 E-submission
E-submission TOTA
TOTA TOTS
TOTS
Articles
- Page Path
- HOME > J Musculoskelet Trauma > Volume 39(2); 2026 > Article
-
Case Report
- Paradoxical hypertrophy as a cause of femoral insufficiency fractures analyzed through differences in force application in Korea: three case reports
-
Yong-Uk Kwon
 , Dae-Hyun Park, Hyoung-Gu Kang
, Dae-Hyun Park, Hyoung-Gu Kang -
Journal of Musculoskeletal Trauma 2026;39(2):174-180.
DOI: https://doi.org/10.12671/jmt.2025.00388
Published online: April 23, 2026
Department of Orthopedic Surgery, Inje University Busan Paik Hospital, Inje University College of Medicine, Busan, Korea
- Correspondence to: Dae-Hyun Park Department of Orthopedic Surgery, Inje University Busan Paik Hospital, Inje University College of Medicine, 75 Bokji-ro, Busanjin-gu, Busan 47392, Korea Tel: +82-51-890-6129 Email: spineparkdaehyun@gmail.com
• Received: December 13, 2025 • Revised: January 29, 2026 • Accepted: February 9, 2026
© 2026 The Korean Orthopaedic Trauma Association
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/4.0/) which permits unrestricted noncommercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
- 355 Views
- 16 Download
Abstract
-
Previous studies have extensively examined the association between femoral insufficiency fractures and prolonged bisphosphonate therapy. However, alternative etiologies remain insufficiently characterized. This study aimed to analyze nonpharmacologic factors associated with femoral insufficiency fractures, with particular emphasis on paradoxical cortical hypertrophy and altered biomechanical load distribution. We reviewed three cases of femoral insufficiency fracture that were surgically treated at our institution between January 2018 and January 2022. None of the patients had a history of bisphosphonate use. Clinical histories—including underlying comorbidities, prior surgical procedures, and radiographic findings—were evaluated. Serial radiographs obtained before and after fracture occurrence were analyzed to characterize fracture morphology and associated cortical changes. Case 1 involved a patient with posttraumatic hip synostosis; case 2 involved a patient with osteogenesis imperfecta; and case 3 involved a patient who had previously undergone intramedullary nailing for an intertrochanteric fracture. Lateral femoral bowing and cortical hypertrophy preceded fracture development in two cases, whereas focal cortical hypertrophy at the distal locking screw site was observed in the third case. No history of bisphosphonate therapy was identified in any patient. Fractures developed at sites characterized by increased cortical remodeling and abnormal load concentration. Femoral insufficiency fractures can occur in the absence of bisphosphonate therapy. Paradoxical cortical hypertrophy and altered biomechanical force distribution appear to be important contributing factors.Level of evidence: IV.
Introduction
Insufficiency fractures are a subtype of stress fractures that occur when repeated and subthreshold stress is applied to normal or abnormal bones [1]. Stress fractures include both fatigue and insufficiency fractures, which are best understood as two contrasting processes with a similar end result. Fatigue fractures are caused by repeated and subthreshold loads upon normal bone, whereas insufficiency fractures are the result of repeated and subthreshold stress upon abnormal bone with deficient elastic resistance [2]. Although the term fatigue fracture may be occasionally used interchangeably with stress fracture, these fractures should be viewed as a subtype of stress fracture. Meanwhile, a pathologic fracture is a break in a weakened bone that is caused by an underlying disease (Benign or malignant neoplasm, infection, metabolic bone disease etc.) [3]. Therefore, insufficiency fractures that occur in abnormal bones are stress fractures and belong to pathologic fractures, and fatigue fractures that occur in normal bones are stress fractures and belong to physiologic fractures (Fig. 1).
Insufficiency fractures most commonly involve the weight-bearing bones, particularly the pelvis, spine, femur and other axial skeleton sites [4,5]. In this study, we present cases of femoral insufficiency fractures occurring in the proximal femur, with a focus on analyzing the specific causative factors and clinical features observed in our patient cases.
The incidence of femoral insufficiency fractures increases with age, and their incidence is especially high in the elderly [4]. Many efforts have been made to identify the causes of femoral insufficiency fractures, and the most widely acknowledged risk factor at present is the long-term use of bisphosphonates to prevent osteoporosis [5]. Many studies have been conducted on this topic, and various case reports have been published to date. But, the published literature suggests that femoral insufficiency fractures have a different pathology than the standard osteoporotic fractures, and the atypical features of these fractures are rarely seen without long-term bisphosphonate therapy [5]. Rogers et al. [6] reported that the potential absolute risk associated with bisphosphonate use seems to be relatively small. In some studies, evidence from clinical and regulatory sources points out that insufficiency fractures can occur independently of bisphosphonate therapy, highlighting the need to consider alternative mechanisms such as biomechanical factors and comorbidities [6-8].
While bisphosphonate use remains a significant contributing factor, this study introduces several cases of femoral insufficiency fractures occurring without bisphosphonate exposure, aiming to discuss other possible nonpharmacologic etiologies and mechanisms involved.
Case reports
This study was approved by Institutional Review Board (IRB) of Inje University Busan Paik Hospital (IRB No. 2023-05-044). The authors attest that informed consent was obtained from all individual patients or their legal guardians.
A 58-year-old female patient visited our emergency room, complaining of pain in the right hip that occurred the day before her hospital visit. She had a history of restricted right hip range of movement following a dislocation of the right hip in her youth, and she typically walked with a cane. The day prior to her visit, while lying on her right side and sleeping, she developed pain in the right hip area without any history of trauma. Upon examination, the patient had a background of hypertension and exhibited a bone mineral density (BMD) of ‒0.1 in the femoral neck. Notably, she had no history of malignancy. Initial physical examination and computed tomography scans conducted upon her arrival did not reveal any signs of malignancy or infection at the fracture site, indicating a low likelihood of these conditions as contributing factors. Radiographic evaluations, including both hip anteroposterior and right axial views, demonstrated signs of synostosis involving the right femoral head and acetabulum. A fracture was observed in the subtrochanteric area of the right femur, characterized by a beak-shaped thickened cortex on the lateral side of the fracture site. Importantly, the radiographs obtained 3 years prior showed no abnormalities at the fracture site (Figs. 2, 3). Following the diagnosis, the patient underwent open reduction and internal fixation using a plate. Subsequent follow-up indicated successful bone union at the fracture site.
An 8-year-old female patient visited our emergency room complaining of pain in the left thigh that began on the day of her visit. She slipped and directly injured her thigh upon falling to the left. Initial examination revealed normal laboratory findings, including serum calcium levels of 9.0 mg/dL and inorganic phosphorus levels of 4.7 mg/dL. Radiographic evaluations, including anteroposterior and lateral views of the left femur, demonstrated a transverse irregular fracture line in the proximal one-third area of the left femur, accompanied by lateral cortex hypertrophy. Importantly, the possibility of malignancy or infection as contributing factors to the fracture was considered low. Two years prior, the patient had visited the pediatric department of our hospital due to concerns about her height, which was below that of her peers. Following genetic testing, she was diagnosed with osteogenesis imperfecta and has since been monitored by both the pediatrics and orthopedics departments. At that time, lateral bowing of both femurs was observed in both lower extremities during standing anteroposterior evaluations (Figs. 4, 5). She had previously undergone epiphysiodesis on both femurs due to genu valgum. After diagnosis, the patient underwent open reduction and internal fixation using an ender nail. Follow-up evaluations indicated successful bone union at the fracture site.
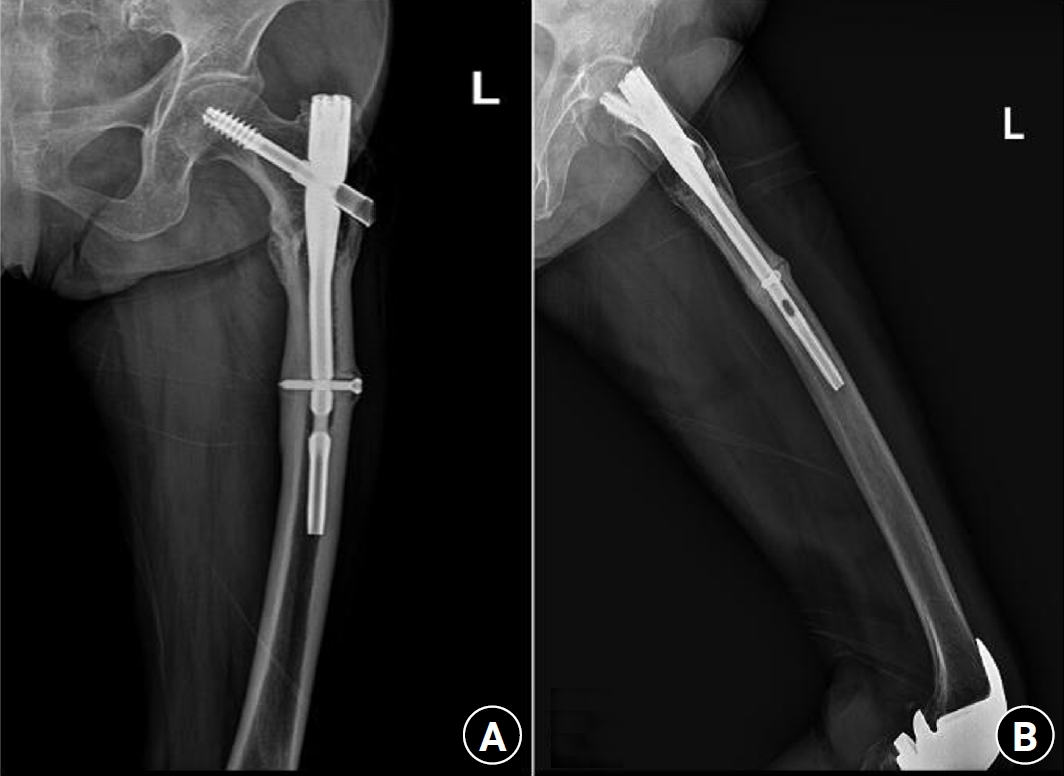
A 73-year-old female patient visited our emergency room complaining of pain in the left thigh that had begun approximately a month ago. She had undergone intramedullary nail fixation for a left femoral intertrochanteric fracture 9 years prior and reported no history of recent trauma. The patient had initially sought treatment at another hospital for her left thigh pain and was discharged after conservative management. However, she experienced sudden severe pain accompanied by a breaking sound while walking. Upon examination, her BMD at the L3‒4 levels was noted to be ‒3.1. The patient also had a history of rheumatoid arthritis and hypertension, with no history of cancer. Radiographic evaluations, including anteroposterior and lateral views of the left femur, revealed a left femoral shaft fracture and metal breakage at the distal locking screw fixation site of the previously inserted intramedullary nail. Notably, when the patient first visited the other hospital, a hypertrophy and microfracture were observed at the lateral site of the distal locking screw insertion (Figs. 6, 7). Following the diagnosis, the patient underwent intramedullary fixation using a long nail. Subsequent follow-up evaluations indicated successful bone union at the fracture site.
Discussion
All three patients had no history of taking bisphosphonates. Hypertrophy of the femur lateral cortex was observed at the fracture site in all three patients. The first patient with synostosis of the hip joint had no range of motion of the right hip joint. As the weight-bearing force was not properly distributed during walking, femur lateral bowing was induced, and tensile force was continuously applied to the lateral cortex of the proximal femur. The second patient had an underlying disease of osteogenesis imperfecta. As a result, the weakened femur showed lateral bowing, and similarly, tensile force acted upon weight-bearing. The other patient underwent intramedullary nail fixation due to a previous femoral intertrochanteric fracture. As the distal locking screw of the intramedullary nail exerted a sustained tensile force on the femur lateral cortex, hypertrophy also occurred around the distal locking screw head.
Since their initial approval, bisphosphonates have been widely used for the prevention of low-energy fractures. This drug is widely considered first-line therapy and the mainstay of primary and secondary insufficiency fracture prevention. However, despite short- and mid-term success, concerns regarding long-term bisphosphonate use and the associated increased risk of insufficiency fractures of the femur have grown over the past 5 years. Several studies have been conducted to determine the association between long-term use of bisphosphonates and femoral insufficiency fractures. While caution is required for long-term use of bisphosphonates, a clear relationship with femoral insufficiency fractures has not yet been established. Accordingly, other causes that can lead to insufficiency fractures have been raised. Long-term glucocorticoid use is known to be associated with the development of insufficiency fractures, with estimates suggesting that over half of chronic glucocorticoid users will develop reduced BMD and fractures. Additionally, prolonged bed rest can lead to disuse osteoporosis due to increased bone resorption and decreased bone formation along with the effect of nutritional factors. Nevertheless, in our study, we aim to report the occurrence of insufficiency fractures related to the patient's bone deformity and force application rather than other environmental or external factors.
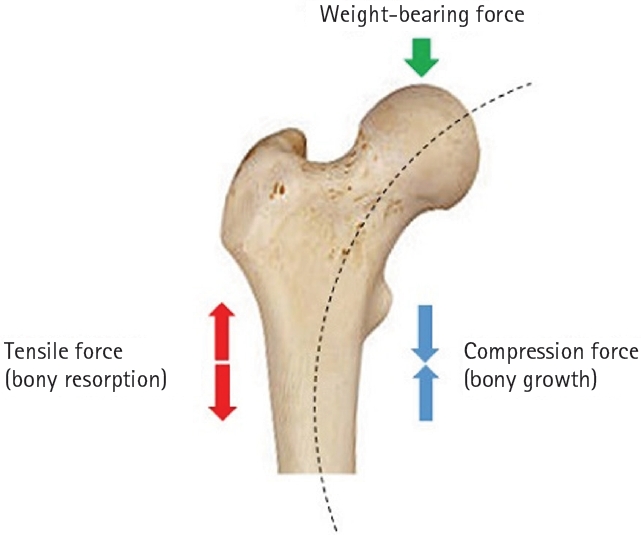
In patients with abnormal bones, whether osteoporotic, bowing, or those who have undergone previous surgery, the opposite of Wolff's law may occur. An adequate understanding of Wolff's law is essential for contextualizing our hypothesis. Proposed by the German anatomist and surgeon Julius Wolff in the 19th century, Wolff's law states that the bone of a healthy animal will adapt to the loads under which it is placed. When a load is applied, bony growth occurs on the side that receives compression force, while bony resorption occurs on the side that experiences tensile force (Fig. 8). Although Wolff's law is primarily applicable to healthy bones, patients with femoral insufficiency fractures do not possess normal healthy bones; instead, they have bones that are osteoporotic, exhibit bowing for various reasons, or have undergone previous surgeries. Therefore, we have termed this phenomenon “paradoxical hypertrophy.”
The phenomenon of paradoxical hypertrophy, which we have named, is thought to arise from several factors. First, tensile force is applied to the lateral cortex due to femoral lateral bowing, and as microfractures and bone healing are repeated in this area, hypertrophy occurs. This hypertrophy of the lateral cortex becomes vulnerable to impact, leading to fractures even with minimal force. Femoral lateral bowing not only progresses with age but can also be exacerbated by the patient's underlying disease or anatomical deformity. The second reason is that hypertrophy occurs at the distal locking screw insertion site in patients who have previously had femoral intramedullary nailing. Similarly, as force is applied to the femur lateral cortex by the head of the distal locking screw, hypertrophy occurs in that area due to repeated microfracture and bone healing. In patients using bisphosphonates, the process of bone resorption is inhibited, leading to an impaired bone remodeling cycle and altering bone mineral and matrix properties, which increases susceptibility to fractures. However, in these three cases, the mechanism is not due to reduced bone turnover from medication, but rather to situations where microdamage accumulates. Initial microfractures fail to heal adequately and are re-injured by new stress, leading to excessive osteoclast-mediated resorption that inhibits normal remodeling and results in the formation of incomplete callus. This mechanism, while opposite to that of bisphosphonate action, ultimately leads to similar outcomes.
In accordance with the American Society for Bone and Mineral Research (ASBMR) [9, 10] diagnostic criteria, each case can be evaluated for insufficiency fractures based on clinical history, imaging findings, and the absence of significant trauma. All three patients demonstrated characteristic features of insufficiency fractures, including specific deformities and forces acting on the femur. In doing so, it is essential to consider the unique circumstances surrounding each case, which collectively suggest that the mechanism of insufficiency fractures may differ from that traditionally associated with long-term bisphosphonate use.
Until now, long-term use of bisphosphonates was thought to be the main cause of femoral insufficiency fractures. However, as demonstrated in our study, repetitive force applied to the femur lateral cortex leads to hypertrophy as a result of microfracture repetition and inadequate healing, culminating in insufficiency fractures in that area.
-
Author contributions
Conceptualization: YUK. Methodology: YUK. Supervision: DHP. Visualization: HGK. Writing–original draft: YUK, HGK. Writing–review & editing: YUK, DHP, HGK. All authors read and approved the final manuscript.
-
Conflicts of interest
No potential conflict of interest relevant to this article was reported.
-
Funding
None.
-
Data availability
Not applicable.
-
Acknowledgments
None.
-
Supplementary material
None.
Article Information
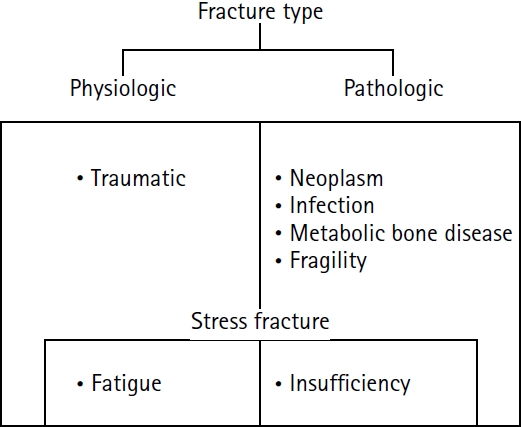
Fig. 2.

Radiograph obtained 3 years earlier of a 58-year-old female patient presenting with a right subtrochanteric femoral fracture (anteroposterior view).
Fig. 3.
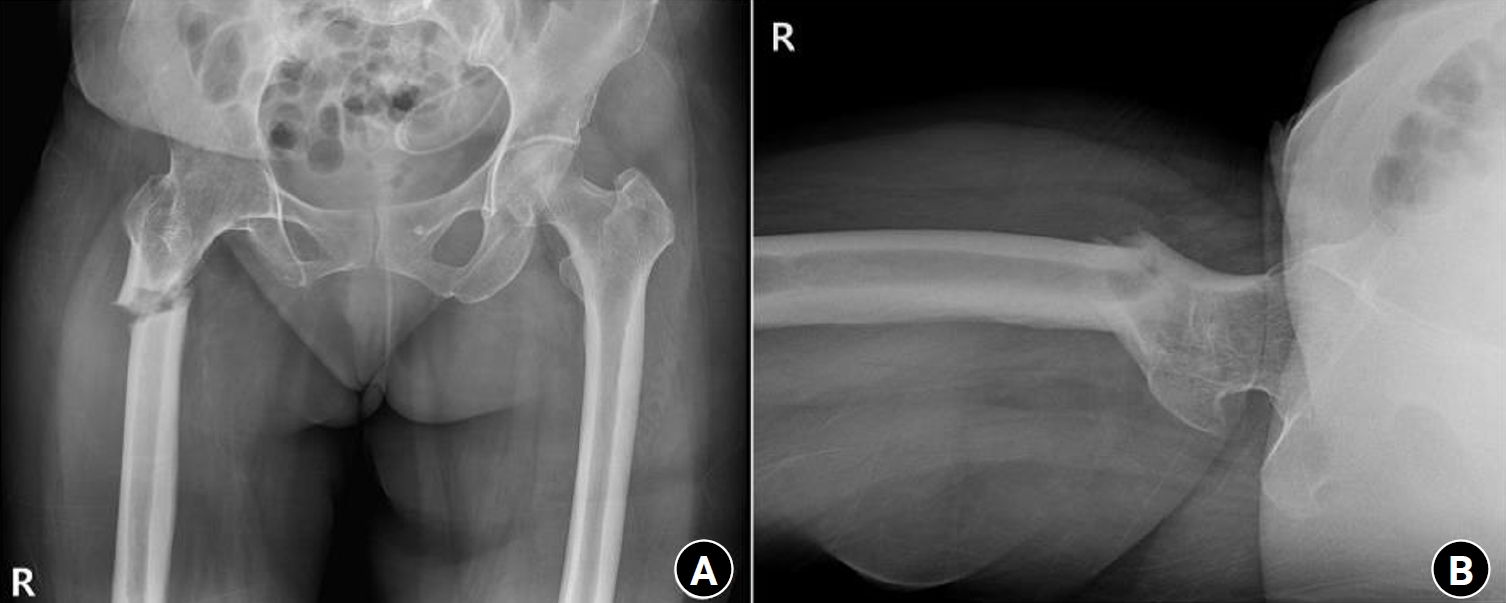
Radiographs of the same patient presenting with a right subtrochanteric femoral fracture (Russell-Taylor classification type 1). (A) Anteroposterior view. (B) Axial view.
Fig. 4.

Prefracture radiograph of an 8-year-old female patient who presented with a proximal one-third fracture of the left femur (bilateral lower-extremity standing anteroposterior view).
Fig. 5.

Radiographs of the same patient with a proximal one-third fracture of the left femur. (A) Anteroposterior view. (B) Lateral view.
Fig. 6.
Prefracture radiographs of a 73-year-old female patient who subsequently presented with a femoral shaft fracture demonstrating cortical hypertrophy and microfracture. (A) Anteroposterior view. (B) Lateral view.
Fig. 7.

Radiographs of the same patient with a femoral shaft fracture and implant failure. (A) Anteroposterior view. (B) Lateral view.
- 1. Pentecost RL, Murray RA, Brindley HH. Fatigue, insufficiency, and pathologic fractures. JAMA 1964;187:1001-4.ArticlePubMed
- 2. Fayad LM, Kawamoto S, Kamel IR, et al. Distinction of long bone stress fractures from pathologic fractures on cross-sectional imaging: how successful are we? AJR Am J Roentgenol 2005;185:915-24.ArticlePubMed
- 3. Matcuk GR Jr, Mahanty SR, Skalski MR, Patel DB, White EA, Gottsegen CJ. Stress fractures: pathophysiology, clinical presentation, imaging features, and treatment options. Emerg Radiol 2016;23:365-75.ArticlePubMedPDF
- 4. Court-Brown CM, McQueen MM. Global forum: fractures in the elderly. J Bone Joint Surg Am 2016;98:e36.ArticlePubMed
- 5. Isaacs JD, Shidiak L, Harris IA, Szomor ZL. Femoral insufficiency fractures associated with prolonged bisphosphonate therapy. Clin Orthop Relat Res 2010;468:3384-92.ArticlePubMedPMC
- 6. Rogers LF, Taljanovic M. FDA statement on relationship between bisphosphonate use and atypical subtrochanteric and femoral shaft fractures: a considered opinion. AJR Am J Roentgenol 2010;195:563-6.ArticlePubMed
- 7. Ha YC, Cho MR, Park KH, Kim SY, Koo KH. Is surgery necessary for femoral insufficiency fractures after long-term bisphosphonate therapy? Clin Orthop Relat Res 2010;468:3393-8.ArticlePubMedPMC
- 8. Rudran B, Super J, Jandoo R, et al. Current concepts in the management of bisphosphonate associated atypical femoral fractures. World J Orthop 2021;12:660-71.ArticlePubMedPMC
- 9. Shane E, Burr D, Ebeling PR, et al. Atypical subtrochanteric and diaphyseal femoral fractures: report of a task force of the American Society for Bone and Mineral Research. J Bone Miner Res 2010;25:2267-94.ArticlePubMed
- 10. Shane E, Burr D, Abrahamsen B, et al. Atypical subtrochanteric and diaphyseal femoral fractures: second report of a task force of the American Society for Bone and Mineral Research. J Bone Miner Res 2014;29:1-23.ArticlePubMed
References
Figure & Data
REFERENCES
Citations
Citations to this article as recorded by 
 ePub Link
ePub Link Cite
CiteParadoxical hypertrophy as a cause of femoral insufficiency fractures analyzed through differences in force application in Korea: three case reports
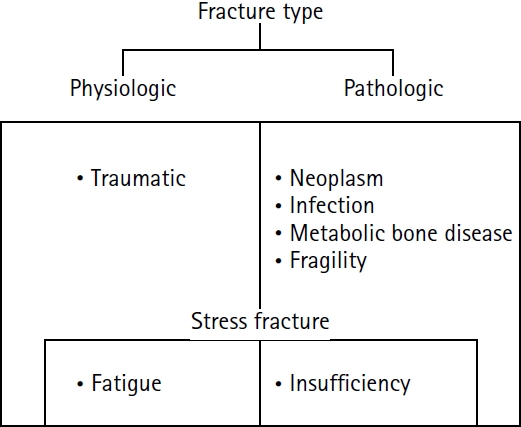

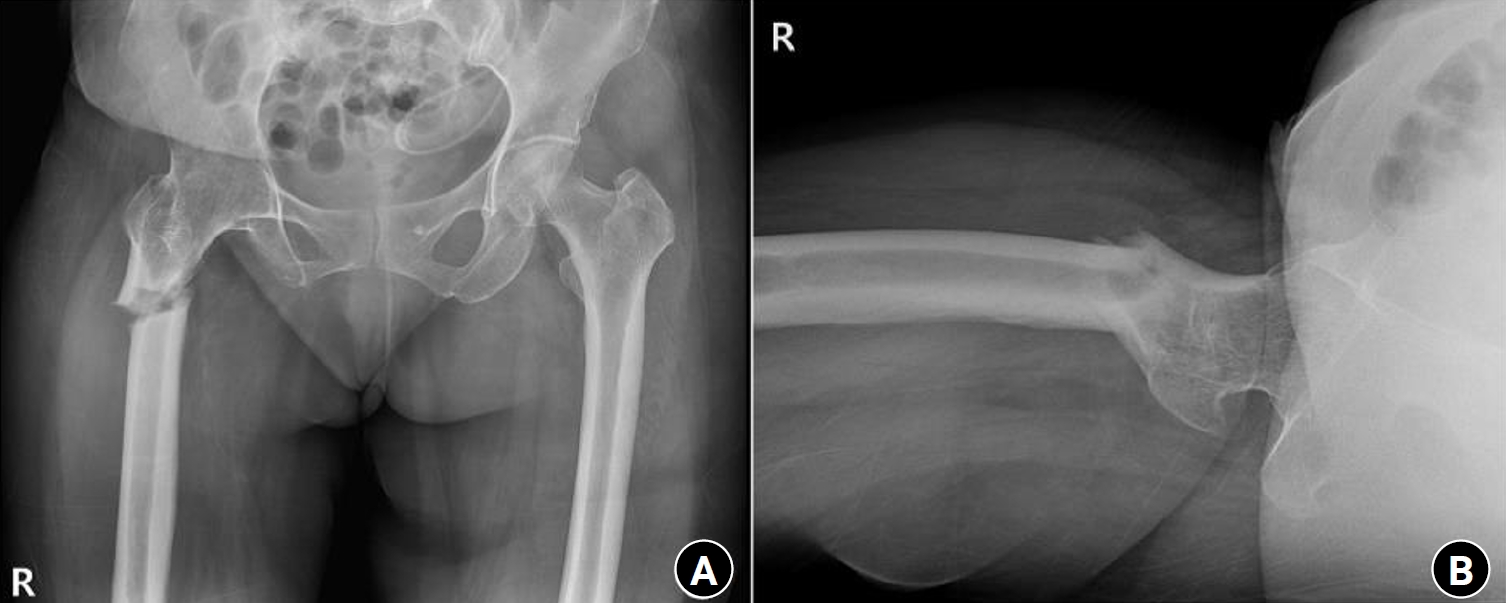


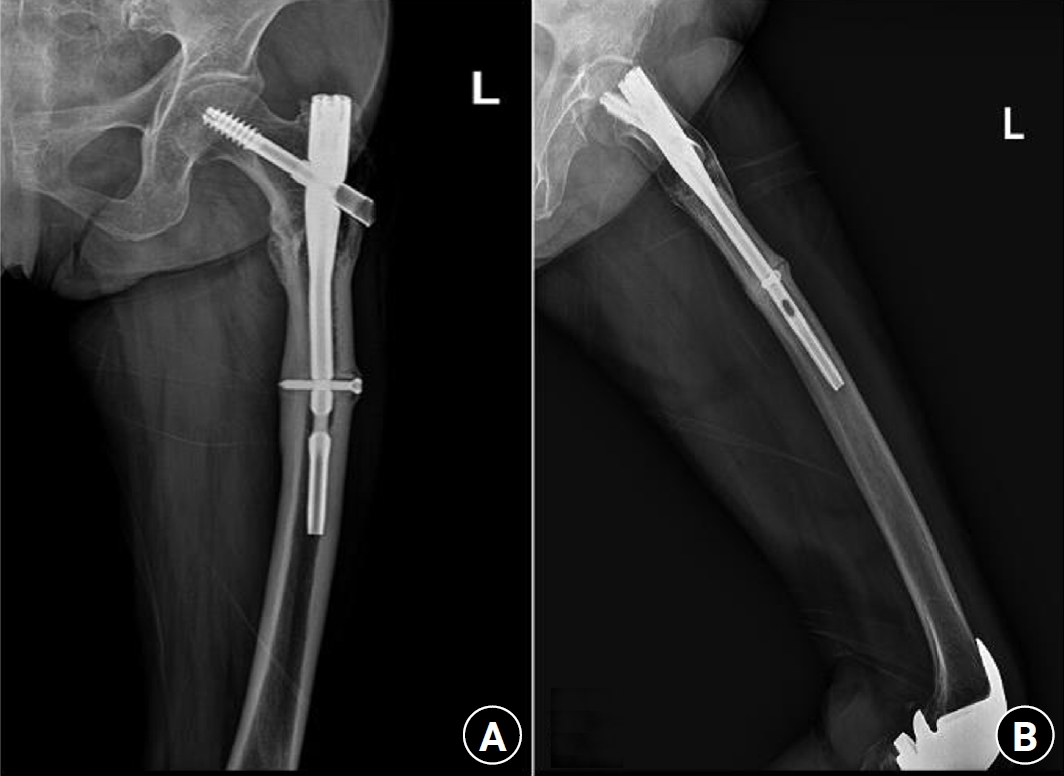

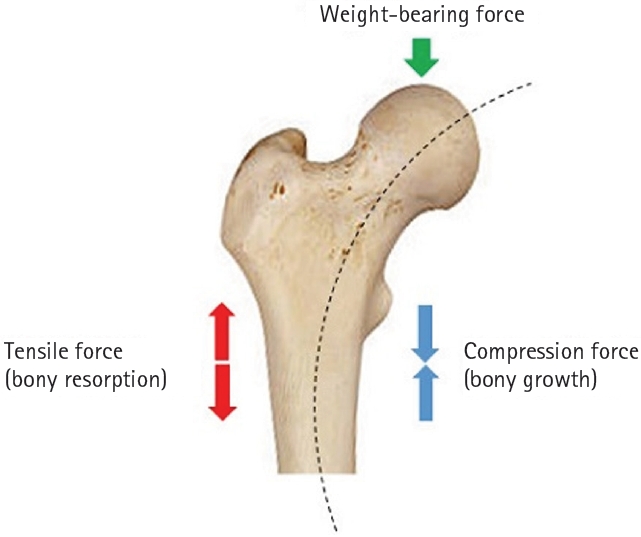
Fig. 1. Schematic diagram illustrating the classification of fractures.
Fig. 2. Radiograph obtained 3 years earlier of a 58-year-old female patient presenting with a right subtrochanteric femoral fracture (anteroposterior view).
Fig. 3. Radiographs of the same patient presenting with a right subtrochanteric femoral fracture (Russell-Taylor classification type 1). (A) Anteroposterior view. (B) Axial view.
Fig. 4. Prefracture radiograph of an 8-year-old female patient who presented with a proximal one-third fracture of the left femur (bilateral lower-extremity standing anteroposterior view).
Fig. 5. Radiographs of the same patient with a proximal one-third fracture of the left femur. (A) Anteroposterior view. (B) Lateral view.
Fig. 6. Prefracture radiographs of a 73-year-old female patient who subsequently presented with a femoral shaft fracture demonstrating cortical hypertrophy and microfracture. (A) Anteroposterior view. (B) Lateral view.
Fig. 7. Radiographs of the same patient with a femoral shaft fracture and implant failure. (A) Anteroposterior view. (B) Lateral view.
Fig. 8. Schematic illustration of Wolff’s law.
Fig. 1.
Fig. 2.
Fig. 3.
Fig. 4.
Fig. 5.
Fig. 6.
Fig. 7.
Fig. 8.
Paradoxical hypertrophy as a cause of femoral insufficiency fractures analyzed through differences in force application in Korea: three case reports

