screws group with a mean of 1,954.43 N (SD, 64.87), and the double-sided plating group with a mean of 1,255.17 N (SD, 231.72).
In the post-hoc tests, all group comparisons were significant at the 0.05 level (Table 3). The anatomically precontoured patellar plate group had a significantly greater tensile load than both the cannulated screw through anterior tension wiring group and the double-sided plating group. Similarly, the anterior tension wiring through cannulated screws group had a significantly greater tensile load than the double-sided plating group.
Discussion
The present study revealed that the anatomically precontoured patellar plate demonstrated adequate mechanical performance under physiologic-range cyclic loading, with no catastrophic failure observed during 10,000 loading cycles. This patellar plate withstood loads ≥844 N without construct failure and remained stable throughout 10,000 cycles of nondestructive dynamic tensile loading (100–300 N). The anatomically precontoured patellar plate was the most capable of bearing a maximum tensile load compared to anterior tension wiring through cannulated screws and double-sided plating. All load-displacement curves showed a consistent pattern with minimal or no deviation in all samples of the anatomically precontoured patellar plate. Although physiologic tensile loads across the patella during routine activities are lower than the ultimate loads measured in this study, greater load-bearing capacity may provide an additional safety margin against unexpected peak loads. Therefore, the higher ultimate load observed in the anatomically precontoured plate construct may indicate a greater mechanical reserve under extreme loading conditions.
Although comminuted patellar fractures are quite common, we applied our biomechanical test to the transverse fracture pattern for two main reasons. First, comminuted type C3 patellar fractures (34C3 according to the current AO/OTA classification) typically feature a primary horizontal fracture line, while additional vertical lines, coronal splits, or satellite fragments can be neutralized to convert the fracture pattern to type C1 [13]. Second, using a simplified transverse pattern allowed us to create identical fractures in all Sawbones samples for consistent testing.
Stoffel et al. [23] conducted a biomechanical investigation of anterior variable-angle locked plating versus tension-band wiring of simple and complex patellar fractures. Their findings showed that anterior locked plating of both simple and complex patellar fractures resulted in less interfragmentary displacement under extended cyclic loading. Similarly, Thelen et al. [22] performed a biomechanical analysis comparing bilateral, polyaxial, fixed-angle plates to modified tension wiring with K-wires and cannulated screws with anterior tension wiring. They found that the plate is significantly stronger, with less fracture gap dehiscence than other osteosynthesis methods. Another study conducted biomechanical cadaveric testing of a fixed-angle plate compared with tension-band wiring and screw fixation in transverse patellar fractures. Both wiring and screw constructs showed significant fracture displacement, whereas the plate showed no significant fracture gap widening [24]. In daily activities, most of the tension around the patella is within 300 N, as recorded in previous biomechanical tests [22,23]. In the present study, our anatomically precontoured patellar plate passed the dynamic tensile load of 300 N.
In general, stable fixation is crucial in patellar fracture fixation, especially in the comminuted pattern. Wagner et al. [3] conducted a biomechanical comparison of a 3.5 mm anterior locking plate to cannulated screws with anterior tension-band wiring in comminuted patellar fractures. The findings revealed that the plate biomechanically provides better primary stability compared to cannulated screws with anterior tension-band wiring. Traditional tension-band wiring with cannulated screws or K-wires, while widely used, has been associated with complications including pin migration, soft tissue irritation, and symptomatic hardware that may require additional surgery for removal [16]. Furthermore, loss of reduction is another complication of these fixation methods [14]. Therefore, stable fixation is necessary, and our anatomically precontoured patellar plate may provide a reliable solution to the potential complications of traditional fixation constructs.
The inclusion of double-sided plating as a comparator in our study warrants clarification, as this technique may not be the most commonly used method for simple transverse fractures. However, bilateral plating using fixed-angle plates applied to the medial and lateral borders of the patella has been established as a viable and effective treatment option for patellar fractures, with several clinical studies demonstrating favorable outcomes [11,17,18]. These studies validate double-sided plating as a clinically relevant comparator. Contrary to previous studies, our study demonstrated that double-sided plating showed inferior mechanical stability compared to anterior tension wiring. This discrepancy may be attributed to differences in plate design and specifications used across studies, as well as variations in screw length and positioning that could affect construct rigidity. Furthermore, bilateral plating represents an alternative plating strategy that differs from anterior single-plate fixation, making it an appropriate comparison to evaluate the relative biomechanical advantages of different plate configurations. Our study therefore contributes to the understanding of how different plate positioning strategies—anterior single-plate versus double-sided plates—perform under standardized biomechanical testing conditions.
There are some limitations to this study that should be considered when interpreting the findings. First, our biomechanical study is not clinically verified and needs to be followed by a clinical study. While our findings require clinical validation, Moore et al. [25] have reported good to excellent functional outcomes following fixed-angle plate fixation of comminuted patellar fractures in a retrospective series of 20 patients (mean follow-up 154 weeks).
Second, the use of synthetic bone models, while providing consistency and reproducibility, does not fully replicate the biological and biomechanical properties of human bone, including bone quality variations, fracture healing responses, and soft tissue interactions. However, the primary advantage of synthetic bone models lies in their standardized material properties, which eliminate variability inherent in cadaveric specimens and allow for controlled comparative biomechanical testing under identical conditions. To minimize these potential sources of bias, we implemented the following standardization measures: all specimens were prepared and instrumented by a single experienced orthopedic surgeon to ensure consistency in surgical technique; screw insertion was performed using a standardized torque driver set at uniform torque settings across all specimens; and implant positioning was verified by photographic documentation to ensure reproducibility. Despite these precautions, minor variations in bone-implant interface contact and screw purchase within the synthetic bone material may still have occurred, particularly in the double-sided plating group where bilateral symmetric placement is more technically demanding. These factors may have contributed to the observed variability in biomechanical performance and represent an inherent limitation of ex vivo biomechanical testing that should be considered when interpreting our results. Third, although our study was limited to the transverse fracture pattern, this model was specifically chosen to represent the biomechanical condition after conversion of complex comminuted fractures to a simplified configuration using auxiliary fixation, as is standard in clinical practice. In comminuted patellar fractures, additional fixation modalities such as screws or mini-plates are employed to neutralize secondary fracture lines and convert the complex pattern into a primary horizontal fracture line, upon which the main definitive fixation is applied [13]. Therefore, our transverse fracture model reflects the clinically relevant scenario where the main fixation construct must effectively resist tensile forces along the primary horizontal fracture line—the predominant mechanism of fixation failure, nonunion, and delayed union in patellar fractures [14,15]. Our uniaxial tensile loading protocol was therefore specifically designed to evaluate this primary failure mechanism under controlled conditions, enabling standardized biomechanical comparison among fixation techniques. Fourth, the small sample size of five specimens per group in the comparative testing represents a limitation that may affect the statistical power of our findings. However, the use of synthetic bone models with consistent material properties reduces inter-specimen variability compared to biological specimens, and the statistically significant differences observed between groups suggest that the sample size was adequate to detect meaningful biomechanical differences. Notably, the double-sided plating group exhibited greater variability in our results, which may be explained by the technical sensitivity of this construct. Double-sided plating requires precise bilateral plate placement and symmetric screw positioning, and minor variations in plate contouring, screw length selection, or screw trajectory between specimens could substantially affect the overall construct stability and load distribution, leading to increased variability in biomechanical performance. Finally, our cyclic testing protocol evaluated construct survival without quantifying interfragmentary displacement at the fracture site. Future studies employing optical tracking systems (e.g., digital image correlation) or extensometers would enable detailed characterization of displacement evolution and stiffness degradation under cyclic loading. Nevertheless, our findings demonstrate that the anatomically precontoured plate can withstand physiologically relevant cyclic loads without catastrophic failure, which is clinically relevant for early postoperative rehabilitation protocols.
It should also be noted that the double-sided plating construct used in this study was not identical to the specific implant systems evaluated in previous biomechanical studies. Variations in plate geometry, screw trajectory, and screw length selection may influence construct rigidity in bilateral plating configurations. Therefore, the inferior mechanical performance observed in the present study should be interpreted within the context of the specific implant configuration tested, rather than as a general conclusion regarding all double-sided plating techniques for patellar fractures.
In conclusion, the anatomically precontoured patellar plate offered stable fixation for patellar fracture models. The mechanical analysis of this plate showed that it could withstand maximum static and dynamic tensile loads without any damage or failure and was the most capable of bearing a maximum tensile load. These findings support the potential clinical utility of the anatomically precontoured patellar plate as a main fixation construct for both simple transverse and converted complex patellar fractures, although cadaveric study or clinical validation is needed to confirm these biomechanical advantages.
-
Author contributions
Conceptualization: YC, JB, JWC. Methodology: YC, JB. Data curation: YC, JB, JSC. Formal analysis: AMA, WC. Project administration: JWC. Supervision: JKO, JWC. Writing-original draft: AMA, WC. Writing-review & editing: AMA, WC, YC, JB, JSC, JKO, JWC. All authors read and approved the final manuscript.
-
Conflicts of interest
No potential conflict of interest relevant to this article was reported.
-
Funding
This study was partially funded by Seoul R&BD Program (BT230060).
-
Data availability
Contact the corresponding author for data availability.
-
Acknowledgments
The authors thank the Jeil Medical Corporation for their support in conducting the biomechanical tests.
-
Supplementary materials
None.
Article Information
Fig. 1.
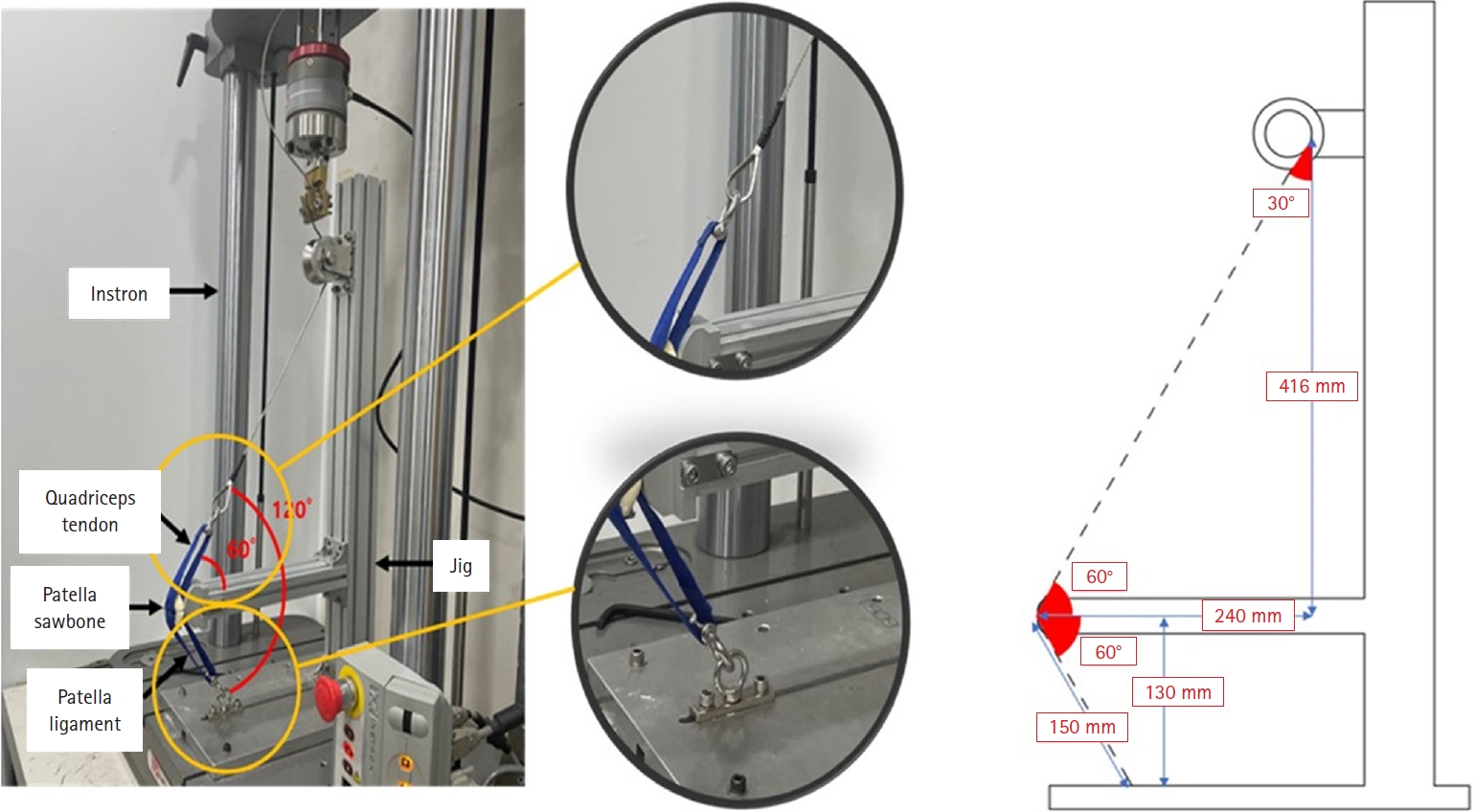
Biomechanical testing environment illustrating the experimental setup, including the Instron testing machine, simulated quadriceps tendon, patellar sawbone, and patellar ligament, with detailed measurements and joint angles. A knee flexion angle of 120° was maintained consistently throughout testing of all specimens.
Fig. 2.

Anatomically precontoured patellar plate fabricated from ASTM F67 titanium (model code 25-ANPA-209). Two 2.8-mm cortical screws can be inserted from the inferior to the superior fragment. Three 2.5-mm cortical screws and four 2.5-mm locking screws can be inserted from the anterior aspect of the plate.
Fig. 3.
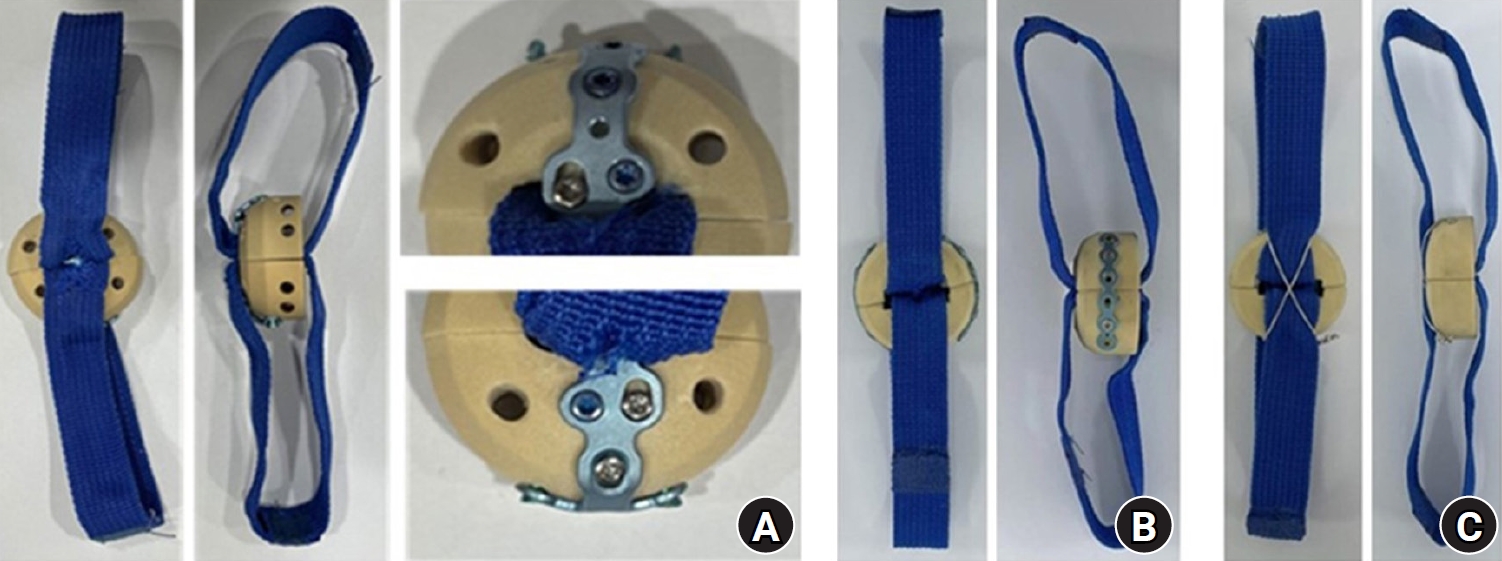
Frontal and lateral views of each fixation construct: (A) anatomically precontoured patellar plate, (B) double-sided plating, and (C) anterior tension wiring through cannulated screws. All specimens were prepared using synthetic sawbone models with identical transverse fracture patterns and simulated quadriceps and patellar tendon attachments (blue bands) to ensure standardized biomechanical testing conditions.
Table 1.
Maximum tensile load applied on each sample
Table 2.
One-way analysis of variance results for maximum tensile load among study groups
| Source | Sum of squares | Degrees of freedom | Mean square | F-value | P-value |
|---|---|---|---|---|---|
| Between groups | 2,579,780 | 2 | 1,289,890 | 53.42 | <0.001** |
| Within groups (error) | 289,745 | 12 | 24,145 | - | - |
| Total | 2,869,525 | 14 | - | - | - |
Table 3.
Post-hoc pairwise comparisons of maximum tensile load among fixation groups (Tukey HSD test)
| Group comparison | Mean difference (N) | SE | 95% CI | P-value |
|---|---|---|---|---|
| Anterior tension wiring through cannulated screws vs. anatomical plate | ‒288.50 | 98.28 | ‒519.45 to ‒57.55 | 0.031* |
| Anterior tension wiring through cannulated screws vs. double-sided plating | 699.26 | 98.28 | 468.31 to 930.21 | <0.001** |
| Anatomical plate vs. double-sided plating | 987.76 | 98.28 | 756.81 to 1,218.71 | <0.001** |
- 1. Sebastian P, Michael Z, Frederik G, et al. Influence of patella height after patella fracture on clinical outcome: a 13-year period. Arch Orthop Trauma Surg 2022;142:1557-61.ArticlePubMedPDF
- 2. Cho JW, Kent WT, Cho WT, et al. Miniplate augmented tension-band wiring for comminuted patella fractures. J Orthop Trauma 2019;33:e143-50.ArticlePubMed
- 3. Wagner FC, Neumann MV, Wolf S, et al. Biomechanical comparison of a 3.5 mm anterior locking plate to cannulated screws with anterior tension band wiring in comminuted patellar fractures. Injury 2020;51:1281-7.ArticlePubMed
- 4. Lee KH, Lee Y, Lee YH, Cho BW, Kim MB, Baek GH. Biomechanical comparison of three tension band wiring techniques for transverse fracture of patella: Kirschner wires, cannulated screws, and ring pins. J Orthop Surg (Hong Kong) 2019;27:2309499019882140.ArticlePubMedPDF
- 5. Hsu KL, Chang WL, Yang CY, Yeh ML, Chang CW. Factors affecting the outcomes of modified tension band wiring techniques in transverse patellar fractures. Injury 2017;48:2800-6.ArticlePubMed
- 6. Banks KE, Ambrose CG, Wheeless JS, Tissue CM, Sen M. An alternative patellar fracture fixation: a biomechanical study. J Orthop Trauma 2013;27:345-51.ArticlePubMed
- 7. Avery MC, Jo S, Chang A, et al. Cannulated screw prominence in tension band wiring of patella fractures increases fracture gapping: a cadaver study. Clin Orthop Relat Res 2019;477:1249-55.ArticlePubMedPMC
- 8. Tsotsolis S, Ha J, Fernandes AR, et al. To plate, or not to plate? A systematic review of functional outcomes and complications of plate fixation in patellar fractures. Eur J Orthop Surg Traumatol 2023;33:3287-97.ArticlePubMedPDF
- 9. Verbeek DO, Hickerson LE, Warner SJ, Helfet DL, Lorich DG. Low profile mesh plating for patella fractures: video of a novel surgical technique. J Orthop Trauma 2016;30 Suppl 2:S32-3.ArticlePubMed
- 10. Wurm S, Buhren V, Augat P. Treating patella fractures with a locking patella plate: first clinical results. Injury 2018;49 Suppl 1:S51-5.ArticlePubMed
- 11. Wild M, Thelen S, Jungbluth P. Fixed-angle plates in patella fractures: a pilot cadaver study. Eur J Med Res 2011;16:41-6.ArticlePubMedPMC
- 12. Wurm S, Augat P, Buhren V. Biomechanical assessment of locked plating for the fixation of patella fractures. J Orthop Trauma 2015;29:e305-8.ArticlePubMed
- 13. Cho JW, Yang Z, Lim EJ, et al. Multifragmentary patellar fracture has a distinct fracture pattern which makes coronal split, inferior pole, or satellite fragments. Sci Rep 2021;11:22836.ArticlePubMedPMCPDF
- 14. Smith ST, Cramer KE, Karges DE, Watson JT, Moed BR. Early complications in the operative treatment of patella fractures. J Orthop Trauma 1997;11:183-7.ArticlePubMed
- 15. Klassen JF, Trousdale RT. Treatment of delayed and nonunion of the patella. J Orthop Trauma 1997;11:188-94.ArticlePubMed
- 16. Hoshino CM, Tran W, Tiberi JV, et al. Complications following tension-band fixation of patellar fractures with cannulated screws compared with Kirschner wires. J Bone Joint Surg Am 2013;95:653-9.ArticlePubMed
- 17. Wild M, Eichler C, Thelen S, Jungbluth P, Windolf J, Hakimi M. Fixed-angle plate osteosynthesis of the patella: an alternative to tension wiring. Clin Biomech (Bristol) 2010;25:341-7.ArticlePubMed
- 18. Wild M, Fischer K, Hilsenbeck F, Hakimi M, Betsch M. Treating patella fractures with a fixed-angle patella plate: a prospective observational study. Injury 2016;47:1737-43.ArticlePubMed
- 19. Matthews LS, Sonstegard DA, Henke JA. Load bearing characteristics of the patello-femoral joint. Acta Orthop Scand 1977;48:511-6.ArticlePubMed
- 20. Carpenter JE, Kasman RA, Patel N, Lee ML, Goldstein SA. Biomechanical evaluation of current patella fracture fixation techniques. J Orthop Trauma 1997;11:351-6.ArticlePubMed
- 21. Scilaris TA, Grantham JL, Prayson MJ, Marshall MP, Hamilton JJ, Williams JL. Biomechanical comparison of fixation methods in transverse patella fractures. J Orthop Trauma 1998;12:356-9.ArticlePubMed
- 22. Thelen S, Schneppendahl J, Baumgartner R, et al. Cyclic long-term loading of a bilateral fixed-angle plate in comparison with tension band wiring with K-wires or cannulated screws in transverse patella fractures. Knee Surg Sports Traumatol Arthrosc 2013;21:311-7.ArticlePubMedPDF
- 23. Stoffel K, Zderic I, Pastor T, et al. Anterior variable-angle locked plating versus tension band wiring of simple and complex patella fractures - a biomechanical investigation. BMC Musculoskelet Disord 2023;24:279.ArticlePubMedPMCPDF
- 24. Thelen S, Schneppendahl J, Jopen E, et al. Biomechanical cadaver testing of a fixed-angle plate in comparison to tension wiring and screw fixation in transverse patella fractures. Injury 2012;43:1290-5.ArticlePubMed
- 25. Moore TB, Sampathi BR, Zamorano DP, Tynan MC, Scolaro JA. Fixed angle plate fixation of comminuted patellar fractures. Injury 2018;49:1203-7.ArticlePubMed
References
Figure & Data
REFERENCES
Citations
Citations to this article as recorded by 
 ePub Link
ePub Link Cite
CiteBiomechanical comparison of anatomically precontoured patellar plate, anterior tension wiring through cannulated screws, and double-sided plating in patellar fractures using a synthetic bone model
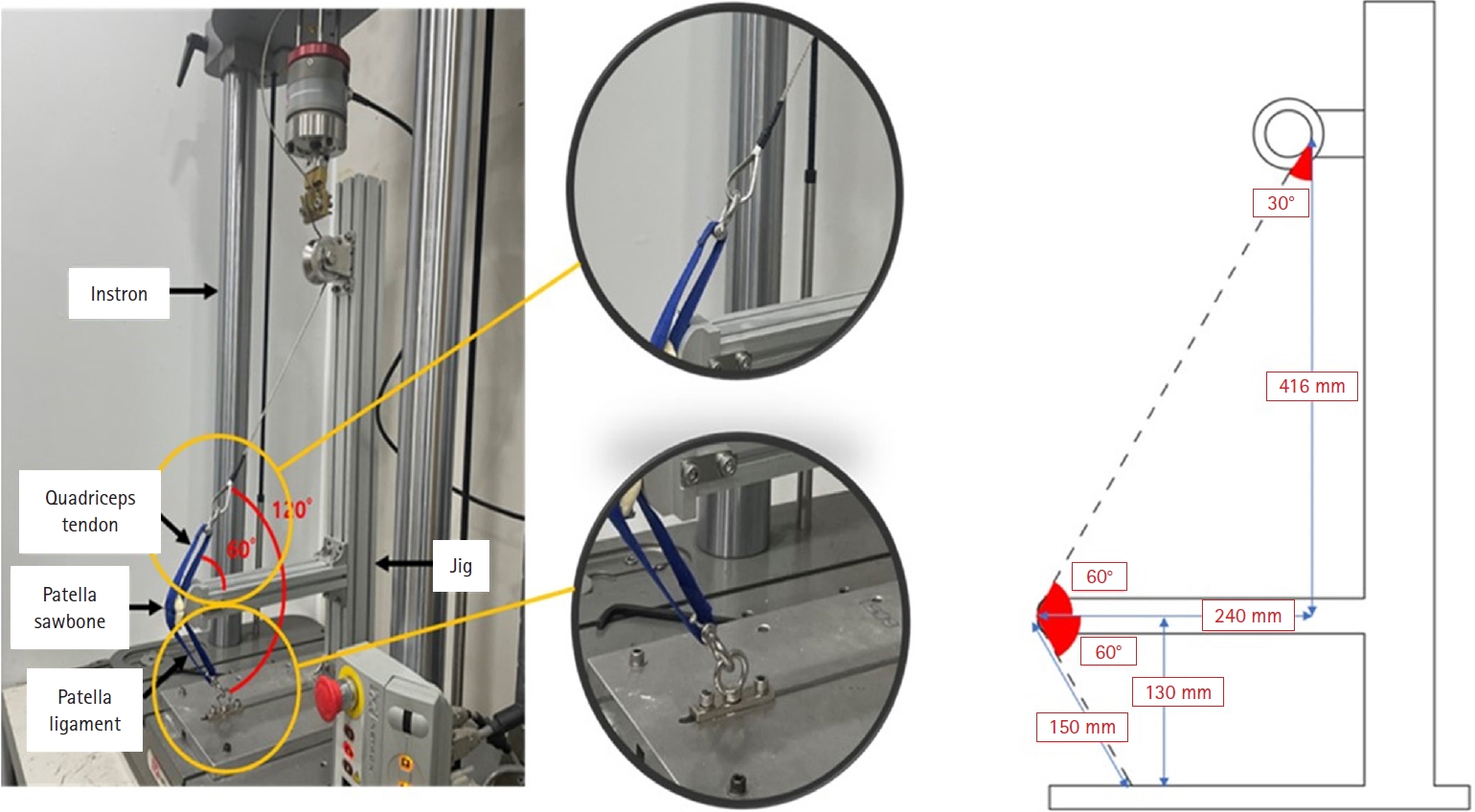

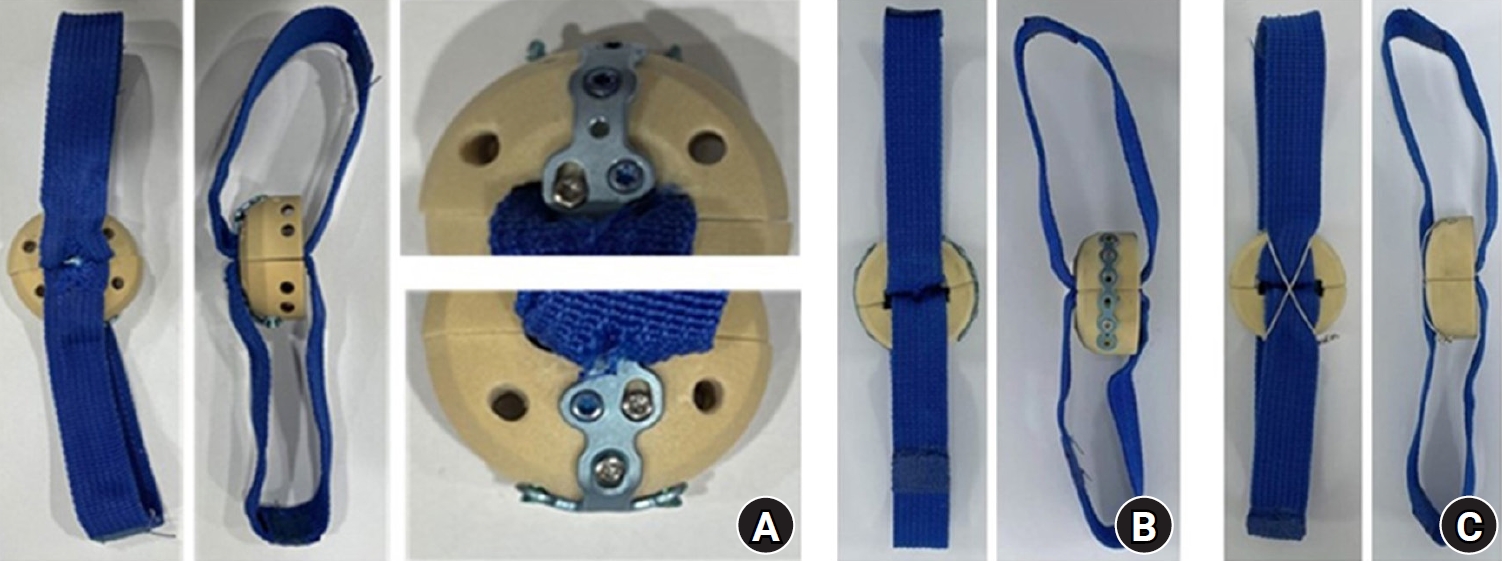
Fig. 1. Biomechanical testing environment illustrating the experimental setup, including the Instron testing machine, simulated quadriceps tendon, patellar sawbone, and patellar ligament, with detailed measurements and joint angles. A knee flexion angle of 120° was maintained consistently throughout testing of all specimens.
Fig. 2. Anatomically precontoured patellar plate fabricated from ASTM F67 titanium (model code 25-ANPA-209). Two 2.8-mm cortical screws can be inserted from the inferior to the superior fragment. Three 2.5-mm cortical screws and four 2.5-mm locking screws can be inserted from the anterior aspect of the plate.
Fig. 3. Frontal and lateral views of each fixation construct: (A) anatomically precontoured patellar plate, (B) double-sided plating, and (C) anterior tension wiring through cannulated screws. All specimens were prepared using synthetic sawbone models with identical transverse fracture patterns and simulated quadriceps and patellar tendon attachments (blue bands) to ensure standardized biomechanical testing conditions.
Fig. 1.
Fig. 2.
Fig. 3.
Biomechanical comparison of anatomically precontoured patellar plate, anterior tension wiring through cannulated screws, and double-sided plating in patellar fractures using a synthetic bone model
| Case | Anterior tension wiring through cannulated screws | Anatomically precontoured patellar plate | Double-sided plating | |
|---|---|---|---|---|
| 1 | 1,983.98 | 2,211.56 | 971.95 | |
| 2 | 1,845.79 | 2,166.29 | 1,258.35 | |
| 3 | 1,980.78 | 2,455.55 | 1,608.03 | |
| 4 | 1,948.64 | 2,173.29 | 1,157.97 | |
| 5 | 2,012.98 | 2,207.97 | 1,279.56 | |
| Mean±SD | 1,954.43±64.87 | 2,242.93±120.56 | 1,255.17±231.72 | |
| Median (IQR) | 1,980.78 (1,948.64–1,983.98) | 2,207.97 (2,173.29–2,211.56) | 1,258.35 (1,157.97–1,279.56) |
| Source | Sum of squares | Degrees of freedom | Mean square | F-value | P-value |
|---|---|---|---|---|---|
| Between groups | 2,579,780 | 2 | 1,289,890 | 53.42 | <0.001 |
| Within groups (error) | 289,745 | 12 | 24,145 | - | - |
| Total | 2,869,525 | 14 | - | - | - |
| Group comparison | Mean difference (N) | SE | 95% CI | P-value |
|---|---|---|---|---|
| Anterior tension wiring through cannulated screws vs. anatomical plate | ‒288.50 | 98.28 | ‒519.45 to ‒57.55 | 0.031 |
| Anterior tension wiring through cannulated screws vs. double-sided plating | 699.26 | 98.28 | 468.31 to 930.21 | <0.001 |
| Anatomical plate vs. double-sided plating | 987.76 | 98.28 | 756.81 to 1,218.71 | <0.001 |
Table 1. Maximum tensile load applied on each sample
SD, standard deviation; IQR, interquartile range.
Table 2. One-way analysis of variance results for maximum tensile load among study groups
P<0.001.
Table 3. Post-hoc pairwise comparisons of maximum tensile load among fixation groups (Tukey HSD test)
Negative values indicate the first group had lower tensile load than the second group. HSD, honestly significant difference; SE, standard error; CI, confidence interval. *P<0.05, **P<0.001.

