 E-submission
E-submission TOTA
TOTA TOTS
TOTS
Articles
- Page Path
- HOME > J Musculoskelet Trauma > Volume 39(2); 2026 > Article
-
Review Article
- Definitive fixation for traumatic pelvic ring injuries: a dynamically informed, posterior-referenced framework
-
Jeong-Hyun Koh
 , Seungyeob Sakong
, Seungyeob Sakong -
Journal of Musculoskeletal Trauma 2026;39(2):73-82.
DOI: https://doi.org/10.12671/jmt.2026.00045
Published online: March 24, 2026
Department of Orthopedic Surgery, Ajou University School of Medicine, Suwon, Korea
- Correspondence to: Seungyeob Sakong Department of Orthopedic Surgery, Ajou University School of Medicine, 164 Worldcup-ro, Yeongtong-gu, Suwon 16499, Korea Tel: +82-31-219-5220 Email: sgsy4040@gmail.com
• Received: January 13, 2026 • Revised: January 24, 2026 • Accepted: January 28, 2026
© 2026 The Korean Orthopaedic Trauma Association
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/4.0/) which permits unrestricted noncommercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
- 1,651 Views
- 37 Download
- Abstract
- Introduction
- Shared language: terms that map to decisions
- Static imaging: necessary but not sufficient
- Deconstructing the “2.5 cm myth”
- Dynamic instability assessment: resolving decision-changing uncertainty
- Translating instability into fixation: escalation along a continuum
- Definitive fixation strategy and sequencing
- Special scenarios and failure prevention
- Conclusions
- Article Information
- References
Abstract
- Optimal definitive fixation for traumatic pelvic ring injuries remains challenging because static radiographs and computed tomography, although essential for defining morphology, do not consistently predict load-dependent behavior during early mobilization. This uncertainty contributes to substantial practice variation and continued reliance on simplified displacement thresholds, such as the 2.5 cm rule. Such rules can misclassify instability by underrepresenting posterior competence and by privileging static measurements over functional behavior. In this narrative review, we propose a dynamically informed, posterior-referenced framework composed of three linked elements: (1) decision-linked terminology that explicitly distinguishes dynamic instability, radiographic change, and clinical failure; (2) selective stress-based assessment when uncertainty is likely to alter management; and (3) escalation along a fixation continuum that weighs incremental stability against operative burden. When static imaging cannot establish posterior competence with confidence, we outline selective stress-based approaches to assess pelvic ring behavior and to translate demonstrated instability into fixation selection along a defined continuum. Across all steps, the framework emphasizes minimum necessary fixation and explicitly incorporates the cost of selection as a primary decision variable. The operative question, therefore, shifts from gap width alone to clinically relevant motion and preservation of posterior competence. In doing so, this approach aims to reduce both undertreatment and overtreatment and to improve the consistency and defensibility of definitive fixation strategies across diverse practice environments.
Introduction
Determining the optimal management of traumatic pelvic ring injuries remains clinically challenging. Static radiographs and computed tomography (CT) are essential for defining morphology and planning fixation, yet they do not consistently predict how an injury will behave during early mobilization. As a result, meaningful variation persists in how similar patterns are treated across surgeons and institutions, in part because complex three-dimensional mechanics must be inferred from two-dimensional static images [1-3].
The clinical consequences of this mismatch are substantial. Underestimation of instability can lead to loss of reduction, malunion, persistent pain, and impaired function. In selected cases, it may require revision surgery with considerable morbidity. Overestimation of instability exposes patients to unnecessary operative invasiveness, greater soft-tissue burden, and implant-related complications. The central problem is therefore not simply whether to operate, but how to select fixation that controls clinically relevant instability while limiting avoidable harm from overtreatment [1,3].
Historically, the field has relied on simplified numeric thresholds because they are teachable and reproducible. Thresholds based on symphyseal diastasis or sacroiliac (SI) widening can assist early stratification, but they do not reliably capture posterior competence, ligament integrity, or load-dependent behavior. In borderline cases, a single static measurement can describe what is seen without forecasting what will occur once the ring is challenged during rehabilitation [1,2].
This review presents a dynamically informed strategy centered on two clinical priorities: posterior competence and the cost of selection. Rigid displacement thresholds—most notably the long-standing “2.5 cm rule”—can misclassify instability. We outline when uncertainty warrants stress-based assessment of behavior and how those findings translate into fixation selection along a construct continuum. The objective is not to promote a single maneuver or construct, but to provide a practical framework that remains applicable across diverse clinical environments [1,4,5].
Shared language: terms that map to decisions
To prevent inconsistent terminology from driving inconsistent surgery, instability and failure should be defined in terms that map directly to decisions. In this review, dynamic instability (Table 1) [1-3,6-11] refers to clinically relevant motion under stress or physiologic loading, regardless of the initial static appearance. This definition shifts emphasis from what an injury looks like to how the pelvic ring behaves when challenged [1,2].
A second distinction is between radiographic change and clinical failure. Radiographic change includes interval widening, minor alignment shifts, and implant loosening on follow-up imaging. These findings—particularly in the anterior ring—may occur without meaningful symptoms or functional compromise. Clinical failure refers to patient-centered deterioration—progressive loss of alignment that compromises the pelvic reference frame, persistent pain or functional limitation that delays rehabilitation, or unplanned revision. Postoperative radiographic changes after anterior fixation do not consistently correlate with poor function or revision, underscoring the risk of escalation driven by imaging alone [6,7].
The gray-zone describes cases in which static imaging does not allow confident classification as stable versus unstable and where management could reasonably differ. Gray-zone injuries are where both undertreatment and overtreatment risks are highest, and interpretation benefits from a consistent reference. In gray-zone injuries, posterior alignment and posterior competence serve as the reference frame for global stability, helping distinguish clinically meaningful anterior instability from expected postoperative variation [2,9].
This logic underpins the review. Static imaging defines morphology and informs planning; however, when uncertainty could change management, controlled stress testing becomes the relevant question. Fixation is then selected by balancing stability benefit against the incremental burden introduced by escalation [1,2]. In this framework, clinically relevant motion refers to reproducible stress- or load-dependent ring motion that plausibly threatens the maintenance of the posterior ring reference frame and/or delays mobilization and rehabilitation. Key working definitions and decision-linked terminology used throughout this review are summarized in Table 1 [1-3,6-11].
Static imaging: necessary but not sufficient
Static imaging remains central to triage and preoperative planning. Radiographs provide an initial characterization of displacement patterns, injury vectors, and associated lesions. CT with multiplanar reconstructions refines assessment of sacral fracture morphology, comminution, and pelvic anatomy relevant to safe fixation corridors. Together, these details guide construct feasibility, technical approach, and operative planning [1,2,12].
A persistent limitation is that morphology and static displacement do not consistently predict functional behavior under physiologic loading. Borderline injuries expose the gap between measured diastasis and clinically meaningful mobility. Two patients with similar symphyseal widening can represent different mechanical states depending on posterior ligament competence, comminution pattern, and mechanical coupling across the ring. Static imaging can be deceptively reassuring: some injuries displace with mobilization, whereas others heal uneventfully without fixation [2,9].
When morphology clearly indicates instability and operative stabilization is indicated, static imaging is typically sufficient for planning. When findings fall in a gray-zone and management could change, displacement thresholds should be treated as risk markers rather than decision rules. The key questions are whether posterior competence is preserved and whether reproducible, clinically relevant motion is demonstrated under stress (Fig. 1) [1,2]. This tension is most visible when practice is organized around numeric cutoffs rather than mechanical behavior. The enduring “2.5 cm rule” is the clearest example of how a single static threshold can oversimplify global pelvic stability [4,13].
Deconstructing the “2.5 cm myth”
The 2.5 cm rule persists because it is simple and historically embedded in pelvic trauma teaching. As a screening heuristic, a numeric cutoff can be useful. However, it should be interpreted as a risk marker—not a decision rule—within the posterior reference-frame logic. The problem arises when it is treated as a definitive boundary for stability across heterogeneous injury patterns and patient contexts [4,13].
A single threshold does not incorporate posterior competence or load-dependent behavior and can therefore misclassify instability. Modest static diastasis may coexist with substantial motion under stress when posterior structures are compromised, whereas larger diastasis may behave relatively stably when posterior competence is preserved. Reducing a three-dimensional mechanical problem to a single static measurement obscures the true determinant of global stability [2,4].
For the practicing surgeon, a more useful question is whether the pelvic ring shows clinically relevant motion under stress, interpreted within a posterior ring reference frame (Fig. 1). Many borderline cases are better framed as uncertainty about posterior competence rather than a measurement problem. Decision-making should therefore prioritize whether mobility is likely to jeopardize early mobilization or maintenance of reduction [1,2].
Minor postoperative changes in the anterior ring do not automatically represent clinical failure. Small interval widening or implant loosening can occur even when posterior alignment is maintained and functional recovery progresses. Revision and escalation are more appropriate when there is loss of global alignment, persistent instability, or meaningful clinical deterioration rather than isolated radiographic findings [6-8].
Accordingly, the practical question returns to behavior: whether clinically relevant motion is present and whether posterior competence is preserved [2,4].
Dynamic instability assessment: resolving decision-changing uncertainty
Dynamic assessment is a clinical principle rather than a routine test (Fig. 1). Its purpose is to reduce decision-changing uncertainty by clarifying pelvic ring behavior under controlled stress, particularly when static imaging defines morphology but cannot confidently establish posterior competence or global stability. The limitations of rigid cutoffs, exemplified by the 2.5 cm rule, help explain why behavior-based assessment becomes relevant when management hinges on borderline findings [1,2,4].
At the bedside, initial assessment and early reassessment can triage presentations that remain consistent with stability. Focused examination, symptom response during early mobilization, and serial imaging in standardized views can clarify whether alignment is maintained over time. The objective is not to “prove stability” with a single maneuver, but to determine whether uncertainty meaningfully persists after reasonable observation [2,9].
When uncertainty persists and operative planning is being considered, intraoperative fluoroscopy can provide adjunct information. Controlled stress under fluoroscopy can assess reduction behavior across standard views (anteroposterior [AP], inlet, and outlet). Because applied force and technique vary across operators, these observations are most informative when documented with method details—patient position, direction of stress, and motion pattern—rather than reduced to isolated cutoffs [2,9].
To maximize reproducibility without implying numeric thresholds, minimum documentation should specify:
• Patient position and support (e.g., supine/prone)
• Fluoroscopic views obtained (AP, inlet, and outlet)
• Stress maneuver (direction and method of force application)
• Reproducibility (consistency across repeat maneuvers)
• Qualitative motion pattern (rotational, vertical, or translational)
• Interpretation relative to posterior competence
Examination under anesthesia can serve as a confirmatory option when higher-fidelity information is expected to change management. Full muscle relaxation can improve consistency of stress application, particularly when posterior competence is uncertain and the fixation plan is near a meaningful escalation boundary. It is best used selectively for decision-changing questions rather than as a routine prerequisite [1,14].
The output of dynamic assessment should translate into mechanical decisions: whether posterior competence is preserved and whether observed motion is sufficient to threaten mobilization or reduction maintenance. Interpretation should prioritize posterior competence and reproducible ring behavior under stress rather than absolute millimeter closure. Demonstrated stable behavior may support nonoperative care or limited fixation, whereas persistent motion strengthens the rationale for prioritizing posterior stabilization within the posterior ring reference frame [1,2].
Practical limitations are clinically important. Dynamic testing lacks universal standardization, anesthesia and operating-room constraints vary, and manipulation carries risk. Evidence is heterogeneous, and thresholds for clinically meaningful motion are not consistent across studies or injury patterns. Dynamic assessment is therefore most appropriate when applied to management-relevant questions and reported transparently in context [1,14].
Translating instability into fixation: escalation along a continuum
Fixation selection is best viewed as a continuum in which stability gains must be weighed against the costs of escalation (Fig. 2). Table 2 summarizes representative constructs, decision triggers, and the primary cost of selection across this continuum [1,2,6-12,15-18]. This framework supports minimum necessary fixation: stabilizing what is demonstrably unstable while avoiding construct expansion when it is unlikely to improve patient-centered outcomes. In polytrauma and medically complex patients, added operative time, blood loss, and physiologic stress may themselves be clinically consequential; escalation should therefore be justified by a clear mechanical need [1,3]. A practical translation begins with behavior. When the ring behaves stably under the available assessment method and the clinical course remains concordant, nonoperative management or limited fixation may be reasonable, depending on morphology and patient factors. When behavior is borderline, standard constructs may be appropriate to protect alignment and facilitate mobilization. When clear mobility is demonstrated or posterior competence is compromised, escalation becomes justified. Throughout, decisions are best interpreted within a posterior ring reference frame [1,2].
Posterior stabilization should guide the primary strategy when posterior competence is compromised or strongly suspected. Posterior competence governs global load transfer and strongly influences whether anterior fixation will remain durable. In unstable patterns, posterior stabilization has been associated with fewer anterior construct failures. These observations suggest that loss of posterior competence drives anterior overload more often than isolated anterior implant insufficiency [19].
Anterior fixation is best framed as an adjunct once posterior competence is addressed. Its role is to restore anterior alignment, reduce rotational tendency, and protect posterior stabilization in patterns where anterior disruption contributes to symptoms and instability. In this context, minor radiographic changes—such as small interval widening or implant loosening—do not necessarily indicate clinical failure if posterior alignment is preserved and functional recovery is favorable. This distinction reduces escalation driven by radiographic anxiety rather than mechanical necessity [6-8].
The durability of low-profile posterior constructs, including iliosacral screw fixation, depends on patient and technical factors that should be treated as explicit decision variables. Bone quality, reduction accuracy, screw trajectory and length, corridor anatomy, and sacral comminution all influence mechanical performance. Syntheses of the literature associate loosening and failure with these factors, supporting the use of a structured risk checklist during planning rather than defaulting to low-profile constructs in mechanically unfavorable settings [15,16,20].
Escalation to more robust constructs is appropriate when standard posterior fixation is unlikely to control the injury pattern or maintain reduction. Practical triggers include a marked vertical tendency, substantial sacral comminution or compromised corridors, and inability to achieve or maintain acceptable alignment with screws alone. Options such as transiliac internal fixation (TIFI) or spinopelvic constructs can provide stronger control, but indications should remain explicit and mechanically justified [10,12,17]. Percutaneous advances, including TIFI, expand posterior options but require precise corridors [21].
The cost of selection should be incorporated as a primary decision factor. More extensive fixation increases operative complexity and soft-tissue burden compared with low-profile constructs. In selected series and pooled analyses, complex posterior constructs have been associated with higher complication rates, including infection and wound problems. These risks must be weighed against the consequences of inadequate stabilization, including loss of reduction and revision surgery. In practice, the aim remains minimum necessary fixation: secure posterior mechanics when indicated, add anterior fixation when it meaningfully supports global stability, and escalate only when standard constructs are unlikely to control demonstrated instability [3,10,11].
Definitive fixation strategy and sequencing
With fixation viewed as a continuum (Fig. 2), operative sequencing becomes a practical exercise in establishing a durable posterior ring reference frame (Fig. 1) and adding anterior stabilization only when it contributes meaningful mechanical value. Definitive fixation is most effective when planned around a clear objective: restoring and maintaining global pelvic stability while limiting unnecessary surgical burden. Posterior competence and alignment often define the reference frame that determines whether subsequent steps—particularly anterior reduction—will be meaningful and durable [1,12].
When posterior competence is compromised or uncertain, a posterior-first sequence is typically the most appropriate strategy. Conversely, an anterior-first or anterior-only approach may be reasonable only when posterior competence is clearly preserved, and the decision should still be justified within the posterior ring reference frame. Recent reviews confirm that reduction evolution favors posterior-first sequencing in unstable patterns [22]. Securing posterior alignment establishes the reference on which anterior reduction can be judged and maintained. In this setting, posterior-first fixation is not merely a preference; it is often mechanically necessary for durable anterior stabilization. Anterior constructs cannot reliably compensate for an unaddressed posterior deficit. Attempting to optimize anterior alignment in the presence of unresolved posterior instability can increase surgical burden without reliably improving global stability [12,19,23].
After posterior stabilization, reassessment under fluoroscopy can clarify whether residual anterior instability is mechanically relevant and whether an anterior adjunct is needed to maintain ring closure during mobilization. This step can also help avoid unnecessary anterior escalation when posterior mechanics are adequately controlled and anterior motion is limited [1,2].
Sequencing should also account for physiologic readiness and competing priorities in polytrauma. In patients who have undergone hemorrhage control and temporary stabilization, definitive fixation is best performed when physiology and soft-tissue conditions allow safe surgery, rather than on a rigid timeline. The choice between earlier versus delayed definitive fixation can be individualized based on hemodynamic stability, associated injuries, anticipated invasiveness, and the incremental risk introduced by escalation [3,5].
Technical feasibility is part of the strategy. Posterior fixation options vary in their demands on corridor anatomy, reduction accuracy, and intraoperative imaging. Preoperative CT planning and attention to dysmorphism are essential. Careful fluoroscopic technique reduces malposition risk and increases the likelihood that the selected construct delivers the intended stability [1,15,18].
Special scenarios and failure prevention
Gray-zone injuries managed nonoperatively require an explicit surveillance plan that reflects the same decision logic used for fixation. Early clinical reassessment and standardized serial imaging can identify cases in which alignment is not maintained during mobilization, and recent work highlights how occult instability can declare itself during follow-up despite borderline initial imaging. Conversion to surgery is most appropriate when driven by patient-centered failure, demonstrable progression that threatens global stability, or persistent mechanical symptoms that align with instability, rather than by minor radiographic change alone [2,9].
Certain patient and injury factors increase the likelihood that low-profile constructs will underperform. Poor bone quality, extensive comminution, compromised screw corridors, and malreduction can undermine posterior fixation durability and should influence the decision to augment or escalate. In these scenarios, the goal is not simply to increase fixation, but to select a construct with a realistic likelihood of controlling the observed instability, with a clear mechanical rationale for any escalation [12,15,16].
Open injuries, severe soft-tissue compromise, and contaminated fields require additional caution because the biological cost of fixation rises. When infection risk is high, construct selection should emphasize achieving essential stability with the least additional soft-tissue insult, and definitive internal fixation may need to be staged or modified based on wound management priorities. In such settings, the cost of selection is not an abstract concept but a constraint that should be stated explicitly in the decision rationale [1,3].
Failure prevention also depends on avoiding iatrogenic harm and defining failure appropriately. Malpositioned implants—particularly in the posterior ring—can produce catastrophic neurovascular complications and can convert a borderline mechanical problem into a major clinical failure. Conversely, automatic revision for isolated radiographic findings can drive unnecessary morbidity when the posterior ring reference frame is preserved and functional recovery is favorable. Revision and escalation are most appropriate when there is loss of global alignment, persistent instability, or meaningful clinical deterioration consistent with true failure [6,7,18,20].
Conclusions
Static imaging remains essential for defining morphology and planning treatment, but it does not consistently predict functional instability in borderline pelvic ring injuries. The central challenge is to identify clinically meaningful instability and to match fixation to the mechanical problem without defaulting to rigid thresholds or automatic escalation [1,2,4].
A dynamically informed strategy addresses this challenge by anchoring interpretation to posterior competence and using behavior-based assessment selectively when uncertainty is likely to change management. A posterior-referenced strategy supports minimum necessary fixation. It targets demonstrable instability, prioritizes posterior mechanics when indicated, and uses anterior fixation selectively when it adds durable mechanical benefit. This perspective is particularly relevant in polytrauma, where operative burden, timing constraints, and competing priorities are not secondary considerations but part of the outcome [1,3,5].
The practical aim is a decision framework that remains usable across diverse environments. It defines stability in behavioral terms and interprets postoperative changes within a posterior ring reference frame. Escalation is reserved for cases in which standard constructs are unlikely to control demonstrated instability. This helps avoid both undertreatment and unnecessary surgical burden and makes decision-making more consistent [1,2].
-
Author contributions
Conceptualization: JHK; SS. Methodology: JHK; SS. Investigation: JHK. Resources: JHK. Data curation: JHK. Supervision: SS. Project administration: SS. Visualization: JHK. Writing–original draft: JHK. Writing–review & editing: JHK, SS. All authors read and approved the final manuscript.
-
Conflicts of interest
No potential conflict of interest relevant to this article was reported.
-
Funding
None.
-
Data availability
Not applicable.
-
Acknowledgments
None.
-
Supplementary materials
None.
Article Information
Fig. 1.
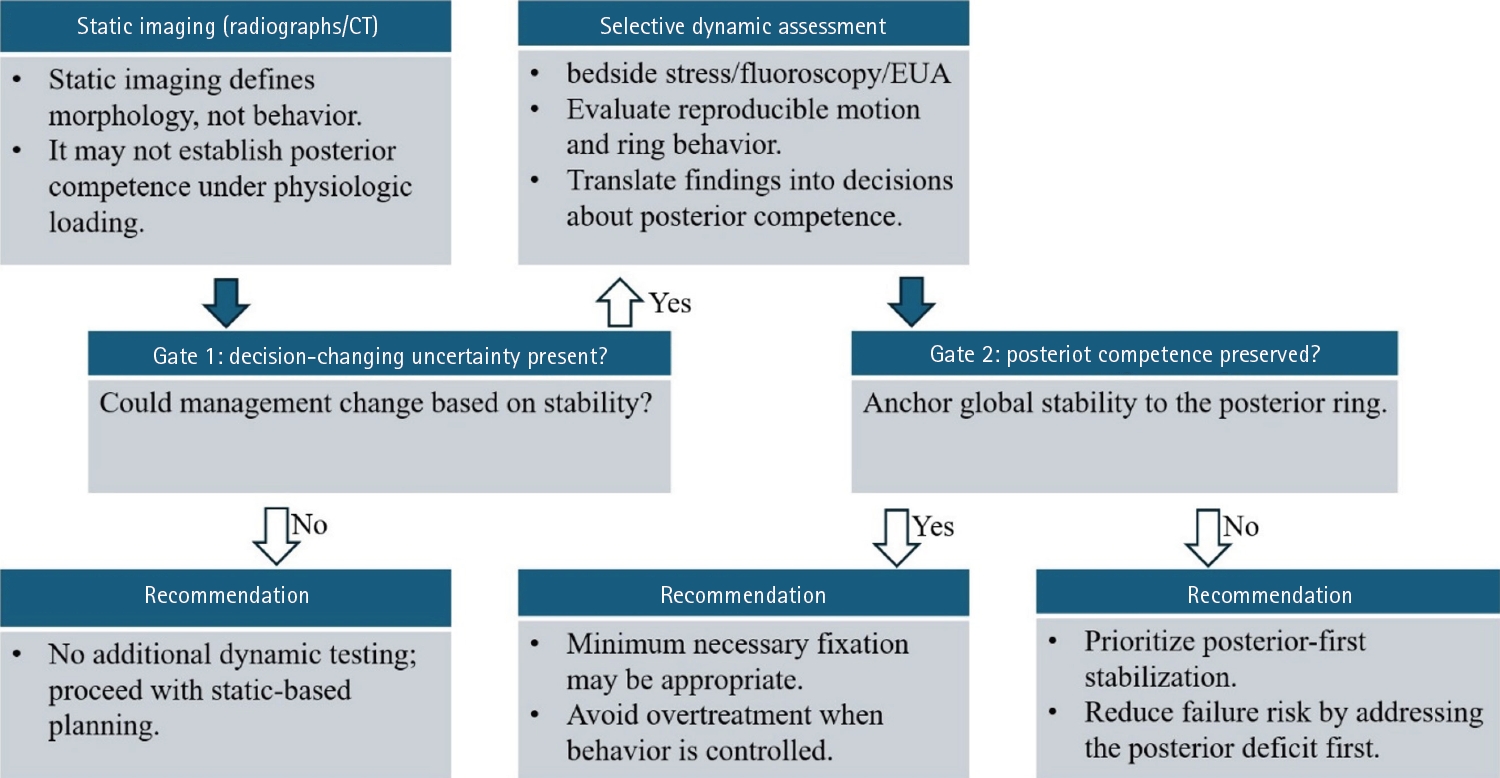
Gate-based decision framework linking static morphology to selective dynamic assessment. Static imaging using radiographs and computed tomography (CT) defines morphology and informs feasibility and operative planning, but may not reliably establish load-dependent behavior or posterior competence in borderline pelvic ring injuries. In this framework, Gates represent decision checkpoints that determine whether dynamic assessment is required and whether posterior competence should anchor management. When decision-changing uncertainty is present (Gate 1), selective dynamic assessment, such as bedside stress examination, fluoroscopy, or examination under anesthesia, documents reproducible motion and ring behavior. Posterior competence is treated as the primary anchor of global pelvic stability (Gate 2), guiding recommendations that range from static-based planning to minimum necessary fixation or posterior-first stabilization. Construct selection along the fixation continuum is summarized in Fig. 2. EUA, examination under anesthesia.
Fig. 2.
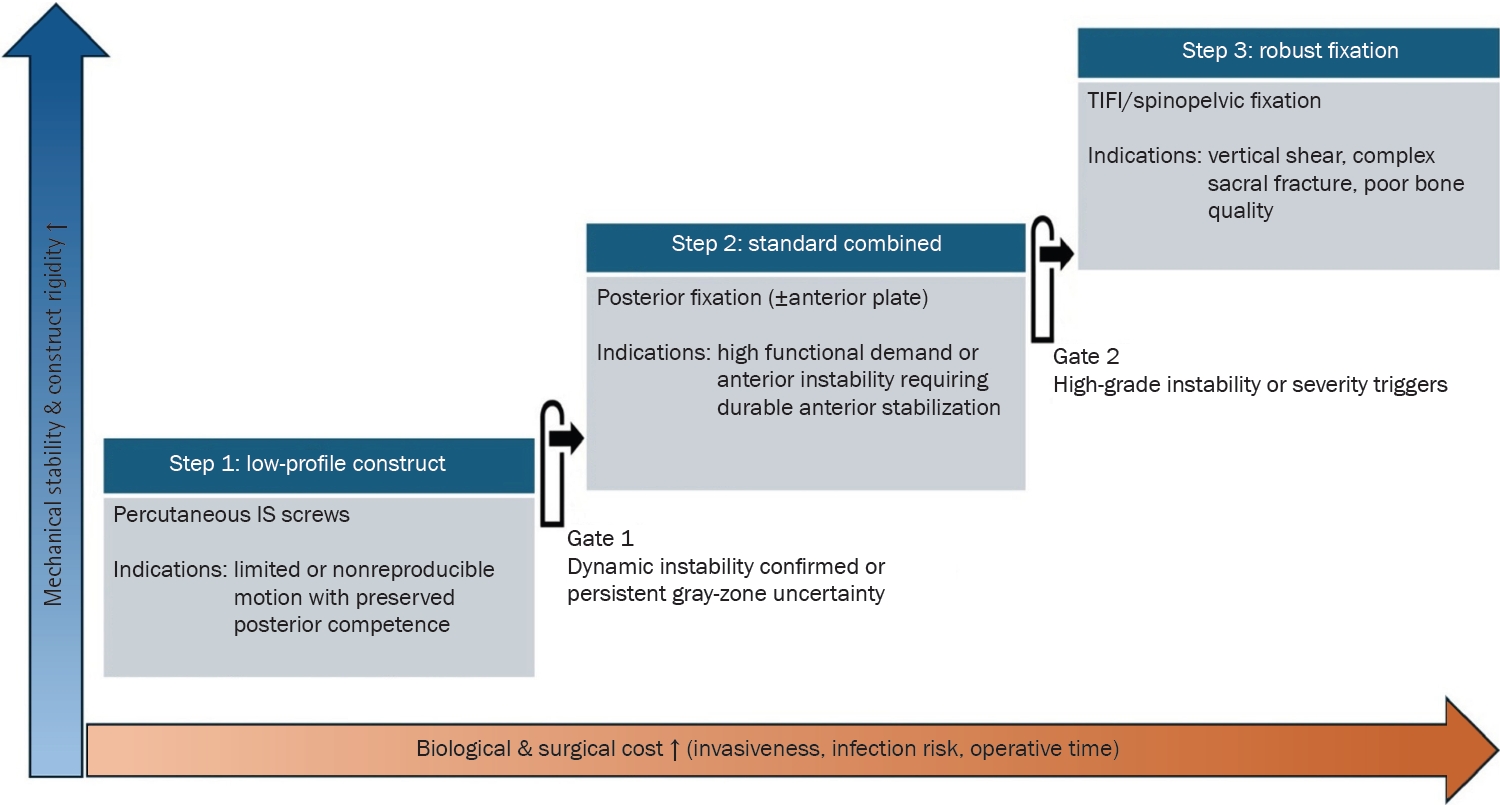
Fixation escalation along a construct continuum balancing mechanical stability and surgical cost. Fixation constructs are organized from low-profile to more robust strategies, balancing increasing mechanical stability and rigidity against escalating biological and surgical cost, including invasiveness, infection risk, and operative time. Steps represent levels of construct escalation along the fixation continuum. Step 1 reflects low-profile posterior fixation for limited or nonreproducible motion with preserved posterior competence. Step 2 represents standard combined fixation, consisting of posterior fixation with or without an anterior plate, when dynamic instability is confirmed or when persistent gray-zone uncertainty and clinical context favor added stability. Step 3 depicts escalation to robust constructs, such as transiliac internal fixation (TIFI) or spinopelvic fixation, for high-grade instability or severity triggers including vertical shear, complex sacral fracture, or severe osteoporosis. IS, iliosacral.
Table 1.
Working definitions and decision-linked terminology used in the current review
| Term | Working definition (current review) | Clinical/surgical implications | Key references |
|---|---|---|---|
| Dynamic instability | Clinically meaningful, demonstrable motion/displacement under stress or early physiologic loading, regardless of initial static alignment. | Shifts decision-making from static diastasis to load-dependent behavior in borderline patterns. | [1,2] |
| Radiographic change | Interval widening or minor alignment change after treatment without parallel symptom or functional deterioration. | Discourages reactive escalation driven by imaging alone, particularly for anterior constructs. | [6,7] |
| Clinical failure | Patient-centered deterioration with progressive malalignment that compromises the posterior ring reference frame, persistent disabling symptoms, and/or unplanned revision. | Defines reoperation thresholds by mechanical/functional deterioration rather than radiographic change alone. | [6-8] |
| Gray-zone injury | Presentations in which static imaging is insufficient to classify stability with confidence and management could reasonably differ. | Identifies cases where selective dynamic assessment or structured surveillance is most defensible. | [2,9] |
| Posterior competence | Functional integrity of the posterior ring (posterior sacroiliac complex/ligamentous integrity) as the primary determinant of global load transfer. | Supports posterior stabilization when posterior competence is compromised or cannot be established confidently. | [1,2] |
| Posterior ring reference frame | Interpreting anterior findings and postoperative change through the context of posterior alignment and stability. | Avoids overbuilding the anterior ring to compensate for posterior deficits and reduces radiograph-driven overreaction. | [1,2] |
| Cost of selection | Incremental burden of escalation (operative time, invasiveness, soft-tissue risk, complications, morbidity). | Requires explicit mechanical justification for construct expansion and reinforces “minimum necessary fixation.” | [3,10,11] |
| Minimum necessary fixation | The least extensive construct that reliably controls demonstrated instability and supports safe mobilization. | Anchors escalation: stabilize what is unstable; escalate only when standard constructs are unlikely to suffice. | [1,3] |
Terms are defined to link language to management decisions. Dynamic instability and postoperative anterior findings are interpreted within the posterior ring reference frame, with radiographic change distinguished from clinical failure to avoid imaging-driven escalation. Posterior competence denotes functional integrity of the posterior sacroiliac complex; cost of selection supports the minimum necessary fixation.
CT, computed tomography.
Table 2.
Fixation levels along a continuum: representative constructs, decision triggers, and the primary “cost of selection”
| Fixation level (continuum) | Typical construct examples | Decision triggers (indications) | Primary “cost of selection” | Key references |
|---|---|---|---|---|
| Structured surveillance | Standardized serial radiographs (AP/inlet/outlet) during early mobilization. | When gray-zone presentations show a stable early course, no evidence of clinically relevant motion, and no progressive malalignment. | Risk of delayed displacement; requires disciplined follow-up and a predefined conversion threshold. | [2,9] |
| Isolated anterior fixation | Symphyseal plating; anterior ramus screw fixation. | When posterior competence is confidently preserved and the anterior injury is the primary driver of symptoms or mobilization limits. | Risk of undertreating occult loss of posterior competence; anterior radiographic change may be overinterpreted as clinical failure. | [1,6,7] |
| Standard posterior fixation | 1–2 Iliosacral screws. | When loss of posterior competence is demonstrated or strongly suspected and is expected to compromise reduction maintenance or safe mobilization. | Technical demand and neurovascular risk; loosening risk in poor bone quality or suboptimal reduction. | [15,16,18] |
| Augmented posterior fixation | Additional SI screws and/or transiliac–transsacral screw options. | When posterior control is borderline and added stability is required to prevent recurrent motion and anterior construct overload. | Increased radiation and operative time; diminishing mechanical returns in high-grade vertical patterns. | [12,15,17] |
| Robust posterior fixation | Transiliac internal fixation. | When there is marked vertical tendency, substantial sacral comminution, compromised corridors, or inability to maintain alignment with screws alone. | Greater soft-tissue burden and implant prominence–related symptoms; higher likelihood of implant-related discomfort. | [10,12] |
| Highest-stability constructs | Lumbopelvic/spinopelvic stabilization. | When spinopelvic dissociation or high-grade vertical shear is present and length and shear control are paramount. | Highest morbidity profile; significant wound complication/infection risk; requires explicit mechanical justification. | [10,11] |
| Anterior adjunct (cross-cutting add-on) | Symphyseal plating; ramus screws (added after posterior stabilization). | When a posterior ring reference frame is secured, add selectively if residual anterior instability limits ring closure or mobilization. | Overreaction to expected anterior radiographic change can drive unnecessary revision; interpret anterior changes within the posterior ring reference frame and reserve revision for clinical failure. | [6-8] |
Indications are expressed as decision triggers rather than static cutoffs and should be interpreted within the posterior ring reference frame. “Isolated anterior fixation” presumes posterior competence; “anterior adjunct” is added selectively after posterior stabilization when residual anterior instability is clinically relevant.
AP, anteroposterior; SI, sacroiliac.
- 1. de Ridder VA, Whiting PS, Balogh ZJ, Mir HR, Schultz BJ. Pelvic ring injuries: recent advances in diagnosis and treatment. OTA Int 2023;6(3 Suppl):e261.ArticlePubMedPMC
- 2. Elsissy JG, Ruckle DE, LeBrun C, Johnson JP. Pelvic ring injuries: stable or not? J Am Acad Orthop Surg 2024;32:99-107.ArticlePubMed
- 3. Halawi MJ. Pelvic ring injuries: surgical management and long-term outcomes. J Clin Orthop Trauma 2016;7:1-6.ArticlePMC
- 4. Gansslen A, Lindahl J, Krappinger D, Lindtner RA, Staresinic M. The myth of 2.5 cm symphyseal diastasis. Arch Orthop Trauma Surg 2025;145:306.ArticlePubMedPMC
- 5. Sawauchi K, Esposito L, Kalbas Y, et al. Evolution of management strategies for unstable pelvic ring injuries over the past 40 years: a systematic review. Patient Saf Surg 2024;18:38.ArticlePubMedPMCPDF
- 6. Collinge C, Archdeacon MT, Dulaney-Cripe E, Moed BR. Radiographic changes of implant failure after plating for pubic symphysis diastasis: an underappreciated reality? Clin Orthop Relat Res 2012;470:2148-53.ArticlePubMedPMC
- 7. Eastman JG, Krieg JC, Routt ML Jr. Early failure of symphysis pubis plating. Injury 2016;47:1707-12.ArticlePubMed
- 8. Wheatley BM, Schorr R, Fuhrman H, et al. Can preoperative radiographs predict hardware complication or fracture displacement after operative treatment of pelvic ring injuries? Injury 2021;52:1788-92.ArticlePubMed
- 9. Keltz E, Keren Y, Jain A, et al. Surgical stabilisation in equivocal pelvic ring injuries: into the grey zone. Injury 2023;54:110887.ArticlePubMed
- 10. Patel S, Ghosh A, Jindal K, Kumar V, Aggarwal S, Kumar P. Spinopelvic fixation for vertically unstable AO type C pelvic fractures and sacral fractures with spinopelvic dissociation: a systematic review and pooled analysis involving 479 patients. J Orthop 2022;29:75-85.ArticlePubMedPMC
- 11. Godolias P, Plumer J, Cibura C, Dudda M, Schildhauer TA, Chapman JR. Posterior pelvic ring injuries, lumbosacral junction instabilities and stabilization techniques for spinopelvic dissociation: a narrative review. Arch Orthop Trauma Surg 2024;144:1627-35.ArticlePubMedPDF
- 12. Verbeek DO, Routt ML Jr. High-energy pelvic ring disruptions with complete posterior instability: contemporary reduction and fixation strategies. J Bone Joint Surg Am 2018;100:1704-12.ArticlePubMed
- 13. Wright RD Jr. Indications for open reduction internal fixation of anterior pelvic ring disruptions. J Orthop Trauma 2018;32 Suppl 6:S18-23.ArticlePubMed
- 14. Avilucea FR, Archdeacon MT, Collinge CA, Sciadini M, Sagi HC, Mir HR. Fixation strategy using sequential intraoperative examination under anesthesia for unstable lateral compression pelvic ring injuries reliably predicts union with minimal displacement. J Bone Joint Surg Am 2018;100:1503-8.ArticlePubMed
- 15. Hofmann A, Wagner D, Rommens PM. Iliosacral screw osteosynthesis: state of the art. Arch Orthop Trauma Surg 2025;145:122.ArticlePubMedPDF
- 16. Zhou W, Chen J, Pei X, et al. Incidence of and risk factors for screw loosening after iliosacral screw fixation for posterior pelvic ring injury. Orthop Surg 2023;15:1814-22.ArticlePubMedPMC
- 17. Muller F, Fuchtmeier B. A systematic review of the transiliac internal fixator (TIFI) for posterior pelvic injuries. SICOT J 2021;7:40.ArticlePubMedPMC
- 18. Pishnamaz M, Dienstknecht T, Hoppe B, et al. Assessment of pelvic injuries treated with ilio-sacral screws: injury severity and accuracy of screw positioning. Int Orthop 2016;40:1495-501.ArticlePubMedPDF
- 19. Avilucea FR, Whiting PS, Mir H. Posterior fixation of APC-2 pelvic ring injuries decreases rates of anterior plate failure and malunion. J Bone Joint Surg Am 2016;98:944-51.ArticlePubMed
- 20. Alzobi OZ, Alborno Y, Toubasi A, et al. Complications of conventional percutaneous sacroiliac screw fixation of traumatic pelvic ring injuries: a systematic review and meta-analysis. Eur J Orthop Surg Traumatol 2023;33:3107-17.ArticlePubMedPDF
- 21. Grewal IS, Starr AJ. What's new in percutaneous pelvis fracture surgery. Orthop Clin North Am 2020;51:317-24.ArticlePubMed
- 22. Shen L, Xue X, Ping Y, et al. Evolution of the reduction technique for unstable pelvic ring fractures: a narrative review. Eur J Med Res 2025;30:335.ArticlePubMedPMCPDF
- 23. Jordan MC, Fuchs KF, Herath SC, Windolf J, Meffert RH, Neubert A. Do we need another screw? Sacroiliac screw fixation in open-book pelvic ring injuries (APC type II). EFORT Open Rev 2024;9:827-36.ArticlePubMedPMC
References
Figure & Data
REFERENCES
Citations
Citations to this article as recorded by 
 ePub Link
ePub Link Cite
CiteDefinitive fixation for traumatic pelvic ring injuries: a dynamically informed, posterior-referenced framework
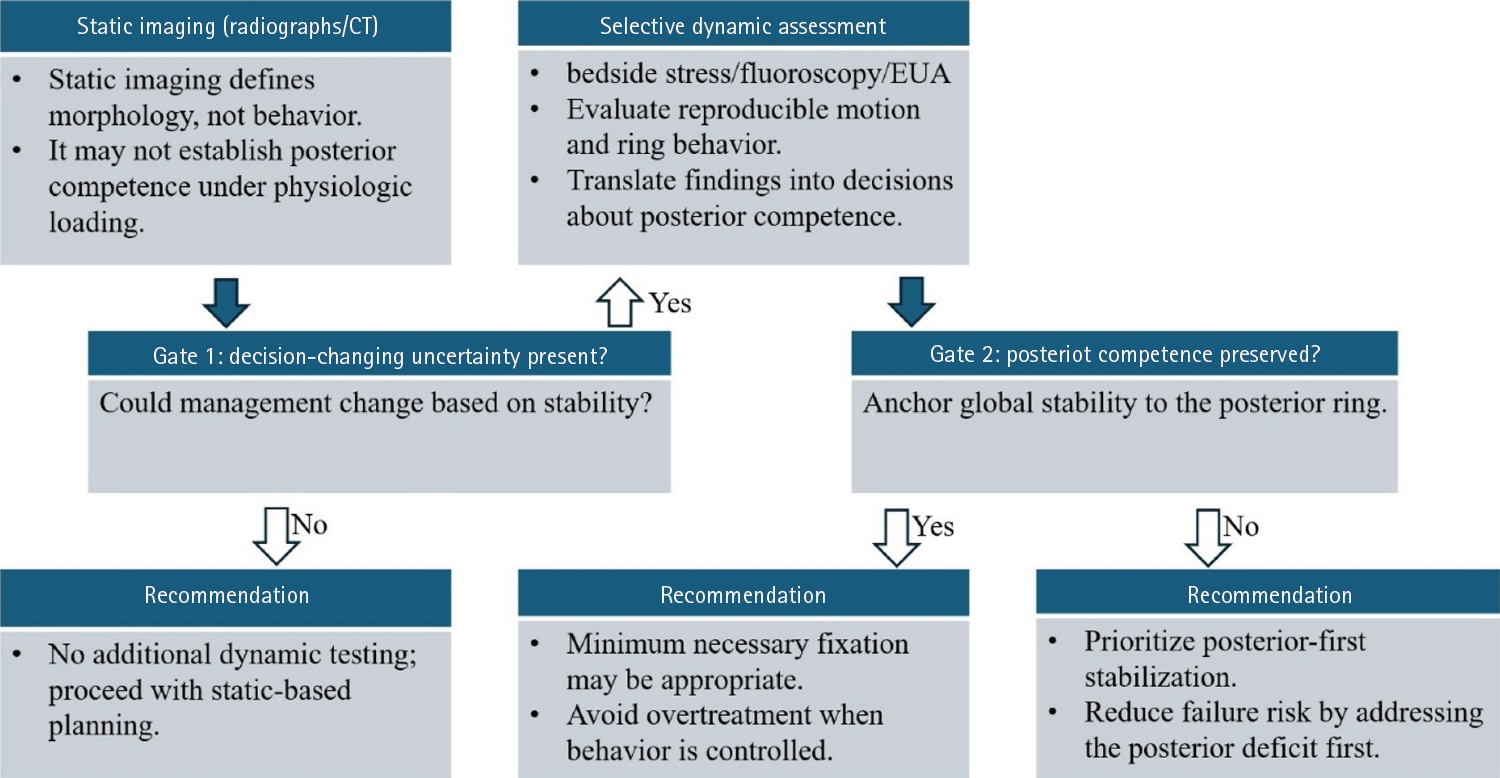
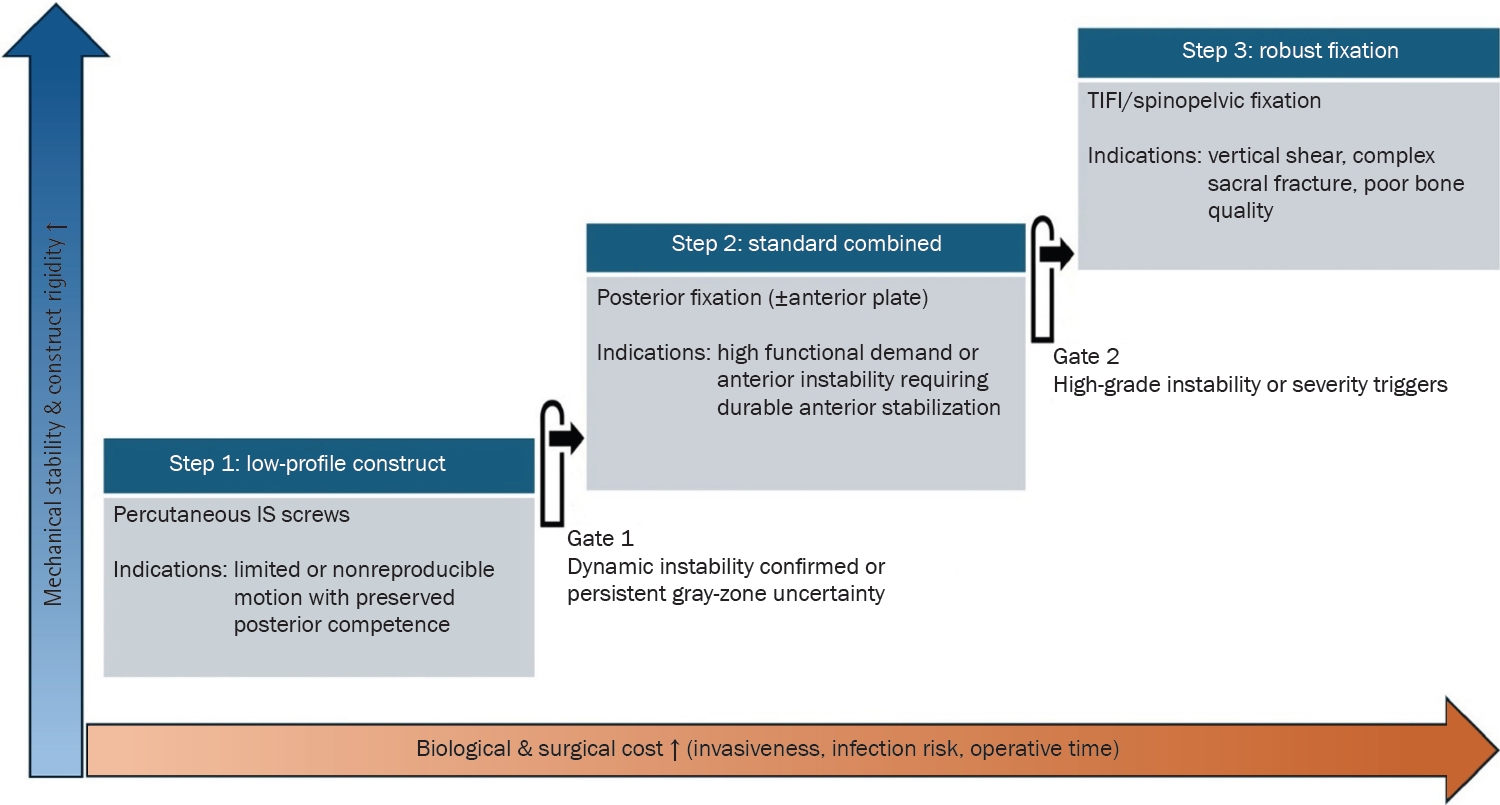
Fig. 1. Gate-based decision framework linking static morphology to selective dynamic assessment. Static imaging using radiographs and computed tomography (CT) defines morphology and informs feasibility and operative planning, but may not reliably establish load-dependent behavior or posterior competence in borderline pelvic ring injuries. In this framework, Gates represent decision checkpoints that determine whether dynamic assessment is required and whether posterior competence should anchor management. When decision-changing uncertainty is present (Gate 1), selective dynamic assessment, such as bedside stress examination, fluoroscopy, or examination under anesthesia, documents reproducible motion and ring behavior. Posterior competence is treated as the primary anchor of global pelvic stability (Gate 2), guiding recommendations that range from static-based planning to minimum necessary fixation or posterior-first stabilization. Construct selection along the fixation continuum is summarized in Fig. 2. EUA, examination under anesthesia.
Fig. 2. Fixation escalation along a construct continuum balancing mechanical stability and surgical cost. Fixation constructs are organized from low-profile to more robust strategies, balancing increasing mechanical stability and rigidity against escalating biological and surgical cost, including invasiveness, infection risk, and operative time. Steps represent levels of construct escalation along the fixation continuum. Step 1 reflects low-profile posterior fixation for limited or nonreproducible motion with preserved posterior competence. Step 2 represents standard combined fixation, consisting of posterior fixation with or without an anterior plate, when dynamic instability is confirmed or when persistent gray-zone uncertainty and clinical context favor added stability. Step 3 depicts escalation to robust constructs, such as transiliac internal fixation (TIFI) or spinopelvic fixation, for high-grade instability or severity triggers including vertical shear, complex sacral fracture, or severe osteoporosis. IS, iliosacral.
Fig. 1.
Fig. 2.
Definitive fixation for traumatic pelvic ring injuries: a dynamically informed, posterior-referenced framework
| Term | Working definition (current review) | Clinical/surgical implications | Key references |
|---|---|---|---|
| Dynamic instability | Clinically meaningful, demonstrable motion/displacement under stress or early physiologic loading, regardless of initial static alignment. | Shifts decision-making from static diastasis to load-dependent behavior in borderline patterns. | [1,2] |
| Radiographic change | Interval widening or minor alignment change after treatment without parallel symptom or functional deterioration. | Discourages reactive escalation driven by imaging alone, particularly for anterior constructs. | [6,7] |
| Clinical failure | Patient-centered deterioration with progressive malalignment that compromises the posterior ring reference frame, persistent disabling symptoms, and/or unplanned revision. | Defines reoperation thresholds by mechanical/functional deterioration rather than radiographic change alone. | [6-8] |
| Gray-zone injury | Presentations in which static imaging is insufficient to classify stability with confidence and management could reasonably differ. | Identifies cases where selective dynamic assessment or structured surveillance is most defensible. | [2,9] |
| Posterior competence | Functional integrity of the posterior ring (posterior sacroiliac complex/ligamentous integrity) as the primary determinant of global load transfer. | Supports posterior stabilization when posterior competence is compromised or cannot be established confidently. | [1,2] |
| Posterior ring reference frame | Interpreting anterior findings and postoperative change through the context of posterior alignment and stability. | Avoids overbuilding the anterior ring to compensate for posterior deficits and reduces radiograph-driven overreaction. | [1,2] |
| Cost of selection | Incremental burden of escalation (operative time, invasiveness, soft-tissue risk, complications, morbidity). | Requires explicit mechanical justification for construct expansion and reinforces “minimum necessary fixation.” | [3,10,11] |
| Minimum necessary fixation | The least extensive construct that reliably controls demonstrated instability and supports safe mobilization. | Anchors escalation: stabilize what is unstable; escalate only when standard constructs are unlikely to suffice. | [1,3] |
| Fixation level (continuum) | Typical construct examples | Decision triggers (indications) | Primary “cost of selection” | Key references |
|---|---|---|---|---|
| Structured surveillance | Standardized serial radiographs (AP/inlet/outlet) during early mobilization. | When gray-zone presentations show a stable early course, no evidence of clinically relevant motion, and no progressive malalignment. | Risk of delayed displacement; requires disciplined follow-up and a predefined conversion threshold. | [2,9] |
| Isolated anterior fixation | Symphyseal plating; anterior ramus screw fixation. | When posterior competence is confidently preserved and the anterior injury is the primary driver of symptoms or mobilization limits. | Risk of undertreating occult loss of posterior competence; anterior radiographic change may be overinterpreted as clinical failure. | [1,6,7] |
| Standard posterior fixation | 1–2 Iliosacral screws. | When loss of posterior competence is demonstrated or strongly suspected and is expected to compromise reduction maintenance or safe mobilization. | Technical demand and neurovascular risk; loosening risk in poor bone quality or suboptimal reduction. | [15,16,18] |
| Augmented posterior fixation | Additional SI screws and/or transiliac–transsacral screw options. | When posterior control is borderline and added stability is required to prevent recurrent motion and anterior construct overload. | Increased radiation and operative time; diminishing mechanical returns in high-grade vertical patterns. | [12,15,17] |
| Robust posterior fixation | Transiliac internal fixation. | When there is marked vertical tendency, substantial sacral comminution, compromised corridors, or inability to maintain alignment with screws alone. | Greater soft-tissue burden and implant prominence–related symptoms; higher likelihood of implant-related discomfort. | [10,12] |
| Highest-stability constructs | Lumbopelvic/spinopelvic stabilization. | When spinopelvic dissociation or high-grade vertical shear is present and length and shear control are paramount. | Highest morbidity profile; significant wound complication/infection risk; requires explicit mechanical justification. | [10,11] |
| Anterior adjunct (cross-cutting add-on) | Symphyseal plating; ramus screws (added after posterior stabilization). | When a posterior ring reference frame is secured, add selectively if residual anterior instability limits ring closure or mobilization. | Overreaction to expected anterior radiographic change can drive unnecessary revision; interpret anterior changes within the posterior ring reference frame and reserve revision for clinical failure. | [6-8] |
Table 1. Working definitions and decision-linked terminology used in the current review
Terms are defined to link language to management decisions. Dynamic instability and postoperative anterior findings are interpreted within the posterior ring reference frame, with radiographic change distinguished from clinical failure to avoid imaging-driven escalation. Posterior competence denotes functional integrity of the posterior sacroiliac complex; cost of selection supports the minimum necessary fixation. CT, computed tomography.
Table 2. Fixation levels along a continuum: representative constructs, decision triggers, and the primary “cost of selection”
Indications are expressed as decision triggers rather than static cutoffs and should be interpreted within the posterior ring reference frame. “Isolated anterior fixation” presumes posterior competence; “anterior adjunct” is added selectively after posterior stabilization when residual anterior instability is clinically relevant. AP, anteroposterior; SI, sacroiliac.

