 E-submission
E-submission TOTA
TOTA TOTS
TOTS
Articles
- Page Path
- HOME > J Musculoskelet Trauma > Volume 39(2); 2026 > Article
-
Original Article
- Percutaneous anterior leverage technique for anteromedial cortical support in intertrochanteric femur fractures: a computed tomography-based validation study
-
Whee Sung Son*
 , Bum Jin Shim*, Oog-jin Shon
, Bum Jin Shim*, Oog-jin Shon -
Journal of Musculoskeletal Trauma 2026;39(2):117-129.
DOI: https://doi.org/10.12671/jmt.2025.00311
Published online: March 27, 2026
Department of Orthopedic Surgery, Yeungnam University Medical Center, Yeungnam University College of Medicine, Daegu, Korea
- Correspondence to: Whee Sung Son Department of Orthopedic Surgery, Yeungnam University Medical Center, Yeungnam University College of Medicine, 170 Hyonchung-ro, Nam-gu, Daegu 42415, Korea Tel: +82-53-620-3640, Email: oswsson@gmail.com
- Co-Correspondence to: Oog-jin Shon Department of Orthopedic Surgery, Yeungnam University Medical Center, Yeungnam University College of Medicine, 170 Hyonchung-ro, Nam-gu, Daegu 42415, Korea Tel: +82-53-620-3640, Email: ossoj@ynu.ac.kr
- *These authors contributed equally to this work as first authors.
• Received: September 24, 2025 • Revised: December 9, 2025 • Accepted: December 10, 2025
© 2026 The Korean Orthopaedic Trauma Association
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/4.0/) which permits unrestricted noncommercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
- 1,214 Views
- 42 Download
Abstract
-
Background Anteromedial cortical support (AMCS) enhances stability in intertrochanteric femur fractures. However, reproducible, validated methods of achieving AMCS have not previously been reported. This study introduces a percutaneous anterior leverage technique and validates its AMCS effects using computed tomography (CT).
-
Methods We retrospectively reviewed patients treated by a single surgeon between March 2022 and December 2024. The inclusion criteria were an AO/OTA classification of A1–A3, application of the percutaneous anterior leverage technique, available pre- and postoperative CT, and ≥6 months follow-up. Outcomes included CT-based AMCS (anterior on axial and medial on coronal images, classified as positive, neutral, or negative), time to union, union rate, changes in neck-shaft angle, and treatment failure (varus collapse, blade cut-through, or nonunion without the former two). The risk factors for failure were analyzed.
-
Results Of 273 patients reviewed, 53 met the inclusion criteria. Follow-up was at least 6 months in all cases. Positive anterior support was achieved in 37 patients (69.8%) and positive medial support in 42 (79.25%). No patient demonstrated negative anterior support; one (1.9%) had negative medial support. Cortical support improved significantly after surgery. CT images demonstrated significant postoperative improvements (anterior P=0.026; medial P<0.001). Bone union was achieved in 50 patients (94.34%) at a mean of 3.93±1.48 months. The mean change in the neck-shaft angle at last follow-up was 1.75°±2.34° varus. Three patients (5.66%) experienced treatment failure. Anteromedial cortical breakage during follow-up differed between failure and nonfailure groups (P=0.002), but regression identified no independent predictors. No technique-related complications were observed.
-
Conclusions Our percutaneous anterior leverage technique produced favorable CT-confirmed AMCS and high union with low failure, supporting its safety and effectiveness in intertrochanteric femur fractures.
-
Level of evidence IV.
Introduction
Femoral intertrochanteric fractures are among the most common types in the geriatric population, and they are considered a life-threatening injury [1]. Potentially fatal complications related to immobilization are frequent, so early rehabilitation is essential [2]. However, early rehabilitation is often difficult to achieve in such patients owing to the high risk of reduction loss, making femoral intertrochanteric fractures particularly challenging to treat.
Anteromedial cortical support (AMCS) is a well-recognized means of addressing these challenges and achieving stable fixation in femoral intertrochanteric fractures [3]. Several studies have reported favorable outcomes, with AMCS providing support between the anteromedial cortex of the head-neck segment and the distal segment. This achieves secondary stability and promotes fracture healing [4-6].
However, surgical methods for achieving AMCS have not been described in detail in the existing literature, and there has been no validation of such techniques. Kim et al. [7] have described eight cases in which a bone hook leverage technique was used. This is performed through the entry incision for intramedullary nailing. Kozono et al. [8] have reported direct reduction using a small elevator in six cases. They note that closed reduction of the anterior cortex is challenging due to the strong attachment of the iliofemoral ligament to the anterior intertrochanteric crest. However, both of these studies were limited by a small number of cases and lacked validation. Furthermore, other studies addressing AMCS did not provide detailed descriptions of surgical methods. Consequently, no study has validated a single technique in an adequately-sized sample.
Therefore, the authors of the present study considered it necessary to establish and validate a surgical technique that allows surgeons to obtain AMCS in a reproducible manner. This study introduces the percutaneous anterior leverage technique, providing a detailed description of the method. It also aims to validate its effectiveness. As computed tomography (CT) provides a more accurate assessment than plain radiography, validation was based on CT evaluation.
Methods
The study adhered to the principles of the 1964 Declaration of Helsinki and its subsequent revisions, and was approved by the Institutional Review Board (IRB) of Yeungnam University Medical Center (IRB No. YUMC 2025-09-019). In accordance with institutional and ethical guidelines, informed consent was obtained from all participants.
This study was a single-center retrospective case series of patients treated for femoral intertrochanteric fractures.
This study was conducted at Yeungnam University Medical Center, Daegu, Korea, between March 2022 and December 2024. The surgical indication criteria for applying the technique were as follows: if preoperative CT in either the axial or coronal plane demonstrated loss of AMCS, a closed reduction maneuver was performed before draping. When fluoroscopic evaluation in both the anteroposterior (AP) and lateral views failed to restore positive AMCS, the percutaneous anterior leverage technique was subsequently applied to achieve adequate AMCS (Fig. 1). The procedure was performed by a single orthopedic trauma surgeon (WSS) between March 2022 and December 2024.
Each patient was positioned on a fracture table, and their overall limb length and approximate neck-shaft angle were restored using the fracture table prior to draping. A 2 cm incision was made along the Smith-Petersen interval (Fig. 2A). Blunt dissection was then performed using blunt Kelley hemostatic forceps to reach the anterior cortex of the femur. Under a fluoroscopic AP view, the position was adjusted to ensure that the forceps were located at the anteromedial cortex of the fracture site, taking care not to extend medially toward the femoral artery (Fig. 2B, 2C). The forceps were then exchanged for a freer retractor, which was safely advanced and positioned at the anteromedial cortex of the fracture site. Subsequently, fluoroscopy was switched to the lateral view. This enabled confirmation of the correct advancement of the freer retractor into the fracture site (Fig. 2D, 2E). The anteromedial cortex of the proximal segment is usually displaced into the intramedullary space of the distal segment. Therefore, the retractor is advanced obliquely, from cephalad to caudal and from medial to lateral, to gain access. Once fluoroscopic confirmation was obtained, the intramedullary-displaced proximal anteromedial cortex was levered into an extramedullary reduced state with the freer retractor. This achieved a positive AMCS state (Fig. 2F, 2G). A 3.2 mm Steinmann pin was then introduced from the anterolateral cortex of the distal segment and advanced toward the proximal segment through an anterior trajectory for temporary fixation. This avoids the passage of the intramedullary nail (Fig. 2F) [9]. During the procedure, the lateral fluoroscopic view was used to verify positive anterior cortical support, and the AP view was used to verify positive medial cortical support. Following these steps, conventional intramedullary nailing was performed using the TFN-ADVANCED Proximal Femoral Nailing System (TFNA; DePuy Synthes). The anteriorly placed freer retractor did not interfere with nail insertion and maintained AMCS of the proximal segment (Fig. 2H, 2I). After blade insertion, compression was applied through the blade as the retractor was gradually withdrawn. This ensured final compression in a complete positive AMCS state (Fig. 2J). Finally, distal interlocking screws were placed, completing the procedure (Figs. 2K, 3). Throughout the procedure, the lateral fluoroscopic view was obtained not as an axial projection aligning the femoral head-neck with the femoral shaft, but rather, as a 30° oblique tangential projection. This allowed optimal visualization of the anteromedial cortical state [10].
Postoperatively, weight bearing was initiated as soon as the patient’s pain became tolerable, and walker-assisted ambulation was achieved within 2 weeks. The patient was then transferred to a rehabilitation hospital. Follow-up evaluations to monitor rehabilitation progress and assess for any complications were conducted at 1, 2, 3, 5, 7, 10, and 13 months postoperatively.
The inclusion criteria were (1) femoral intertrochanteric fractures classified as AO/OTA types A1, A2, and A3; (2) use of the percutaneous anterior leverage technique; (3) availability of preoperative and postoperative CT scans; (4) a minimum postoperative follow-up period of 6 months; and (5) availability of complete medical records and radiographic data for review.
The index exposure (intervention) was the application of the percutaneous anterior leverage technique. The primary outcome was CT-based postoperative AMCS, assessed as anterior cortical support on axial CT, and medial cortical support on coronal CT, each classified as positive, neutral, or negative. Secondary outcomes included bone union (yes/no) and time to union (months), change in neck-shaft angle, treatment failure, and technique-related complications.
Data were collected from institutional medical records on patient demographics, operative times, AO/OTA fracture classifications, and Dorr types. Tip to apex distance (TAD), blade position, the difference between the postoperative and contralateral neck-shaft angles (representing varus or valgus alignment relative to the contralateral hip), and the occurrence of anteromedial cortical breakage during follow-up were assessed using plain radiographs and CT images. These variables were included in an analysis of risk factors for treatment failure. Anteromedial cortical breakage during follow-up was included in the failure analysis because it was anticipated that, even if AMCS was initially achieved, subsequent cortical breakage could nullify this support.
Outcomes were assessed using plain radiographs and CT images. Plain radiographic evaluations assessed time to union, achievement of bone union (defined as bridging callus formation across at least three cortices with no signs of implant failure or further displacement), and the difference in neck-shaft angle between the postoperative period and the final follow-up. This latter measure reflects the degree of varus displacement during the follow-up period. Varus collapse (defined as a decrease in the neck-shaft angle of >10° compared with the postoperative measurement) [11], blade cut-through, and nonunion in the absence of varus collapse or blade cut-through were also evaluated. The presence of any of these three was defined as treatment failure.
Axial CT images were used to evaluate anterior cortical support, which was classified as positive, neutral, or negative. When the anteromedial cortex of the proximal segment was located anterior to that of the distal segment, anterior cortical support was classified as positive. When both cortices were aligned, it was classified as neutral. When the proximal cortex was located posterior to the distal cortex, it was classified as negative. Coronal CT images were used to assess medial cortical support. This was also classified as positive, neutral, or negative. When the anteromedial cortex of the proximal segment was located medial to that of the distal segment, medial cortical support was classified as positive. When both cortices were aligned, it was classified as neutral. When the proximal cortex was located lateral to the distal cortex, it was classified as negative (Fig. 4). These assessments were performed on both preoperative and postoperative CT scans. Postoperative AMCS status was evaluated as an outcome of the percutaneous anterior leverage technique and was included in the treatment failure risk factor analysis. It was also compared with the preoperative status in each patient to assess the changes resulting from the use of the technique. In addition, we performed subgroup analyses based on patient demographics and fracture characteristics (AO/OTA classification and Dorr type), reporting the postoperative AMCS within each subgroup. Complications such as femoral artery injury associated with the percutaneous anterior leverage technique were also assessed.
To mitigate bias in this retrospective, single-center study, we employed prespecified eligibility criteria and an indication pathway, including only patients with paired pre- and postoperative CTs, complete records, and a minimum of 6 months of follow-up. CT-based grading of anterior and medial cortical support reduced misclassification compared to plain radiographs. Outcomes—such as union, neck-shaft angle change, and failure components—were defined as a priori using objective radiographic criteria. A single surgeon performed all procedures to minimize variability, while potential confounders, including age, fracture type, position, and TAD, were examined using univariate and multivariable analyses.
Because this was a single-center retrospective review, no a priori sample-size calculation was performed; instead, the study size was determined by the number of patients who met all eligibility criteria during the study period.
We used IBM SPSS ver. 27.0 (IBM Corp.) for all analyses. Continuous data were tested for normality of distribution. Accordingly, the Student t-test or the Mann-Whitney U test was used to compare two groups. Categorical data were evaluated using Pearson chi-square test or Fisher exact test. Variables associated with treatment failure were assessed using univariate analysis. A multivariate logistic regression model was intended to further analyze the variables found to be statistically significant in the univariate analysis. P-values <0.05 were deemed statistically significant.
Results
Among 273 patients reviewed, 53 patients met the inclusion criteria and were enrolled in the study (Fig. 5). The mean age of the enrolled patients was 81.36±8.43 years, and the sample comprised 22 males and 31 females. The AO/OTA classification was type A1 in 24 cases (45.28%), type A2 in 21 cases (39.62%), and type A3 in eight cases (15.09%). The Dorr classification was type A in 16 patients (30.19%), type B in 24 patients (45.28%), and type C in 13 patients (24.53%).
On preoperative axial CT scans, anterior cortical support was positive in three patients (5.66%), neutral in four patients (7.55%), and negative in 46 patients (86.79%). In the coronal view, medial cortical support was positive in five patients (9.43%), neutral in nine patients (16.98%), and negative in 39 patients (73.58%). Thus, most patients demonstrated negative AMCS in both the axial and coronal views.
The mean TAD was 10.75±3.77 mm, and no patient had a TAD greater than 25 mm. Blade position was center-center in 12 patients (22.64%), inferior-center in 38 patients (71.70%), and inferior-posterior in three patients (5.66%). The mean difference between the postoperative and contralateral neck-shaft angles was 3.09°±4.16° in valgus. This indicated that the postoperative neck-shaft angle was slightly more valgus than the contralateral side. The mean operative time was 34.15±10.21 minutes. During the follow-up period, there were two cases (3.77%) of anteromedial cortical breakage (Table 1).
The postoperative axial CT scans revealed that 37 patients (69.81%) had positive anterior cortical support, 16 patients (30.19%) had neutral support, and none had negative support. In the coronal CT scans, 42 patients (79.25%) demonstrated positive medial cortical support, 10 patients (18.87%) neutral support, and one patient (1.89%) negative support. There was a significant preoperative to postoperative improvement in anterior cortical support on the axial CT views (P=0.026), as well as in medial cortical support on the coronal views (P<0.001) (Table 2).
Bone union was achieved in 50 patients (94.34%), with a mean time to union of 3.93±1.48 months. The mean change in the neck-shaft angle between the postoperative period and the final follow-up was 1.75°±2.34° in varus. Nonunion in the absence of varus collapse or blade cut-through occurred in one patient (1.89%), and blade cut-through in one patient (1.89%). Varus collapse was seen in one patient (1.89%), despite the achievement of bone union during long-term follow-up. This case was classified as a treatment failure. Thus, three cases (5.66%) in total were categorized as treatment failures (Table 3). Interestingly, all instances of anteromedial cortical breakage during follow-up were in patients who experienced treatment failure (Fig. 6). Specifically, it occurred in the patients with blade cut-through and varus collapse. It was not seen in the patient with nonunion in the absence of varus collapse or blade cut-through, in whom reduction was maintained, but bone union was not achieved. This patient had multiple comorbidities—including bladder cancer, chronic kidney disease, cerebral infarction, alcoholic liver cirrhosis, diabetes, and hypertension—and it is presumed that these host factors contributed to the development of nonunion.
In subgroup analyses evaluating postoperative AMCS across demographic and fracture-related subgroups, age and Dorr type showed significant differences in postoperative anterior cortical support. Patients with postoperative positive anterior cortical support had a mean age of 83.0±6.6 years, whereas those with neutral cortical support had a mean age of 77.6±11.0 years (P=0.030). Regarding Dorr classification, type C showed 11 postoperative anterior cortical positive (84.62%) and two neutral (15.38%); type B showed 19 positive (79.17%) and five neutral (20.83%); and type A showed seven positive (43.75%) and nine neutral (56.25%; P=0.037). No significant differences were observed in the other subgroup categories with respect to postoperative AMCS (Table 4).
In a comparison of the treatment failure and success groups for risk factor analysis, we found no significant differences in the demographic or fracture variables. Only anteromedial cortical breakage during follow-up differed significantly between the two groups (P=0.002) (Table 5). As univariate logistic regression analysis did not identify any significant factors, multivariate logistic regression analysis was not performed (Table 6). No complications associated with the percutaneous anterior leverage technique occurred.
Discussion
This study demonstrates that the percutaneous anterior leverage technique is a reproducible and effective method for achieving AMCS in intertrochanteric femur fractures. Using CT for validation, the technique consistently converted preoperative negative AMCS into positive or neutral states, resulting in a high union rate and low incidence of treatment failure. Importantly, no complications related to the procedure were observed. To our knowledge, this is the first study to provide a detailed description of a surgical method for obtaining AMCS and to validate its clinical effectiveness through CT-based evaluation, thereby addressing a critical unresolved issue in the current literature.
To date, only two studies have provided specific descriptions of direct reduction techniques aimed at achieving AMCS. Kozono et al. [8] reported six cases treated with various direct reduction approaches, in which five cases (83.33%) achieved neutral or positive anterior cortical support, while one case (16.67%) demonstrated negative support. Medial cortical support outcomes were not reported in their study. Kim et al. [7] described the use of bone hook leverage via incision of the intramedullary nail entry in eight cases. Although they assessed reduction quality based on whether displacement of the anterior and medial cortices was <1 cortical thickness, they did not classify outcomes into positive, neutral, or negative categories. Among the eight cases, five cases (62.50%) demonstrated <1 cortical thickness displacement in both the anterior and medial cortices, whereas the remaining three cases (37.50%) had ≥1 cortical thickness displacement in at least one of the two cortices. Because their study did not employ a clear classification system for AMCS, the interpretation of their outcomes is limited with respect to the AMCS concept.
In this study, we observed negative AMCS in only one patient (1.89%), with all other patients achieving at least neutral AMCS. Positive anterior cortical support was achieved in 69.81% and positive medial cortical support in 79.25%. Although AMCS appeared to be restored on intraoperative fluoroscopy, postoperative CT did not demonstrate positive support in all cases. This discrepancy is likely attributable to differences between plain radiographic and CT-based assessments of AMCS, as described in detail later in the Discussion. A direct comparison with other techniques is not feasible because previous studies have not validated a single method for achieving AMCS. Nevertheless, the bone union rate of 94.34% in this older cohort (mean age, 81.36±8.43 years) may be considered favorable. The percutaneous anterior leverage technique for achieving AMCS offers several advantages. First, it utilizes a separate incision and anterior plane, which do not interfere with the intramedullary nailing procedure. Second, maintaining leverage with the freer retractor throughout the nailing process helps to prevent re-displacement during intramedullary nail fixation. Finally, because the procedure is performed percutaneously, it is minimally invasive and does not appear to substantially increase operative time (mean operative time, 34.15±10.21 minutes), although no direct comparison with other methods was possible. However, potential pitfalls of this technique include the risk of injury to the medial femoral circumflex artery and the possibility of lateral femoral cutaneous nerve injury, even though no such events were observed in the present cohort. Therefore, careful attention to these anatomical structures is warranted during the procedure.
Subgroup analyses of postoperative AMCS across demographic and fracture-related categories revealed that older patients were more likely to achieve postoperative positive anterior cortical support than neutral support. Similarly, patients with Dorr type C and type B demonstrated higher rates of postoperative positive anterior cortical support compared with neutral support. Notably, no cases of negative anterior cortical support were observed in this study. These findings suggest that the percutaneous anterior leverage technique may offer particular advantages in patient groups—such as older individuals and those with Dorr type B or C morphology—who are generally considered at higher risk for treatment failure.
Our risk factor analysis for treatment failure found no significant relationships between treatment failure and patient variables, including age, sex, AO/OTA classification, and Dorr type. Notably, eight patients (15.09%) had AO/OTA type A3 fractures, which are generally considered to carry a high risk of fixation failure, yet no significant association was observed. This suggests that favorable outcomes may be achieved even in A3 intertrochanteric fractures when AMCS is obtained using this technique. The mean TAD was 10.75±3.77 mm, and no patient had a TAD greater than 25 mm. Blade position was not unfavorable in any of the patients [12], and the neck-shaft angle compared with the contralateral side was, on average, 3.09°±4.16° in valgus. All of these fracture characteristics are considered acceptable. However, anteromedial cortical breakage during follow-up was significantly correlated with treatment failure (P=0.002 in a comparison between the treatment failure and success groups). However, statistical significance was not confirmed in a regression analysis. Anteromedial cortical breakage was observed in the patient with varus collapse and the patient with blade cut-through. In contrast, reduction was maintained in the patient with nonunion without varus collapse or blade cut-through, and anteromedial cortical breakage did not occur. These findings suggest that, even when AMCS is initially achieved, subsequent anteromedial cortical breakage can result in reduction loss, thereby increasing the risk of treatment failures such as varus collapse or blade cut-through. Thus, careful monitoring for anteromedial cortical breakage during follow-up is warranted. However, further studies with more cases of treatment failure are required to validate this observation. Moreover, because the temporal relationship could not be determined, it remains unclear whether anteromedial cortical breakage was a cause or a consequence of treatment failure, limiting the interpretation of this finding. In addition, although not observed in the cohort of the present study, it is reasonable to assume that preoperative anteromedial cortical comminution would diminish the effectiveness of the percutaneous anterior leverage technique, as the technique relies on an intact cortical buttress to achieve and maintain reduction. In such cases, the method may be insufficient to provide durable stability, and the development of additional strategies or adjunctive techniques to ensure reliable fixation may be required.
Previous studies have raised concerns about neutral cortical support. Li et al. [13] reported that among 46 patients, 16 patients (34.8%) with intraoperative neutral medial cortical support progressed to negative cortical support at 6 months postoperatively. They concluded that neutral cortical support, particularly medial, as assessed by fluoroscopy, is associated with a high rate of fracture reduction loss during follow-up. In the present study, CT imaging found that 16 of the 53 patients (30.19%) had neutral anterior cortical support, and 10 (18.87%) had neutral medial cortical support. However, despite these numbers, only three cases (5.66%) of treatment failure were observed. This may be explained by Mao et al. [4]’s suggestion that previous studies may have misclassified cases of negative cortical support as neutral because evaluations were based on plain radiographs rather than CT. As our study validated cortical support states using CT, the assessments were likely to have been more accurate. Moreover, we did not find neutral cortical support to be a significant risk factor in our treatment failure analysis, suggesting that neutral cortical support may be acceptable. Mao et al. [4] have further posited that poor outcomes following neutral cortical support could result from secondary interfragmentary movement or sliding, which may lead to loss of immediate postoperative neutral reduction. However, in the percutaneous anterior leverage technique, the freer retractor used to maintain AMCS is removed only after compression has been performed through the blade. This ensures that compression is achieved in the AMCS position. This approach may have helped to prevent changes from neutral to negative cortical support [11]. In summary, neutral cortical support, as assessed by CT, combined with intraoperative blade compression to prevent secondary interfragmentary movement, does not appear to be a risk factor for treatment failure and may be considered an acceptable outcome.
First, it included only 53 patients, so further studies with larger sample sizes are needed. However, to our knowledge, this is the largest study to date that has focused on a single technique for achieving AMCS. Second, only three patients experienced treatment failure, which limited the validity and reliability of the risk factor analysis. Studies with larger samples are needed to obtain larger numbers of treatment failure cases. Third, bone mineral density (BMD) was not included as a variable in this study. Because incorporating only patients with available BMD measurements would have substantially reduced the sample size, it was excluded; nevertheless, given that bone quality can significantly influence fixation stability and fracture healing, this remains an important limitation. Fourth, comparative studies that include other techniques are needed to fully establish the utility of this method. Finally, all surgeries were performed by a single surgeon. Future multicenter studies with multiple surgeons would strengthen the generalizability of the findings.
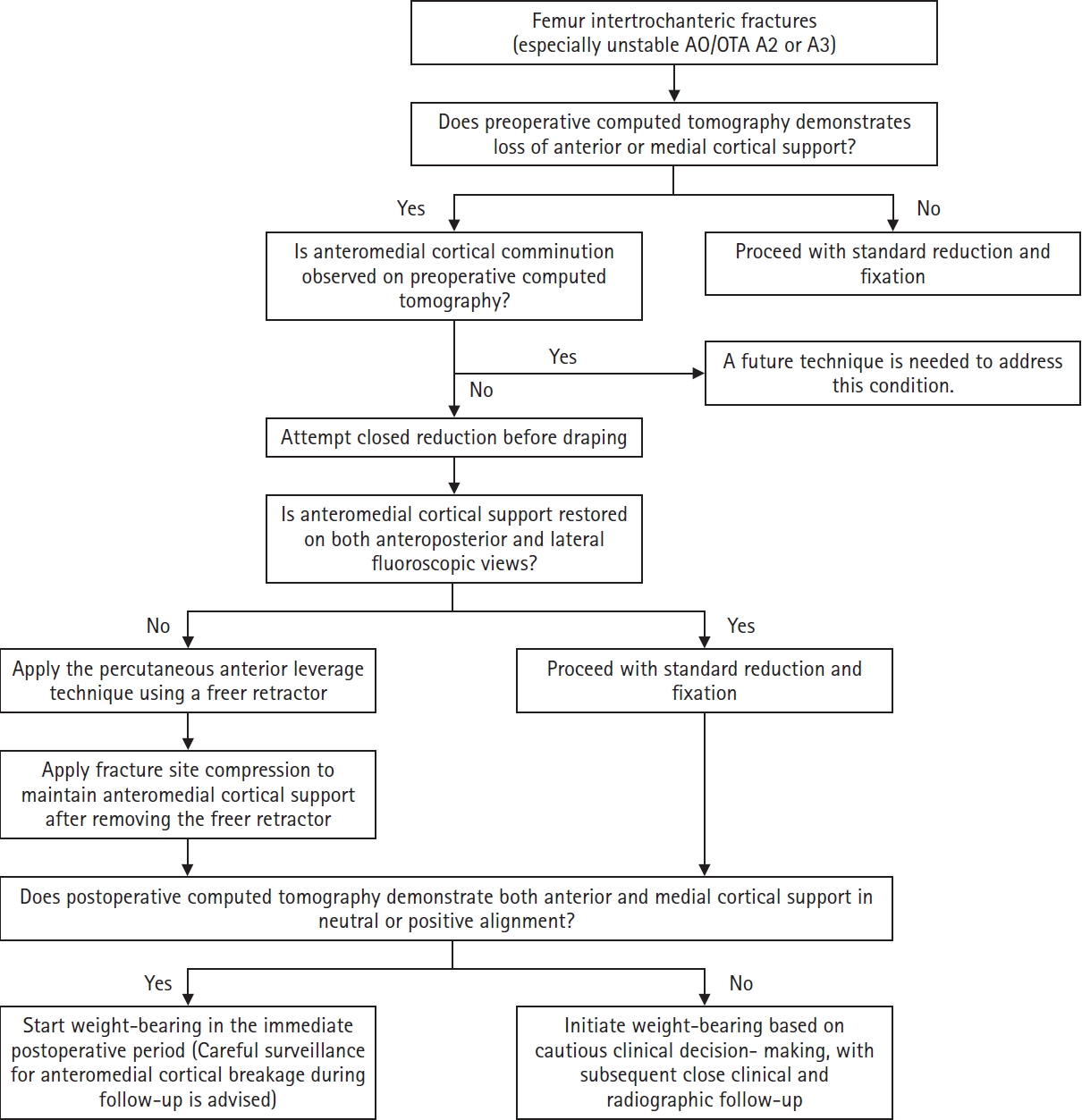
Despite these limitations, the findings of this study allow for the proposal of a practical clinical decision pathway for applying the percutaneous anterior leverage technique. In patients with intertrochanteric femur fractures—particularly unstable AO/OTA A2 or A3 patterns—preoperative CT should first be evaluated for loss of AMCS. When the AMCS loss is identified and the anteromedial cortex is intact without comminution, a closed reduction maneuver is recommended before draping. If intraoperative fluoroscopic assessment in both AP and lateral views confirms restoration of AMCS, standard reduction and fixation may proceed. However, if both anterior and medial cortical support cannot be restored, the percutaneous anterior leverage technique should be applied to achieve adequate reduction, followed by fracture site compression to maintain the achieved AMCS. Postoperative CT should then be used to confirm both anterior and medial cortical support in either a neutral or positive state, as discrepancies between intraoperative fluoroscopy and postoperative CT assessment may occur. When postoperative AMCS is confirmed on CT, immediate weight bearing should be initiated, with continued surveillance for potential anteromedial cortical breakage during the follow-up period (Fig. 7).
The percutaneous anterior leverage technique for AMCS in femoral intertrochanteric fractures resulted in positive anterior cortical support in 69.81% and positive medial cortical support in 79.25% of cases, as evidenced by CT imaging. Only one of the 53 patients showed negative medial cortical support. In addition, 94.34% of patients achieved bone union without technique-related complications. These findings suggest that the percutaneous anterior leverage technique is a safe and effective method with which to achieve AMCS in femoral intertrochanteric fractures.
-
Author contributions
Conceptualization: WSS. Data curation: WSS, BJS, OS. Formal analysis: WSS, BJS, OS. Funding acquisition: WSS. Investigation: WSS, BJS, OS. Methodology: WSS. Validation: WSS, BJS, OS. Writing–original draft: WSS, BJS. Writing–review & editing: WSS, BJS, OS. All authors read and approved the final manuscript.
-
Conflicts of interest
No potential conflict of interest relevant to this article was reported.
-
Funding
This work was supported by the 2024 Yeungnam University Research Grant (224A580029).
-
Data availability
Contact the corresponding author for data availability.
-
Acknowledgments
None.
-
Supplementary materials
None.
Article Information
Fig. 1.
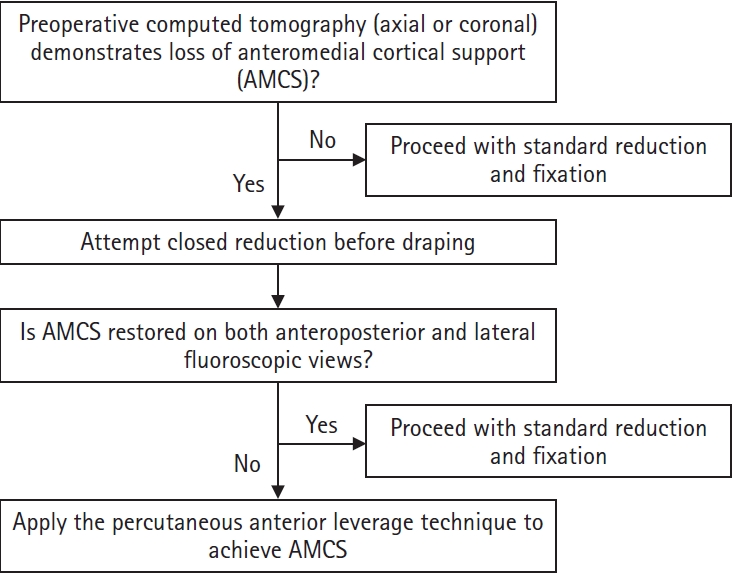
Clinical decision-making algorithm for applying the percutaneous anterior leverage technique.
Fig. 2.
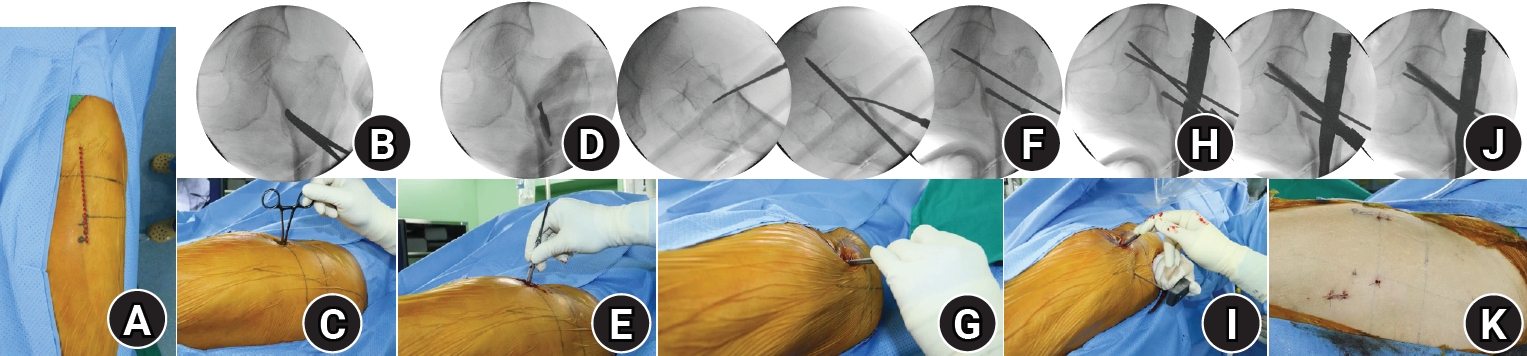
Intraoperative photographs and fluoroscopic images illustrating the percutaneous anterior leverage technique for achieving anteromedial cortical support (AMCS) in intertrochanteric femur fractures. (A) The red dotted line represents the lateral margin of the rectus femoris, corresponding to the Smith-Petersen interval used for the procedure; (B, C) A small incision is made along the Smith-Petersen interval, followed by blunt dissection with Kelley hemostatic forceps to reach the anteromedial cortex of the femur; (D, E) The forceps are replaced with a freer retractor, which is advanced to the fracture site at the anteromedial cortex; (F, G) The leverage maneuver, in which the freer retractor is used to elevate the intramedullary-displaced proximal anteromedial cortex into an extramedullary reduced position to achieve positive AMCS. This is followed by temporary fixation with a 3.2 mm Steinmann pin; (H, I) The freer retractor remains in place during intramedullary nailing without interfering with the procedure; (J) After blade insertion, compression is applied through the blade while the freer retractor is gradually withdrawn, ensuring final compression with complete positive AMCS; (K) Photograph showing the minimally invasive nature of this approach.
Fig. 3.

Radiographic, fluoroscopic, and computed tomography (CT) images from an 83-year-old female patient with a left femoral intertrochanteric fracture (AO/OTA classification A3). (A) Preoperative plain radiographs and CT showing a negative anteromedial cortical support (AMCS) state; (B) Intraoperative fluoroscopic images illustrating the percutaneous anterior leverage technique; (C) Comparative postoperative images from plain radiographs and CT showing that lateral plain radiographs alone do not clearly reveal the AMCS state. This CT shows positive AMCS in both the coronal and axial views; (D) Plain radiographs obtained 3 months postoperatively, showing bone union without complications.
Fig. 4.
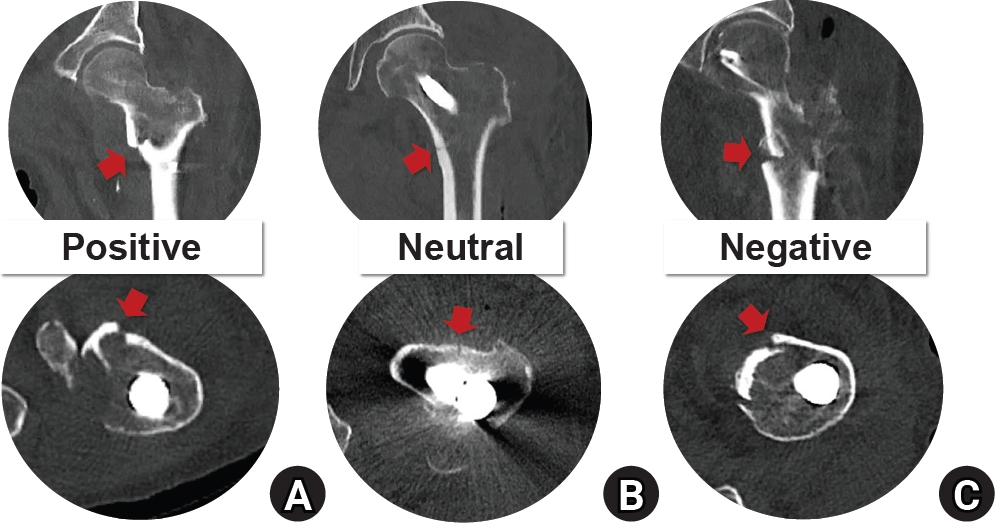
Computed tomography (CT) images of the anteromedial cortical support states in intertrochanteric femur fractures. The upper row shows coronal CT images illustrating medial cortical support, and the lower row shows axial CT images illustrating anterior cortical support. (A) Positive cortical support; (B) neutral cortical support; (C) negative cortical support. The red arrow indicates the anteromedial cortical state.
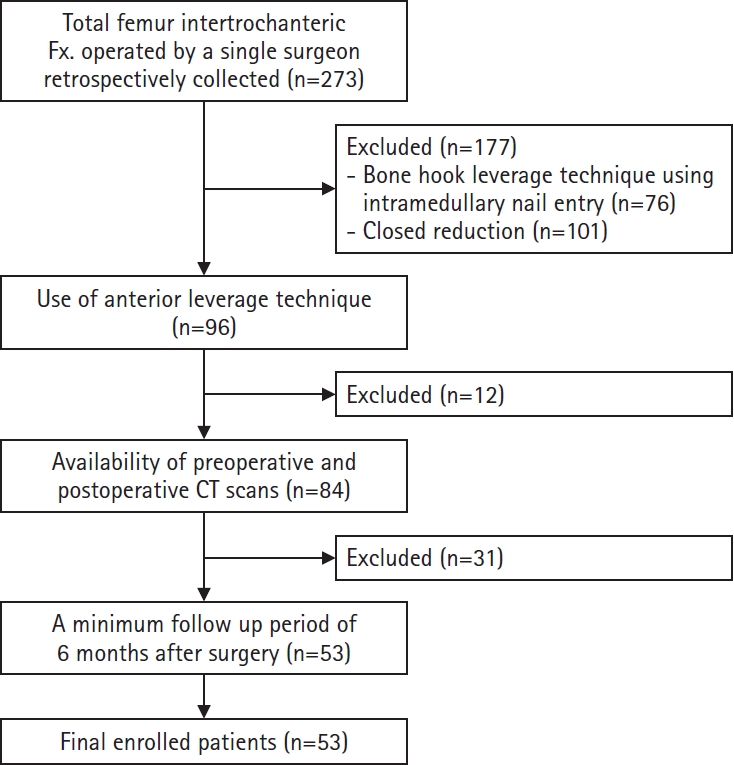
Fig. 6.
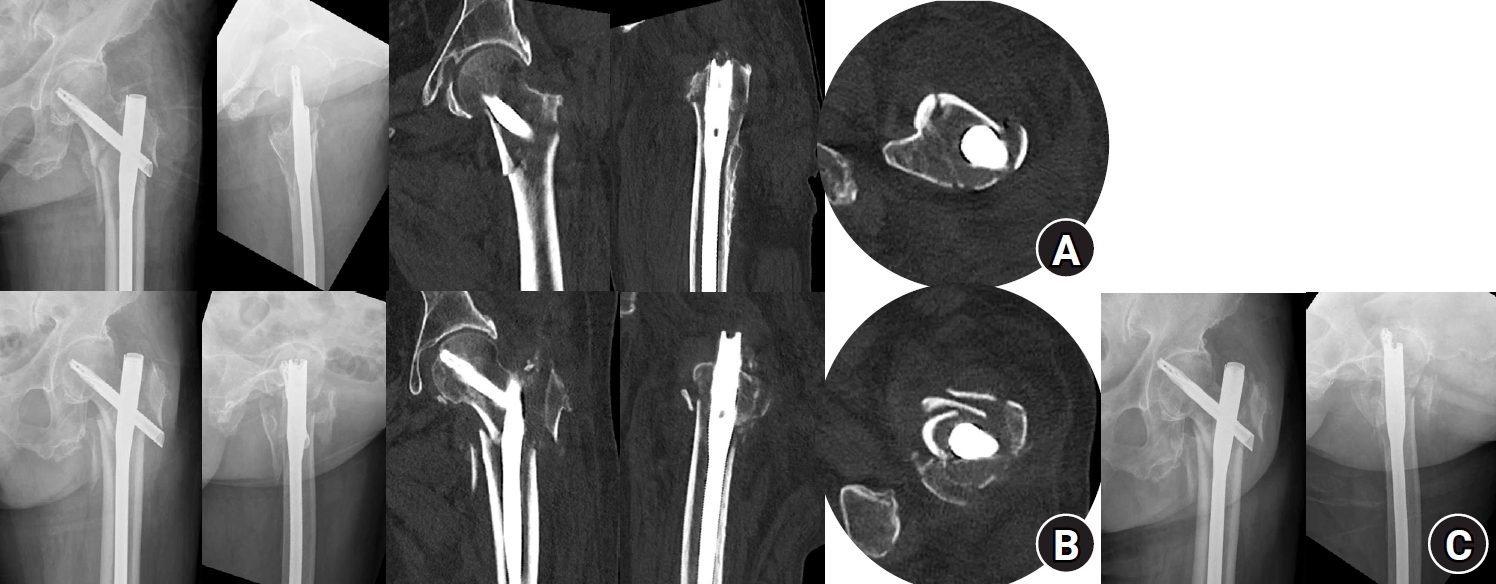
Radiographic images of an 82-year-old female patient with an AO/OTA intertrochanteric femur fracture classification of A3 treated with the percutaneous anterior leverage technique. (A) Postoperative radiographs showing positive medial cortical support and neutral anterior cortical support; (B) Radiographs taken 3 weeks postoperatively (at the first outpatient visit) showing conversion to negative anteromedial cortical support with cortical breakage; (C) Radiographs taken 7 weeks postoperatively showing blade cut-through.
Fig. 7.
Clinical algorithm providing practical guidance for the percutaneous anterior leverage technique.
Table 1.
Demographic and fracture characteristics of patients (n=53)
Table 2.
Preoperative and postoperative anterior and medial cortical support in patients with intertrochanteric femur fractures treated with the percutaneous anterior leverage technique
| Cortical support | Preoperative | Postoperative | P-value |
|---|---|---|---|
| Anterior | 0.026* | ||
| Positive | 3 (5.66) | 37 (69.81) | |
| Neutral | 4 (7.55) | 16 (30.19) | |
| Negative | 46 (86.79) | 0 (0.00) | |
| Medial | <0.001* | ||
| Positive | 5 (9.43) | 42 (79.25) | |
| Neutral | 9 (16.98) | 10 (18.87) | |
| Negative | 39 (73.58) | 1 (1.89) |
Table 3.
Clinical and radiographic characteristics of treatment failure patients
| Case | Age (yr) | Sex | AO/OTA classification | Dorr type | Preoperative anterior cortical support | Preoperative medial cortical support | Tip to apex distance (mm) | Blade position | Neck-shaft valgus angle (°) difference (postoperative-contralateral) | Operative time (min) | Postoperative anterior cortical support | Postoperative medial cortical support | Anteromedial cortical breakage during follow-up |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 8. Nonunion in the absence of varus collapse or blade cut-through | 81 | Male | A2 | B | Negative | Neutral | 9.2 | Inferior (AP)‒center (lateral) | 4a) | 33 | Positive | Positive | None |
| 20. Varus collapse | 88 | Female | A2 | B | Negative | Negative | 15.2 | Center (AP)‒center (lateral) | 0 | 50 | Neutral | Neutral | Occurred |
| 51. Blade cut-through | 80 | Female | A3 | C | Negative | Negative | 7.7 | Inferior (AP)‒center (lateral) | 7a) | 48 | Neutral | Positive | Occurred |
Table 4.
Subgroup analyses of postoperative anteromedial cortical support according to patient demographics and fracture characteristics
| Variable | Anterior cortical support | Medial cortical support | ||||||
|---|---|---|---|---|---|---|---|---|
| Positive (n=37) | Neutral (n=16) | Negative (n=0) | P-value | Positive (n=42) | Neutral (n=10) | Negative (n =1) | P-value | |
| Age (yr) | 83.0±6.6 | 77.6±11.0 | 0.030* | 81.2±9.1 | 81.8±5.9 | 83±0 | 0.847 | |
| Sex | 0.068 | 0.287 | ||||||
| Male (n=22) | 12 (54.55) | 10 (45.45) | 0 | 16 (72.73) | 6 (27.27) | 0 | ||
| Female (n=31) | 25 (80.65) | 6 (19.35) | 0 | 26 (83.87) | 4 (12.90) | 1 (1.89) | ||
| AO/OTA classification | 0.778 | 0.199 | ||||||
| A1 (n=24) | 18 (75.00) | 6 (25.00) | 0 | 21 (87.50) | 3 (12.50) | 0 | ||
| A2 (n=21) | 14 (66.67) | 7 (33.33) | 0 | 16 (76.19) | 5 (23.81) | 0 | ||
| A3 (n=8) | 5 (62.50) | 3 (37.50) | 0 | 5 (62.50) | 2 (25.00) | 1 (12.50) | ||
| Dorr type | 0.037* | 0.278 | ||||||
| A (n=16) | 7 (43.75) | 9 (56.25) | 0 | 11 (68.75) | 5 (31.25) | 0 | ||
| B (n=24) | 19 (79.17) | 5 (20.83) | 0 | 21 (87.50) | 3 (12.50) | 0 | ||
| C (n=13) | 11 (84.62) | 2 (15.38) | 0 | 10 (76.92) | 2 (15.38) | 1 (7.69) | ||
Table 5.
Comparisons between the treatment success and treatment failure groups in intertrochanteric femur fractures managed with the percutaneous anterior leverage technique
| Characteristic | Treatment success group (n=50) | Treatment failure group (n=3) | P-value | |
|---|---|---|---|---|
| Age (yr) | 81.3±8.4 | 83.0±4.4 | 0.732 | |
| Sex | Male | 21 (42) | 1 (33) | >0.999 |
| Female | 29 (58) | 2 (67) | ||
| AO/OTA classification | A1 | 24 (48) | 0 | 0.185 |
| A2 | 19 (38) | 2 (67) | ||
| A3 | 7 (14) | 1 (33) | ||
| Dorr type | A | 15 (30) | 1 (33) | 0.787 |
| B | 22 (44) | 2 (67) | ||
| C | 13 (26) | 0 | ||
| Tip to apex distance (mm) | 10.7±3.8 | 10.7±4.0 | 0.983 | |
| Blade position | Center (AP)‒center (lateral) | 11 (22) | 1 (33) | >0.999 |
| Inferior (AP)‒center (lateral) | 36 (72) | 2 (67) | ||
| Inferior (AP)‒posterior (lateral) | 3 (6) | 0 | ||
| Neck-shaft angle (°) difference (postoperative−contralateral) | 3.06±4.23 | 3.51±2.03 | 0.809 | |
| Anterior cortical support | Positive | 36 (72) | 1 (33) | 0.213 |
| Neutral | 14 (28) | 2 (67) | ||
| Negative | 0 | 0 | ||
| Medial cortical support | Positive | 40 (80) | 1 (33) | 0.510 |
| Neutral | 9 (18) | 2 (67) | ||
| Negative | 1 (2) | 0 (0) | ||
| Anteromedial cortical breakage during follow-up | Occurred | 0 | 2 (67) | 0.002* |
| None | 50 (100) | 1 (33) | ||
Table 6.
Univariate logistic regression analysis of factors associated with treatment failure
- 1. Kim SH, Jang SY, Cha Y, et al. The impact of hospital volume and region on mortality, medical costs, and length of hospital stay in elderly patients following hip fracture: a nationwide claims database analysis. Clin Orthop Surg 2025;17:80-90.ArticlePubMedPDF
- 2. Jang BW, Kim JW, Nho JH, et al. Hip fractures in centenarians: functional outcomes, mortality, and risk factors from a multicenter cohort study. Clin Orthop Surg 2023;15:910-6.ArticlePubMedPMCPDF
- 3. Lim EJ, Sakong S, Son WS, Cho JW, Oh JK, Kim CH. Comparison of sliding distance of lag screw and nonunion rate according to anteromedial cortical support in intertrochanteric fracture fixation: a systematic review and meta-analysis. Injury 2021;52:2787-94.ArticlePubMed
- 4. Mao W, Liu CD, Chang SM, Yang AL, Hong CC. Anteromedial cortical support in reduction of trochanteric hip fractures: from definition to application. J Bone Joint Surg Am 2024;106:1008-18.ArticlePubMed
- 5. Chang SM, Zhang YQ, Ma Z, Li Q, Dargel J, Eysel P. Fracture reduction with positive medial cortical support: a key element in stability reconstruction for the unstable pertrochanteric hip fractures. Arch Orthop Trauma Surg 2015;135:811-8.ArticlePubMedPMCPDF
- 6. Xie W, Shi L, Zhang C, et al. Anteromedial cortical support reduction of intertrochanteric fractures-A review. Injury 2024;55:111926.ArticlePubMed
- 7. Kim Y, Dheep K, Lee J, et al. Hook leverage technique for reduction of intertrochanteric fracture. Injury 2014;45:1006-10.ArticlePubMed
- 8. Kozono N, Ikemura S, Yamashita A, Harada T, Watanabe T, Shirasawa K. Direct reduction may need to be considered to avoid postoperative subtype P in patients with an unstable trochanteric fracture: a retrospective study using a multivariate analysis. Arch Orthop Trauma Surg 2014;134:1649-54.ArticlePubMedPDF
- 9. Cho WT, Cho JW, Yoon YC, Kim Y, Oh CW, Oh JK. Provisional pin fixation: an efficient alternative to manual maintenance of reduction in nailing of intertrochanteric fractures. Arch Orthop Trauma Surg 2016;136:55-63.ArticlePubMedPDF
- 10. Chen SY, Chang SM, Tuladhar R, et al. A new fluoroscopic view for evaluation of anteromedial cortex reduction quality during cephalomedullary nailing for intertrochanteric femur fractures: the 30° oblique tangential projection. BMC Musculoskelet Disord 2020;21:719.ArticlePubMedPMCPDF
- 11. Song H, Chang SM, Hu SJ, Du SC, Xiong WF. Calcar fracture gapping: a reliable predictor of anteromedial cortical support failure after cephalomedullary nailing for pertrochanteric femur fractures. BMC Musculoskelet Disord 2022;23:175.ArticlePubMedPMCPDF
- 12. Lee CH, Su KC, Chen KH, Pan CC, Wu YC. Impact of tip-apex distance and femoral head lag screw position on treatment outcomes of unstable intertrochanteric fractures using cephalomedullary nails. J Int Med Res 2018;46:2128-40.ArticlePubMedPMCPDF
- 13. Li SJ, Kristan A, Chang SM. Neutral medial cortical relation predicts a high loss rate of cortex support in pertrochanteric femur fractures treated by cephalomedullary nail. Injury 2021;52:3530-1.ArticlePubMed
References
Figure & Data
REFERENCES
Citations
Citations to this article as recorded by 
 ePub Link
ePub Link Cite
CitePercutaneous anterior leverage technique for anteromedial cortical support in intertrochanteric femur fractures: a computed tomography-based validation study
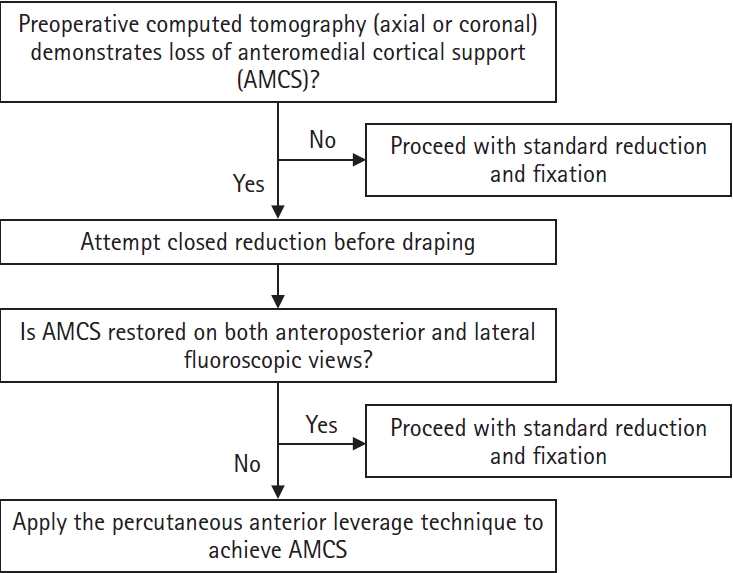
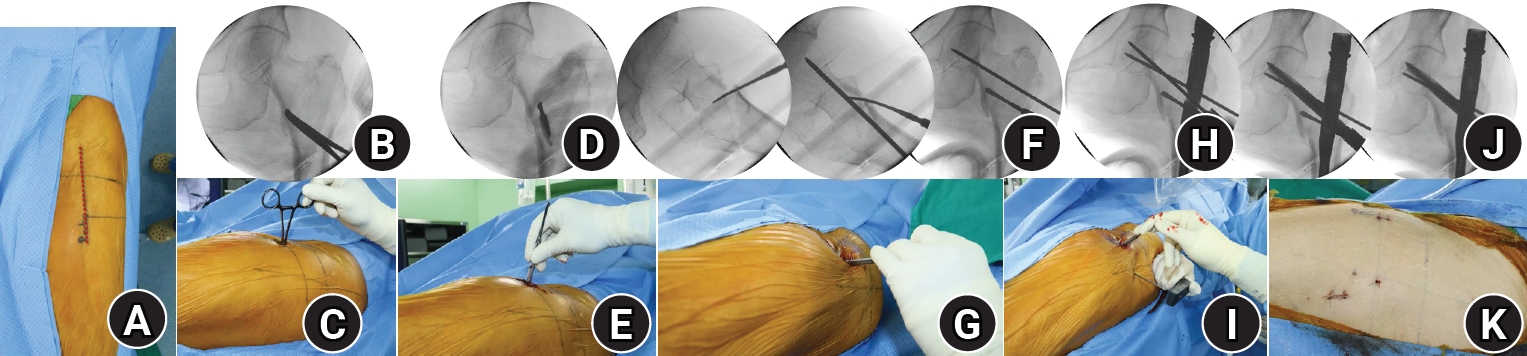

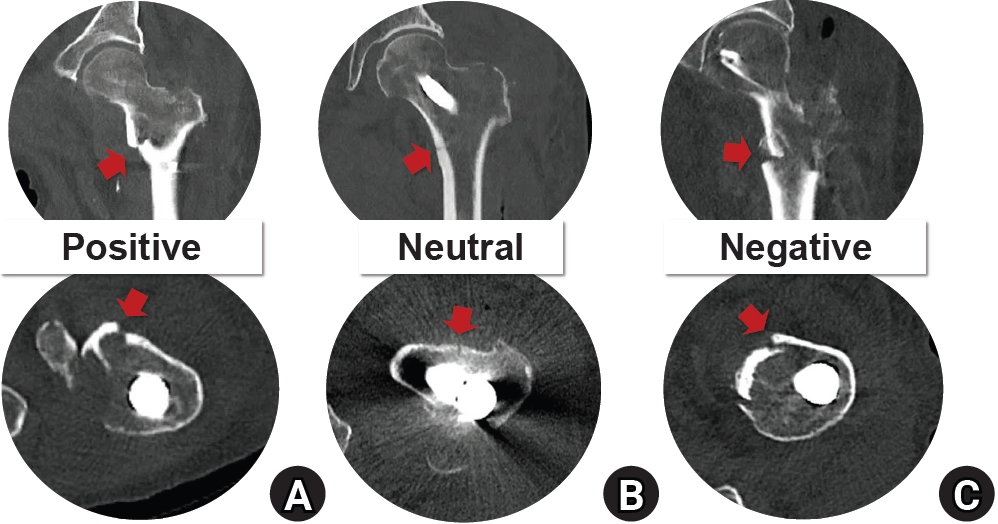
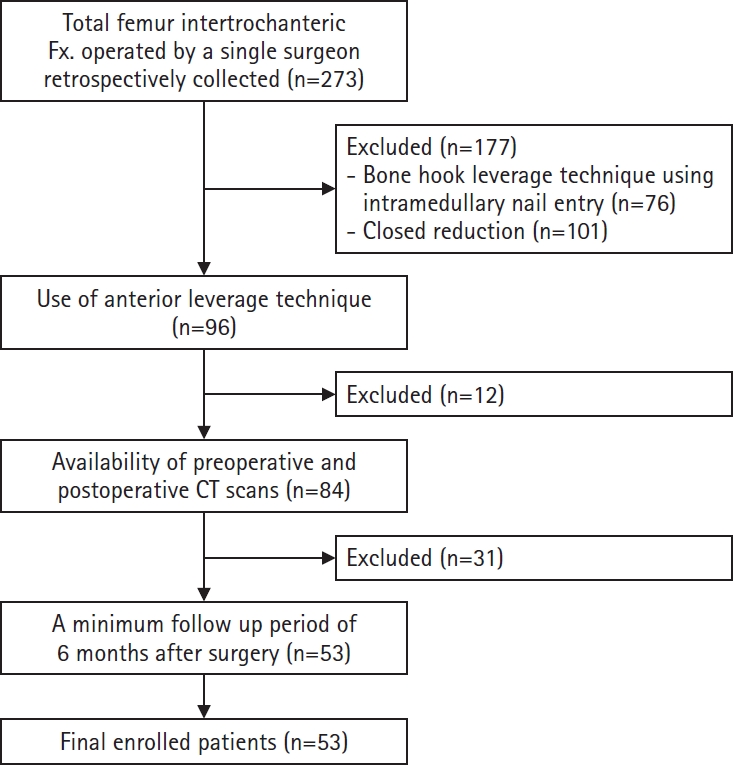
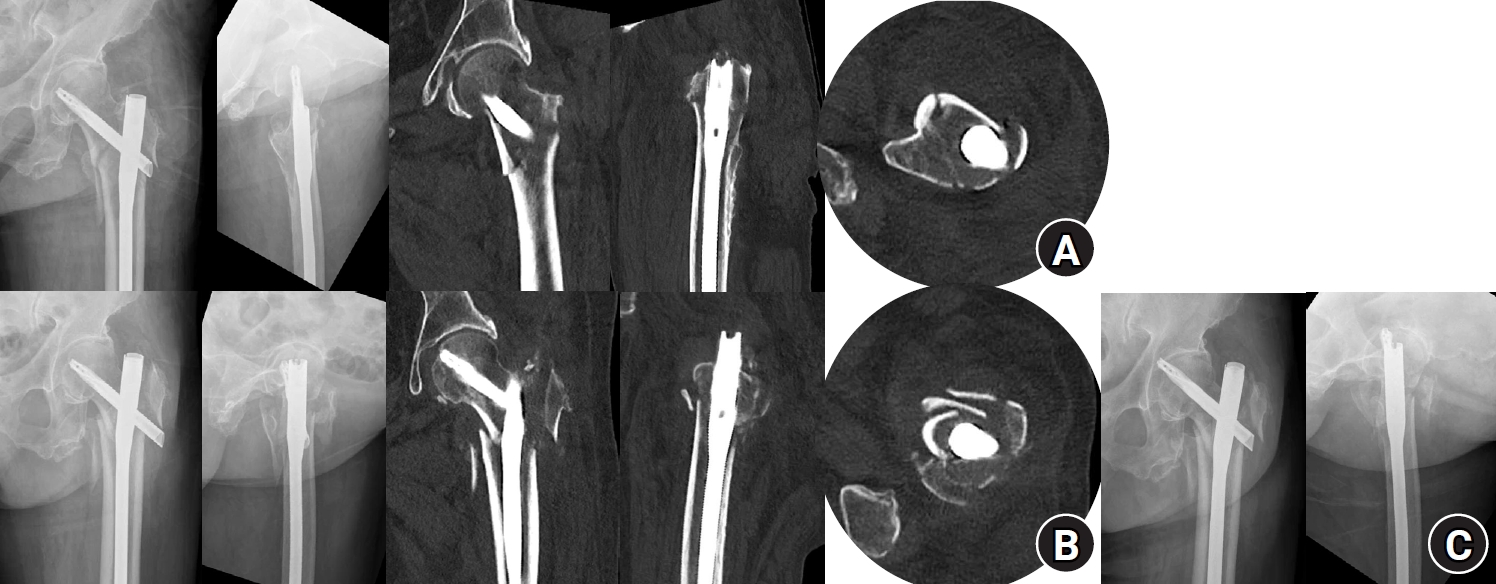
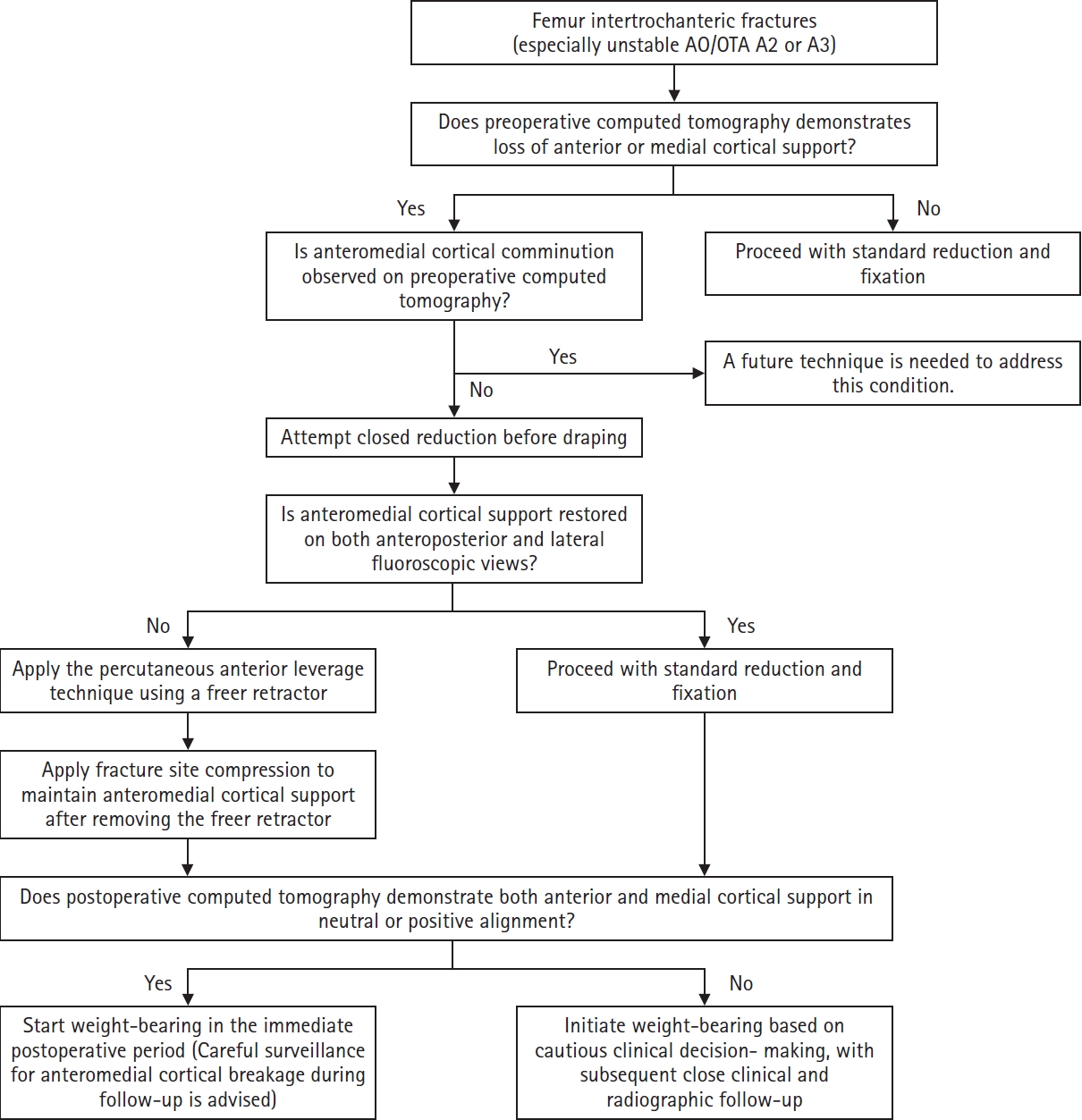
Fig. 1. Clinical decision-making algorithm for applying the percutaneous anterior leverage technique.
Fig. 2. Intraoperative photographs and fluoroscopic images illustrating the percutaneous anterior leverage technique for achieving anteromedial cortical support (AMCS) in intertrochanteric femur fractures. (A) The red dotted line represents the lateral margin of the rectus femoris, corresponding to the Smith-Petersen interval used for the procedure; (B, C) A small incision is made along the Smith-Petersen interval, followed by blunt dissection with Kelley hemostatic forceps to reach the anteromedial cortex of the femur; (D, E) The forceps are replaced with a freer retractor, which is advanced to the fracture site at the anteromedial cortex; (F, G) The leverage maneuver, in which the freer retractor is used to elevate the intramedullary-displaced proximal anteromedial cortex into an extramedullary reduced position to achieve positive AMCS. This is followed by temporary fixation with a 3.2 mm Steinmann pin; (H, I) The freer retractor remains in place during intramedullary nailing without interfering with the procedure; (J) After blade insertion, compression is applied through the blade while the freer retractor is gradually withdrawn, ensuring final compression with complete positive AMCS; (K) Photograph showing the minimally invasive nature of this approach.
Fig. 3. Radiographic, fluoroscopic, and computed tomography (CT) images from an 83-year-old female patient with a left femoral intertrochanteric fracture (AO/OTA classification A3). (A) Preoperative plain radiographs and CT showing a negative anteromedial cortical support (AMCS) state; (B) Intraoperative fluoroscopic images illustrating the percutaneous anterior leverage technique; (C) Comparative postoperative images from plain radiographs and CT showing that lateral plain radiographs alone do not clearly reveal the AMCS state. This CT shows positive AMCS in both the coronal and axial views; (D) Plain radiographs obtained 3 months postoperatively, showing bone union without complications.
Fig. 4. Computed tomography (CT) images of the anteromedial cortical support states in intertrochanteric femur fractures. The upper row shows coronal CT images illustrating medial cortical support, and the lower row shows axial CT images illustrating anterior cortical support. (A) Positive cortical support; (B) neutral cortical support; (C) negative cortical support. The red arrow indicates the anteromedial cortical state.
Fig. 5. Flowchart illustrating the patient selection process. Fx, fracture; CT, computed tomography.
Fig. 6. Radiographic images of an 82-year-old female patient with an AO/OTA intertrochanteric femur fracture classification of A3 treated with the percutaneous anterior leverage technique. (A) Postoperative radiographs showing positive medial cortical support and neutral anterior cortical support; (B) Radiographs taken 3 weeks postoperatively (at the first outpatient visit) showing conversion to negative anteromedial cortical support with cortical breakage; (C) Radiographs taken 7 weeks postoperatively showing blade cut-through.
Fig. 7. Clinical algorithm providing practical guidance for the percutaneous anterior leverage technique.
Fig. 1.
Fig. 2.
Fig. 3.
Fig. 4.
Fig. 5.
Fig. 6.
Fig. 7.
Percutaneous anterior leverage technique for anteromedial cortical support in intertrochanteric femur fractures: a computed tomography-based validation study
| Characteristic | Value |
|---|---|
| Age (yr) | 81.36±8.43 |
| Sex (male:female) | 22:31 |
| AO/OTA classification | |
| A1 | 24 (45.28) |
| A2 | 21 (39.62) |
| A3 | 8 (15.09) |
| Dorr type | |
| A | 16 (30.19) |
| B | 24 (45.28) |
| C | 13 (24.53) |
| Preoperative anterior cortical support | |
| Positive | 3 (5.66) |
| Neutral | 4 (7.55) |
| Negative | 46 (86.79) |
| Preoperative medial cortical support | |
| Positive | 5 (9.43) |
| Neutral | 9 (16.98) |
| Negative | 39 (73.58) |
| Tip to apex distance (mm) | 10.75±3.77 |
| Blade position | |
| Center (anteroposterior)‒center (lateral) | 12 (22.64) |
| Inferior (anteroposterior)‒center (lateral) | 38 (71.70) |
| Inferior (anteroposterior)‒posterior (lateral) | 3 (5.66) |
| Neck-shaft valgus angle difference (postoperative−contralateral) (°) | 3.09±4.16 |
| Operative time (min) | 34.15±10.21 |
| Follow-up (mo) | 8.79±4.35 |
| Cortical support | Preoperative | Postoperative | P-value |
|---|---|---|---|
| Anterior | 0.026 |
||
| Positive | 3 (5.66) | 37 (69.81) | |
| Neutral | 4 (7.55) | 16 (30.19) | |
| Negative | 46 (86.79) | 0 (0.00) | |
| Medial | <0.001 |
||
| Positive | 5 (9.43) | 42 (79.25) | |
| Neutral | 9 (16.98) | 10 (18.87) | |
| Negative | 39 (73.58) | 1 (1.89) |
| Case | Age (yr) | Sex | AO/OTA classification | Dorr type | Preoperative anterior cortical support | Preoperative medial cortical support | Tip to apex distance (mm) | Blade position | Neck-shaft valgus angle (°) difference (postoperative-contralateral) | Operative time (min) | Postoperative anterior cortical support | Postoperative medial cortical support | Anteromedial cortical breakage during follow-up |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 8. Nonunion in the absence of varus collapse or blade cut-through | 81 | Male | A2 | B | Negative | Neutral | 9.2 | Inferior (AP)‒center (lateral) | 4 |
33 | Positive | Positive | None |
| 20. Varus collapse | 88 | Female | A2 | B | Negative | Negative | 15.2 | Center (AP)‒center (lateral) | 0 | 50 | Neutral | Neutral | Occurred |
| 51. Blade cut-through | 80 | Female | A3 | C | Negative | Negative | 7.7 | Inferior (AP)‒center (lateral) | 7 |
48 | Neutral | Positive | Occurred |
| Variable | Anterior cortical support | Medial cortical support | ||||||
|---|---|---|---|---|---|---|---|---|
| Positive (n=37) | Neutral (n=16) | Negative (n=0) | P-value | Positive (n=42) | Neutral (n=10) | Negative (n =1) | P-value | |
| Age (yr) | 83.0±6.6 | 77.6±11.0 | 0.030 |
81.2±9.1 | 81.8±5.9 | 83±0 | 0.847 | |
| Sex | 0.068 | 0.287 | ||||||
| Male (n=22) | 12 (54.55) | 10 (45.45) | 0 | 16 (72.73) | 6 (27.27) | 0 | ||
| Female (n=31) | 25 (80.65) | 6 (19.35) | 0 | 26 (83.87) | 4 (12.90) | 1 (1.89) | ||
| AO/OTA classification | 0.778 | 0.199 | ||||||
| A1 (n=24) | 18 (75.00) | 6 (25.00) | 0 | 21 (87.50) | 3 (12.50) | 0 | ||
| A2 (n=21) | 14 (66.67) | 7 (33.33) | 0 | 16 (76.19) | 5 (23.81) | 0 | ||
| A3 (n=8) | 5 (62.50) | 3 (37.50) | 0 | 5 (62.50) | 2 (25.00) | 1 (12.50) | ||
| Dorr type | 0.037 |
0.278 | ||||||
| A (n=16) | 7 (43.75) | 9 (56.25) | 0 | 11 (68.75) | 5 (31.25) | 0 | ||
| B (n=24) | 19 (79.17) | 5 (20.83) | 0 | 21 (87.50) | 3 (12.50) | 0 | ||
| C (n=13) | 11 (84.62) | 2 (15.38) | 0 | 10 (76.92) | 2 (15.38) | 1 (7.69) | ||
| Characteristic | Treatment success group (n=50) | Treatment failure group (n=3) | P-value | |
|---|---|---|---|---|
| Age (yr) | 81.3±8.4 | 83.0±4.4 | 0.732 | |
| Sex | Male | 21 (42) | 1 (33) | >0.999 |
| Female | 29 (58) | 2 (67) | ||
| AO/OTA classification | A1 | 24 (48) | 0 | 0.185 |
| A2 | 19 (38) | 2 (67) | ||
| A3 | 7 (14) | 1 (33) | ||
| Dorr type | A | 15 (30) | 1 (33) | 0.787 |
| B | 22 (44) | 2 (67) | ||
| C | 13 (26) | 0 | ||
| Tip to apex distance (mm) | 10.7±3.8 | 10.7±4.0 | 0.983 | |
| Blade position | Center (AP)‒center (lateral) | 11 (22) | 1 (33) | >0.999 |
| Inferior (AP)‒center (lateral) | 36 (72) | 2 (67) | ||
| Inferior (AP)‒posterior (lateral) | 3 (6) | 0 | ||
| Neck-shaft angle (°) difference (postoperative−contralateral) | 3.06±4.23 | 3.51±2.03 | 0.809 | |
| Anterior cortical support | Positive | 36 (72) | 1 (33) | 0.213 |
| Neutral | 14 (28) | 2 (67) | ||
| Negative | 0 | 0 | ||
| Medial cortical support | Positive | 40 (80) | 1 (33) | 0.510 |
| Neutral | 9 (18) | 2 (67) | ||
| Negative | 1 (2) | 0 (0) | ||
| Anteromedial cortical breakage during follow-up | Occurred | 0 | 2 (67) | 0.002 |
| None | 50 (100) | 1 (33) | ||
| Characteristic | OR | 95% CI | P-value | |
|---|---|---|---|---|
| Age | 1.028 | 0.881–1.200 | 0.726 | |
| Sex | Male | 1 | - | - |
| Female | 1.448 | 0.123–17.041 | 0.768 | |
| AO/OTA classification | A1 | 1 | - | - |
| A2 | 170,049,980.6 | 0.000–0.000 | 0.998 | |
| A3 | 230,782,116.5 | 0.000–0.000 | 0.998 | |
| Dorr type | A | 1 | - | - |
| B | 1.364 | 0.113–16.423 | 0.807 | |
| C | 0.000 | 0.000–0.000 | 0.999 | |
| Tip to apex distance | 0.997 | 0.729–1.363 | 0.983 | |
| Blade position | Center (AP)‒center (lateral) | 1 | - | |
| Inferior (AP)‒center (lateral) | 0.611 | 0.050–7.397 | 0.699 | |
| Inferior (AP)‒posterior (lateral) | 0.000 | 0.000–0.000 | 0.999 | |
| Neck-shaft angle difference (postoperative−contralateral) | 1.034 | 0.795–1.345 | 0.805 | |
| Anterior cortical support | Positive | 1 | - | - |
| Neutral | 5.143 | 0.431–61.324 | 0.195 | |
| Medial cortical support | Positive | 1 | - | - |
| Neutral | 2.222 | 0.181–27.262 | 0.532 | |
| Negative | 0.000 | 0.000–0.000 | >0.999 | |
| Anteromedial cortical breakage during follow-up | Occurred | 1 | - | - |
| None | 80,773,742,143 | 0.000–0.000 | 0.999 | |
Table 1. Demographic and fracture characteristics of patients (n=53)
Values are presented as mean±standard deviation or number (%).
Table 2. Preoperative and postoperative anterior and medial cortical support in patients with intertrochanteric femur fractures treated with the percutaneous anterior leverage technique
Values are presented as number (%). P<0.05
Table 3. Clinical and radiographic characteristics of treatment failure patients
AP, anteroposterior. Positive values indicate valgus alignment compared with the contralateral hip, and negative values indicate varus alignment.
Table 4. Subgroup analyses of postoperative anteromedial cortical support according to patient demographics and fracture characteristics
Values are presented as mean±standard deviation or number (%). P<0.05.
Table 5. Comparisons between the treatment success and treatment failure groups in intertrochanteric femur fractures managed with the percutaneous anterior leverage technique
Values are presented as mean±standard deviation or number (%). AP, anteroposterior. P<0.05.
Table 6. Univariate logistic regression analysis of factors associated with treatment failure
OR, odds ratio; CI, confidence interval; AP, anteroposterior. P<0.05.

