 E-submission
E-submission TOTA
TOTA TOTS
TOTS
Articles
- Page Path
- HOME > J Musculoskelet Trauma > Volume 39(2); 2026 > Article
-
Original Article
- Biomechanical analysis of medial distal tibial locking plate fixation for distal-third spiral tibial shaft fractures
-
Yao-Jen Liu

-
Journal of Musculoskeletal Trauma 2026;39(2):140-146.
DOI: https://doi.org/10.12671/jmt.2026.00094
Published online: April 10, 2026
Department of Orthopedic Surgery, Hsinchu MacKay Memorial Hospital, Hsinchu, Taiwan
- Correspondence to: Yao-Jen Liu Department of Orthopedic Surgery, Hsinchu MacKay Memorial Hospital, No. 690, Sec. 2, Guangfu Rd., East Dist., Hsinchu City 300, Taiwan Tel: +886-3-6889595 Email: lyjs93311132@gmail.com
• Received: February 4, 2026 • Revised: February 24, 2026 • Accepted: March 9, 2026
© 2026 The Korean Orthopaedic Trauma Association
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/4.0/) which permits unrestricted noncommercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
- 226 Views
- 13 Download
Abstract
-
Background Distal spiral fractures of the tibial shaft present fixation challenges, particularly in patients who are not suitable candidates for intramedullary nailing. This study evaluated the biomechanical stability of medial minimally invasive percutaneous plating osteosynthesis (MIPO) under various physiological loading conditions.
-
Methods A finite-element model of a distal AO/OTA 42-A1.1c spiral fracture of the tibia was created using computed tomography data. A precontoured titanium medial distal tibia locking compression plate with nine locking screws was simulated. Material properties were assigned to cortical and cancellous bone. The loading conditions included axial compression (750 N), varus/valgus bending (300 N at a 9° offset), and internal/external torsion (7.5 N·m). von Mises stress and fracture displacement were analyzed.
-
Results Axial loading produced a peak plate stress of 508.06 MPa and a displacement of 2.17 mm. Valgus and varus loading generated stresses of 490.17 MPa and 324.08 MPa, respectively, with corresponding displacements of 3.86 mm and 2.01 mm. External and internal torsion resulted in stresses of 354.23 MPa and 358.9 MPa, respectively, with corresponding displacements of 2.64 mm and 2.22 mm.
-
Conclusions Medial distal tibial plating demonstrated favorable biomechanical performance in this finite-element model; however, clinical extrapolation should be made cautiously.
-
Level of evidence V.
Introduction
Tibial shaft fractures represent the most common long bone fractures. According to the AO/OTA classification system, spiral fractures (AO/OTA 42-A1) represent approximately 34% of tibial shaft fractures, followed by oblique fractures (AO/OTA 42-A2), which account for 17% [1]. Externally rotated spiral fractures are the most frequently observed and are often accompanied by a concurrent fibular fracture. These injuries can occur as a result of high-energy trauma—such as traffic accidents or falls in young males, or due to low-energy mechanisms like ground-level falls in the elderly individuals [1,2].
Especially in geriatric patients, bone quality and overall physical condition are often compromised, making early mobilization and weight bearing essential to prevent complications related to immobilization [3]. Therefore, it is crucial to choose a fixation technique that provides sufficient stability and can support early weight bearing.
While intramedullary (IM) nailing remains the gold standard treatment for tibial shaft fractures, it may not be suitable in certain patients due to soft tissue conditions, associated injuries, or the aging population with prior total knee arthroplasty or technical limitations [4], In such cases, techniques such as blocking screws, locking screws, or percutaneous reduction may be unfeasible, and there may also be an increased risk of pulmonary complications [5-7]. Recently, minimally invasive percutaneous plating osteosynthesis (MIPO) has gained traction as a viable alternative, particularly in cases with compromised anterior and medial soft tissue coverage where open reduction and internal fixation may increase the risk of wound complications. In addition, MIPO can also be used in patients with combined multiple injuries in whom IM reaming is contraindicated because of the potential increased risk of pulmonary complications or in cases where blocking screws, locking screws, or percutaneous repositioning techniques are difficult to perform.
Kati et al. [6] have proposed MIPO as an effective method for managing spiral and spiral wedge tibial shaft fractures, hypothesizing that it provides improved alignment and torsional stability. Biomechanical studies further support the use of medial plating, showing superior stiffness in both axial and torsional loading and reduced fracture site displacement and rotation compared to lateral plating [8,9]. However, limited studies have specifically evaluated the biomechanical performance of the medial plates in the treatment of distal tibial spiral fractures. This study aimed to evaluate the biomechanical performance of the medial plate for the stability of distal tibial spiral fracture under different physiological loads.
Methods
This study is a biomechanical simulation using a finite-element model based on an anonymized dataset from the Visible Human Project [10]. As the study did not involve any live human participants or animal subjects, Institutional Review Board approval and informed consent were not required. All computational procedures were conducted in accordance with the ethical standards of the institutional and/or national research committee.
A three-dimensional (3D) lower-leg finite-element model that included the tibia of a normal adult was developed. The bony structures were generated using a computed tomography data set segmentation from the Visible Human Project [10]. The 3D tibia model was reconstructed via the cortical shell and cancellous core. Cortical and cancellous regions were segmented anatomically during reconstruction, with the cortical shell defined as the outer layer of the tibial shaft and the cancellous bone assigned to the IM core. A simple spiral fracture model (AO/OTA 42-A1.1c) was made at the distal-third of the tibia shaft (Fig. 1A). The distal fracture initiation point was located 50 mm proximally to the distal tibial joint line, with a spiral fracture orientation of 50°. The fracture line extended approximately 40 mm in length from distal to proximal.
A common implant, a Zimmer periarticular distal tibial locking plate, was utilized in this simulation. This medial distal tibial plate features an anatomical precontoured titanium plate and is used with 10 holes and is 168 mm in length. The plate was affixed to the tibial shaft with three 3.5 mm locking screws whereas six 3.5 mm locking screws were used for the articular fixation. The plate and screw models were simplified without threads. The placement of the medial tibial plate on the simulated spiral fracture is shown in Fig. 1B.
The ANSYS Workbench 19 (ANSYS Inc.) was used for computational analysis. A frictional contact behavior was defined between the fracture fragments with a coefficient of friction of 0.2 for possible contact after loading while a coefficient of friction of 0.42 was used at the interfaces between the bone and the plate [11]. Fully constrained treatments were applied between the screws and the surrounding bone, as well as between the contact surfaces of the plate and the screw head, to simulate the mechanism of tightened locking. Both plate and screws were made of titanium and modeled according to specifications described in previous studies (Young’s modulus, 110,000 MPa; Poisson ratio, 0.3), while the cortical bone was modeled with Young’s modulus of 17,500 MPa and 0.3 Poisson ratio. Material properties for the cancellous bone were assigned with a Young’s modulus of 1,500 MPa and Poisson ratios of 0.12. Bones and implants were modeled as linear elastic, isotropic, and homogeneous materials.
A vertical compressive load of 750 N was applied to simulate physiological weight bearing, corresponding to loading conditions ranging from cane-assisted walking to fast walking [12]. For varus-valgus bending tests, a load of 300 N was applied at the medial side of the distal tibial articular surface in a direction deviated 9° medially from the mechanical axis of the lower limb to simulate varus stress [13]. Conversely, a 300 N load was applied to the lateral side of the distal tibial articular surface at a 9° lateral deviation to simulate valgus stress. For torsional loading, the distal articular surface of the tibia was fixed, and internal and external torques of 7.5 N·m were applied to the proximal articular surface to simulate internal and external rotation forces, respectively [12]. Maximum von Mises stress in the bone plate and the maximum displacement of the fracture surface were calculated for evaluation.
Results
Under vertical loading (Fig. 2), the bone plate exhibited a maximum von Mises stress of 508.06 MPa, with a corresponding fracture site displacement of 2.17 mm. Valgus loading (Fig. 3) resulted in a relatively high von Mises stress of 490.17 MPa among the three loading modes and a displacement of 3.86 mm. In contrast, varus loading (Fig. 4) produced a lower von Mises stress of 324.08 MPa among three loading modes and lower displacement of 2.01 mm. Under external rotational loading (Fig. 5), the maximum stress was 354.23 MPa, with a fracture displacement of 2.64 mm. Internal rotational loading (Fig. 6) resulted in a peak von Mises stress of 358.9 MPa and lower fracture displacement observed than that observed under external rotation, at 2.22 mm.
Discussion
This study investigated the biomechanical performance of a medial distal tibial plate for the stabilization of distal-third spiral tibial shaft fractures under various physiological loading conditions. Biomechanically, the failure displacement of a fracture fragment is 3 mm [14]. The finite-element analysis (FEA) demonstrated that the medial plate provided sufficient stability under vertical compressive, varus, and internal/external rotation loadings, with relatively low fracture displacement (approximately 2 mm).
Vertical loading, which simulates normal weight bearing, produced the highest von Mises stress (508.06 MPa) in the plate, yet the corresponding fracture displacement was limited to 2.17 mm, indicating effective load transfer and structural stiffness. In Jia et al. [15]’s study, which used the finite-element method to evaluate a distal transverse fracture type under comparable loading conditions, the lateral plate sustained a peak stress of 738 MPa with 5.74 mm of displacement. These findings suggest the superiority of medial plating in resisting vertical compressive loading. Importantly, while the maximum stress remained below the commonly cited fatigue strength of titanium alloy (approximately 600 MPa), it approached this threshold. This is clinically significant, as repeated loading cycles—especially during activities such as walking or stair climbing—can lead to fatigue failure over time if the stress approaches or exceeds the fatigue endurance limit of the implant material. Therefore, although acute performance under single-cycle loading is acceptable, the proximity to fatigue limits warrants caution in high-demand patients or those with delayed healing (such as elderly patients).
Varus loading resulted in the lowest stress (324.08 MPa) and minimal displacement (2.01 mm), likely because the loading vector aligned with the medial plate’s position and construct geometry. In contrast, valgus loading, which applies a bending moment opposite to the plate’s location, produced higher stress (490.17 MPa) and increased displacement (3.86 mm), reflecting the plate’s biomechanical disadvantage under medially-directed bending forces. These findings are consistent with prior biomechanical studies showing superior stiffness in axial and varus directions for medial plates, but increased vulnerability under valgus loading [8,9]. The increased stress and displacement observed under valgus loading highlight a potential coronal-plane vulnerability of medial distal tibial plating, as the bending moment acts opposite to the plate location. Clinically, this warrants careful attention to construct optimization and alignment control. The use of a longer plate to increase working length, higher distal screw density, bicortical fixation when feasible, and multiplanar locking screw orientation may enhance resistance to valgus bending. Anatomical reduction in the coronal plane is essential, as residual valgus malalignment may further amplify tensile stress on the medial plate. Additionally, the present model did not include the fibula, which in vivo may provide lateral column support and reduce valgus instability; therefore, fibular fixation should be considered in distal-third fractures when coronal stability is a concern.
Under torsional conditions, both internal and external rotational loading resulted in moderate stress (354.23–358.9 MPa), but the highest displacement at the fracture site (2.22–2.64 mm), suggesting limited torsional control. In Jia et al. [15]’s study, lateral plating fixation demonstrated a peak stress of 355.04 MPa with a displacement of 1.39 mm. These findings suggest that medial plating may provide a safer construct than lateral plating under comparable loading conditions. This may be due to the geometric limitations of the plate and screw configuration in resisting rotational moments. While Kati et al. [6] advocated medial MIPO for spiral fractures, citing improved alignment and torsional resistance, our findings suggest that the construct alone may be insufficient to fully counteract torsional instability. In clinical practice, this may necessitate supplemental fixation techniques or altered screw configurations to optimize rotational stability, especially in active patients or complex fracture patterns.
The proximity of observed stress values to the fatigue strength of titanium emphasizes the need for careful patient selection and postoperative load management. Though none of the loading scenarios exceeded the fatigue threshold, repeated high-load activities or delayed union could potentially result in cyclic fatigue and implant failure. Therefore, long-term implant durability should be a consideration, particularly in younger or heavier patients and in those expected to return to high levels of activity.
Several biomechanical studies have evaluated fixation strategies for distal tibial fractures using both finite-element modeling and experimental testing.
Jia et al. [15] performed a finite-element comparison of medial plating, lateral plating, and IM nailing for distal tibial fractures under axial and torsional loading. Their results demonstrated differences in stress distribution and displacement between fixation methods, with medial plating showing favorable axial stiffness but variable torsional performance depending on screw configuration. However, differences in fracture pattern and model assumptions limit direct comparison with the present study.
Cao et al. [16] investigated the biomechanical effects of plate length, fibular integrity, and plate position in tibial shaft fracture models. Their findings emphasized that fibular fixation significantly enhances coronal-plane stability and reduces implant stress in distal fractures. They also reported that longer plates distribute stress more evenly and improve construct durability, underscoring the importance of construct configuration.
Unal et al. [17] performed biomechanical testing and FEA comparing a newly designed tibial IM nail with distal supportive locking versus medial distal tibial plating. Their results demonstrated that under axial loading, the IM nail construct showed greater force resistance, greater stiffness, and lower fracture displacement than the plate group, suggesting superior load transfer and structural stability of nail fixation under axial loads.
Collectively, previous biomechanical studies indicate that fixation performance in distal tibial fractures is strongly influenced by fracture pattern, implant position, plate length, screw configuration, and fibular integrity. The present findings are consistent with prior reports showing that medial plating provides satisfactory axial stability but may demonstrate increased stress under coronal-plane bending, particularly without fibular support. In comparison, IM nailing generally offers superior axial load-sharing and stiffness, whereas plating constructs may allow more precise alignment control in selected fracture configurations.
Several limitations must be acknowledged. The finite-element model utilized homogeneous, isotropic, and linear elastic assumptions for bone and implant materials, which may not fully represent in vivo mechanical behavior. Thread features of the screws were not modeled, and biological healing or callus formation over time was not considered. Only single plate length was evaluated, and it was not compared with IM nailing to further prove the ability of enabling early weight bearing. Only simple spiral fracture type was analyzed. The findings primarily apply to simple distal spiral fractures rather than highly comminuted patterns. This study references a titanium fatigue threshold of 600 MPa to explain the safety of medial plating for the fixation of the spiral tibial shaft fracture. However, the actual fatigue performance of a bone plate depends on multiple factors, including alloy type, surface condition, loading cycles, and stress ratios. Additionally, this study is based on FEA, which evaluates construct mechanics under controlled, idealized, and primarily static loading conditions. Although FEA provides valuable insight into stress distribution and interfragmentary motion, it cannot directly predict clinical outcomes such as fracture union, implant failure, complication rates, or patient function. Therefore, the present findings should be interpreted as biomechanical evidence rather than direct clinical recommendations. Furthermore, the loading conditions applied in this model do not fully replicate the complex in vivo biomechanical environment of the tibia. In reality, tibial loading is influenced by dynamic muscle forces, joint reactions, and patient-specific gait patterns, with relatively stronger lateral muscular forces that may amplify valgus-directed bending moments. In this context, the increased stress and displacement observed under valgus loading may represent a potential mechanical vulnerability of the medial plating construction, particularly during functional activities such as walking or stair climbing. Accordingly, the clinical implications of these findings should be interpreted with caution, and further in vivo or clinical studies are necessary to validate their translational relevance. The cited reference [15] used for comparison did not involve an equivalent fracture type to that investigated in the present study. As no methodologically comparable reference was available, this comparison was intended only to verify that the analyzed results of the current study fell within reasonable ranges. Nonetheless, the controlled and comparative nature of the simulated loading conditions provides valuable insight into the mechanical performance of the medial plating construct.
This finite-element study evaluated the mechanical behavior of a medial distal tibial plate construct in a normal adult tibial model with a distal-third spiral fracture in the absence of the fibula under idealized loading conditions. The results demonstrated that, within the constraints of the model, the medial plating construct maintained fracture displacement within the simulated parameters, and the calculated von Mises stresses remained below the referenced fatigue threshold of titanium alloy. Increased stress and displacement were observed under axial compression and valgus loading, indicating relative mechanical sensitivity to these loading modes. These findings describe only the biomechanical performance of the specific construct configuration analyzed and should not be interpreted as direct clinical recommendations or as evidence of surgical technique superiority.
-
Author contributions
All the work was done by Yao-Jen Liu.
-
Conflicts of interest
No potential conflict of interest relevant to this article was reported.
-
Funding
None.
-
Data availability
Not applicable.
-
Acknowledgments
None.
-
Supplementary materials
None.
Article Information
Fig. 1.

The reconstructed tibial model with (A) a simulated spiral fracture and (B) an implanted medial distal locking plate.
Fig. 2.
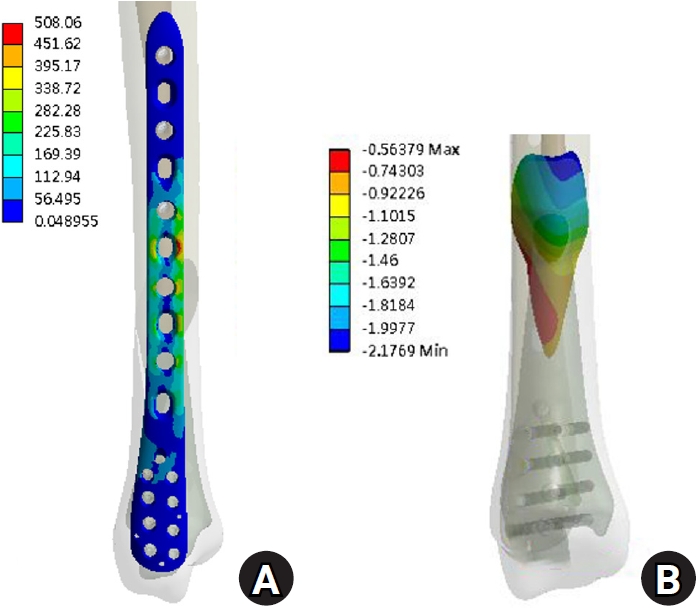
The results under compression load. (A) von Mises stress distribution on the plate and (B) the displacement on the fracture surface.
Fig. 3.
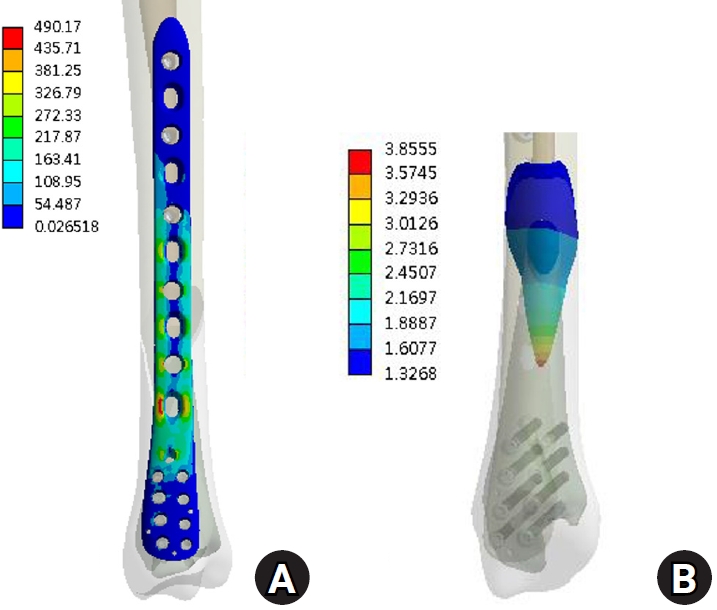
The results under valgus load. (A) von Mises stress distribution on the plate and (B) the displacement on the fracture surface.
Fig. 4.
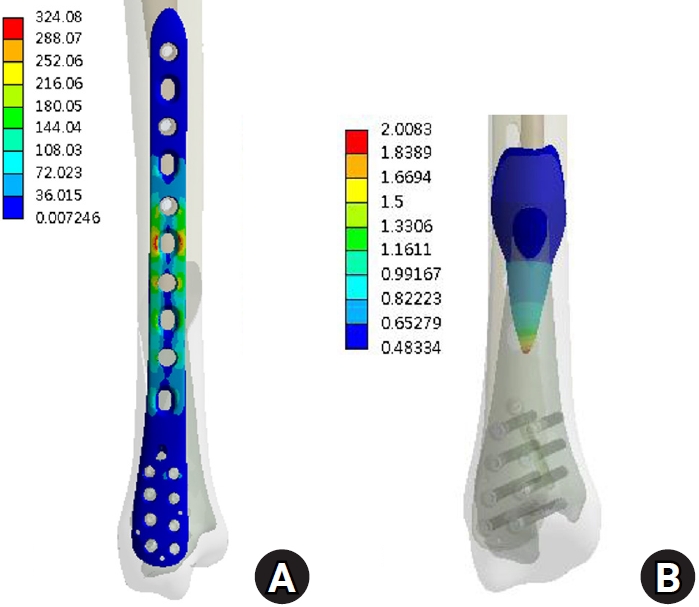
The results under varus load. (A) von Mises stress distribution on the plate and (B) the displacement on the fracture surface.
Fig. 5.
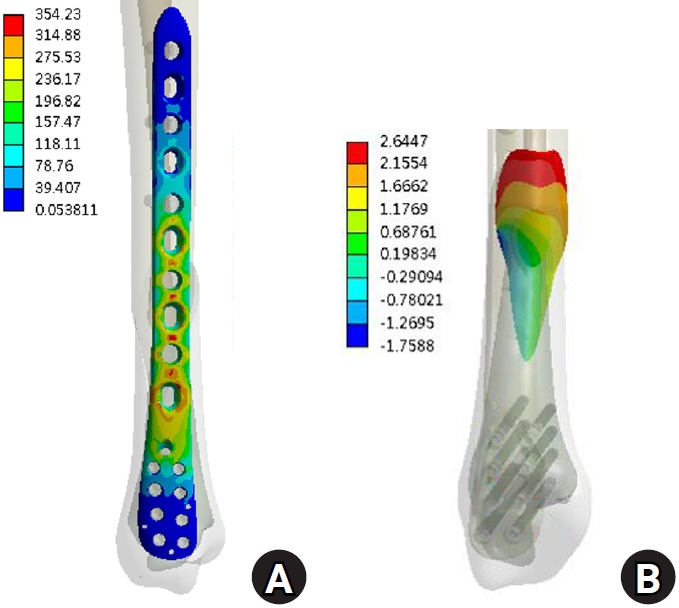
The results under external torque. (A) von Mises stress distribution on the plate and (B) the displacement on the fracture surface.
Fig. 6.
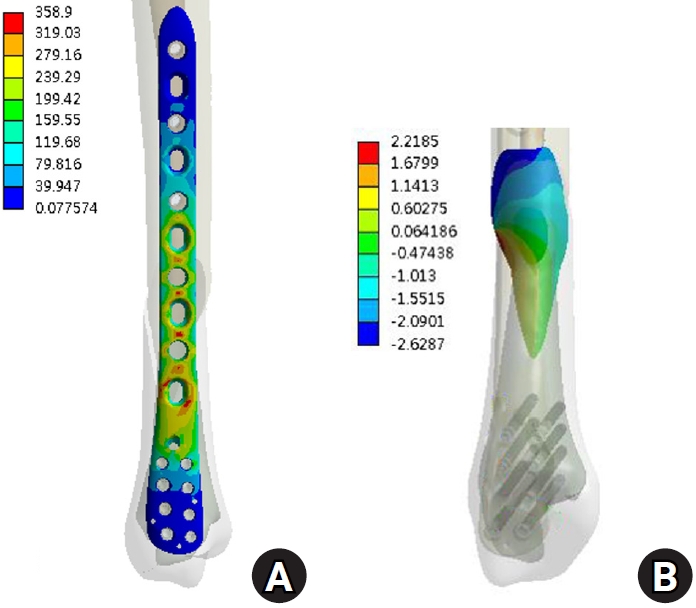
The results under internal torque. (A) von Mises stress distribution on the plate and (B) the displacement on the fracture surface.
- 1. Larsen P, Elsoe R, Hansen SH, Graven-Nielsen T, Laessoe U, Rasmussen S. Incidence and epidemiology of tibial shaft fractures. Injury 2015;46:746-50.ArticlePubMed
- 2. Laurila J, Huttunen TT, Kannus P, Kaariainen M, Mattila VM. Tibial shaft fractures in Finland between 1997 and 2014. Injury 2019;50:973-7.ArticlePubMed
- 3. Kammerlander C, Pfeufer D, Lisitano LA, Mehaffey S, Bocker W, Neuerburg C. Inability of older adult patients with hip fracture to maintain postoperative weight-bearing restrictions. J Bone Joint Surg Am 2018;100:936-41.ArticlePubMed
- 4. Tamburini L, Zeng F, Neumann D, et al. A review of tibial shaft fracture fixation methods. Trauma Care 2023;3:202-11.Article
- 5. Lai TC, Fleming JJ. Minimally invasive plate osteosynthesis for distal tibia fractures. Clin Podiatr Med Surg 2018;35:223-32.ArticlePubMed
- 6. Katı YA, Oken OF, Yıldırım AO, Kose O, Unal M. May minimally invasive plate osteosynthesis be an alternative to intramedullary nailing in selected spiral oblique and spiral wedge tibial shaft fractures. Jt Dis Relat Surg 2020;31:494-501.ArticlePubMedPMC
- 7. Xue XH, Yan SG, Cai XZ, Shi MM, Lin T. Intramedullary nailing versus plating for extra-articular distal tibial metaphyseal fracture: a systematic review and meta-analysis. Injury 2014;45:667-76.ArticlePubMed
- 8. Aizat RM, Kadir MR, Ab Rahman S, Md Shihabudin TM, Robson N, Kamarul T. Biomechanical comparative analyses between the anterolateral and medial distal tibia locking plates in treating complex distal tibial fracture: a finite element study. J Med Imaging Hlth Inform 2013;3:532-7.Article
- 9. Pirolo JM, Behn AW, Abrams GD, Bishop JA. Anterolateral versus medial plating of distal extra-articular tibia fractures: a biomechanical model. Orthopedics 2015;38:e760-5.ArticlePubMed
- 10. Oken OF, Yildirim AO, Asilturk M. Finite element analysis of the stability of AO/OTA 43-C1 type distal tibial fractures treated with distal tibia medial anatomic plate versus anterolateral anatomic plate. Acta Orthop Traumatol Turc 2017;51:404-8.ArticlePubMedPMC
- 11. Lin K, Tarng Y, Lin K, Wei H. Biomechanical superiority of locking plate designed with cluster of head screws compared to conventional buttress plate for fixation of posteromedial tibial plateau fractures: a computational assessment. J Med Biol Eng 2022;42:189-95.ArticlePDF
- 12. Ebramzadeh E, Knutsen AR, Sangiorgio SN, Brambila M, Harris TG. Biomechanical comparison of syndesmotic injury fixation methods using a cadaveric model. Foot Ankle Int 2013;34:1710-7.ArticlePubMedPDF
- 13. Jiang D, Zhan S, Wang Q, Ling M, Hu H, Jia W. Biomechanical comparison of locking plate and cancellous screw techniques in medial malleolar fractures: a finite element analysis. J Foot Ankle Surg 2019;58:1138-44.ArticlePubMed
- 14. Ali AM, El-Shafie M, Willett KM. Failure of fixation of tibial plateau fractures. J Orthop Trauma 2002;16:323-9.ArticlePubMed
- 15. Jia J, Tang C, Yue J, Li F. Finite element analysis of three different fixation methods for distal tibial fracture. Chin J Tissue Eng Res 2019;23:5188-94.Article
- 16. Cao Y, Zhang Y, Huang L, Huang X. The impact of plate length, fibula integrity and plate placement on tibial shaft fixation stability: a finite element study. J Orthop Surg Res 2019;14:52.ArticlePubMedPMCPDF
- 17. Unal OK, Dagtas MZ, Najafov T, Demir C, Ugutmen E, Akpinar F. Medial plating versus newly designed intramedullary nail with distal interlocking system for distal tibia fractures: a biomechanical study with finite element analysis. Jt Dis Relat Surg 2025;37:477-88.Article
References
Figure & Data
REFERENCES
Citations
Citations to this article as recorded by 
 ePub Link
ePub Link Cite
CiteBiomechanical analysis of medial distal tibial locking plate fixation for distal-third spiral tibial shaft fractures

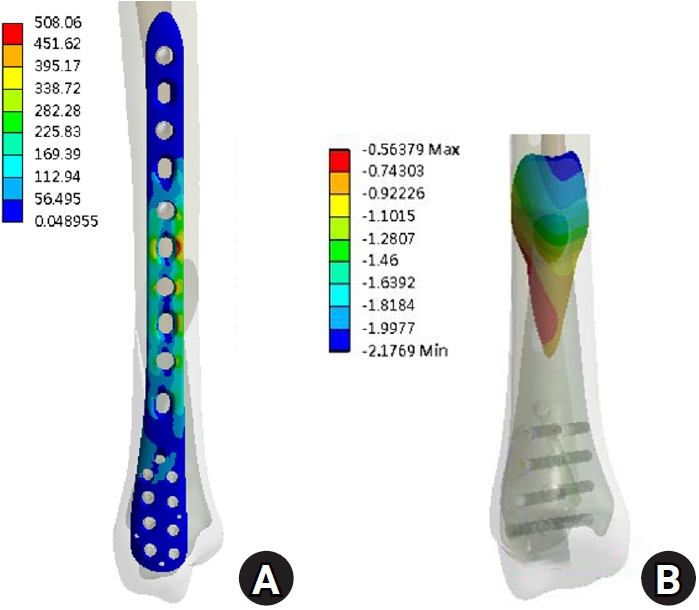
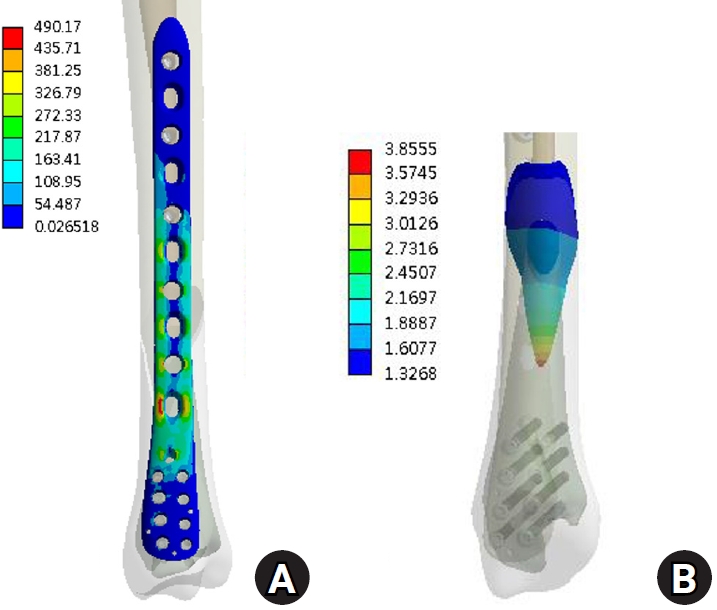
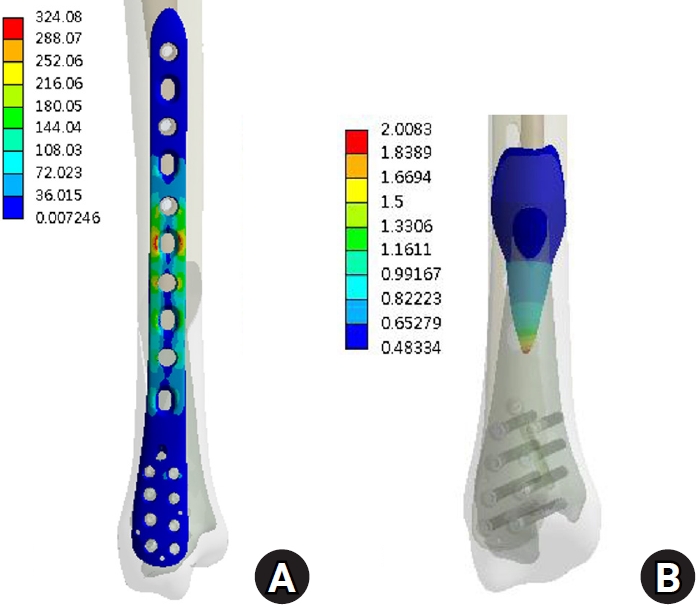
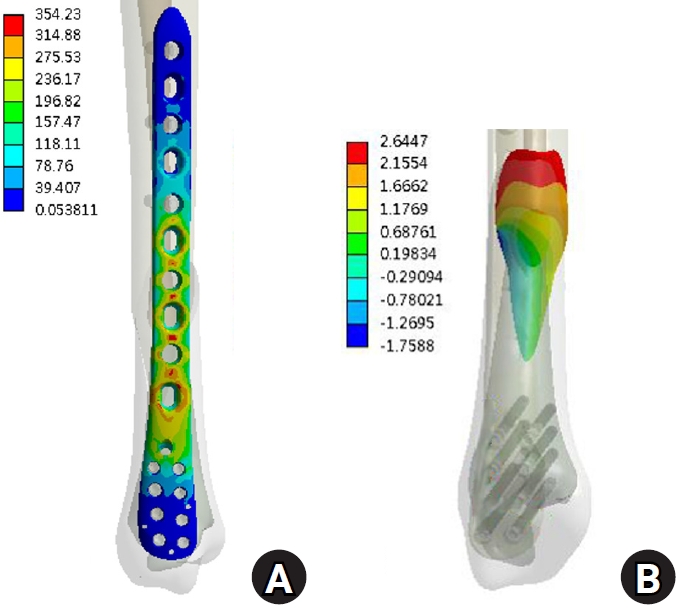
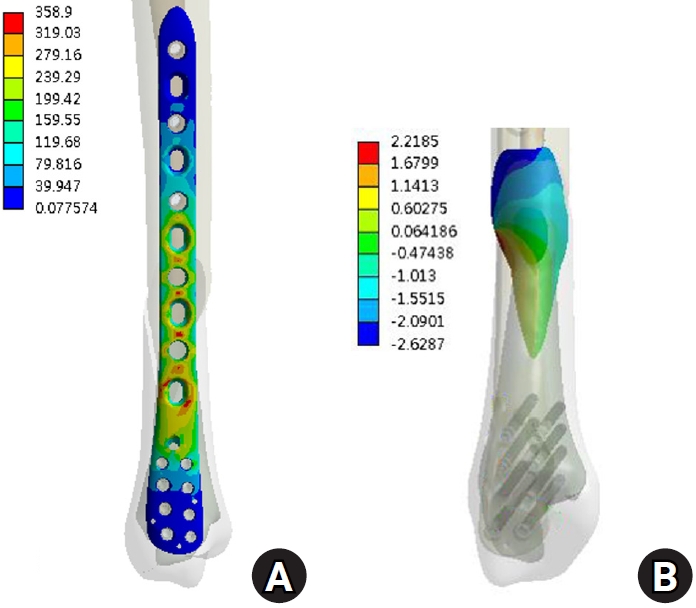
Fig. 1. The reconstructed tibial model with (A) a simulated spiral fracture and (B) an implanted medial distal locking plate.
Fig. 2. The results under compression load. (A) von Mises stress distribution on the plate and (B) the displacement on the fracture surface.
Fig. 3. The results under valgus load. (A) von Mises stress distribution on the plate and (B) the displacement on the fracture surface.
Fig. 4. The results under varus load. (A) von Mises stress distribution on the plate and (B) the displacement on the fracture surface.
Fig. 5. The results under external torque. (A) von Mises stress distribution on the plate and (B) the displacement on the fracture surface.
Fig. 6. The results under internal torque. (A) von Mises stress distribution on the plate and (B) the displacement on the fracture surface.
Fig. 1.
Fig. 2.
Fig. 3.
Fig. 4.
Fig. 5.
Fig. 6.
Biomechanical analysis of medial distal tibial locking plate fixation for distal-third spiral tibial shaft fractures

