 E-submission
E-submission TOTA
TOTA TOTS
TOTS
Search
- Page Path
- HOME > Search
Original Articles
- Clinical and radiographic outcomes of hemiarthroplasty for proximal humeral fractures in Korea with three or more years of follow-up: a retrospective cohort study
- Sang Jin Cheon, Kyu-Hak Jung, Min Hyeok Choi, Suk-Woong Kang
- J Musculoskelet Trauma 2026;39(2):147-155. Published online February 26, 2026
- DOI: https://doi.org/10.12671/jmt.2025.00325

-
 Abstract
Abstract
 PDF
PDF - Background
Shoulder hemiarthroplasty (HA) is an established treatment option for complex proximal humeral fractures, particularly in cases involving severe comminution or osteoporotic bone. This study investigated the clinical and radiographic outcomes of HA with a minimum follow-up of 3 years and aimed to identify prognostic factors associated with postoperative function.
Methods
We retrospectively reviewed 44 patients (16 males and 28 females; mean age, 61.2 years; range, 23–83 years) who underwent shoulder HA for complex proximal humeral fractures between 2005 and 2018. The mean follow-up duration was 70.4 months (range, 36–168 months). Clinical evaluations included the Constant score, visual analog scale pain score, patient satisfaction, and range of motion. Radiographic assessments examined tuberosity healing, radiolucent lines, acromiohumeral distance (AHD), and glenoid arthrosis.
Results
At the 3-year follow-up, 64% of patients reported being satisfied or very satisfied. The mean Constant score was 46.6 (range, 13–71), and the age- and sex-adjusted Constant score was 53.5 (range, 19–92). Radiographically, 23% of patients demonstrated radiolucent lines, and 41% showed evidence of glenoid arthrosis. Tuberosity absorption occurred in 39% of patients, with a mean onset of 11.2 months postoperatively, and was significantly associated with lower Constant scores and reduced range of motion. Patients younger than 60 years demonstrated better functional outcomes and lower rates of tuberosity absorption. The mean AHD decreased from 8.4 mm postoperatively to 4.4 mm at the 3-year follow-up (P<0.001).
Conclusions
Shoulder HA for complex proximal humeral fractures yielded satisfactory pain relief and functional outcomes, particularly when tuberosity healing was preserved. However, elderly patients with diminished bone quality were more likely to develop tuberosity absorption and experience poorer functional recovery. Meticulous surgical technique and careful postoperative surveillance remain essential to achieving optimal results. Level of evidence: III.
- 900 View
- 24 Download

- Surgical outcomes of the coracoid process fracture associated with the acromioclavicular joint injury in Korea: a case series
- Dongju Shin, Sung Choi, Sangwoo Kim, Byung Hoon Kwack
- J Musculoskelet Trauma 2026;39(1):54-61. Published online January 14, 2026
- DOI: https://doi.org/10.12671/jmt.2025.00346
-
Abstract
PDF
- Background
Excluding technical reports and isolated case reports, there are no published studies evaluating coracoid process fixation with or without an acromioclavicular joint (ACJ) stabilization procedure for coracoid process fractures associated with ACJ injury. The purpose of this study was to assess the surgical outcomes of coracoid process fractures associated with ACJ injuries and to determine the usefulness of coracoid process fixation with or without an ACJ stabilization procedure.
Methods
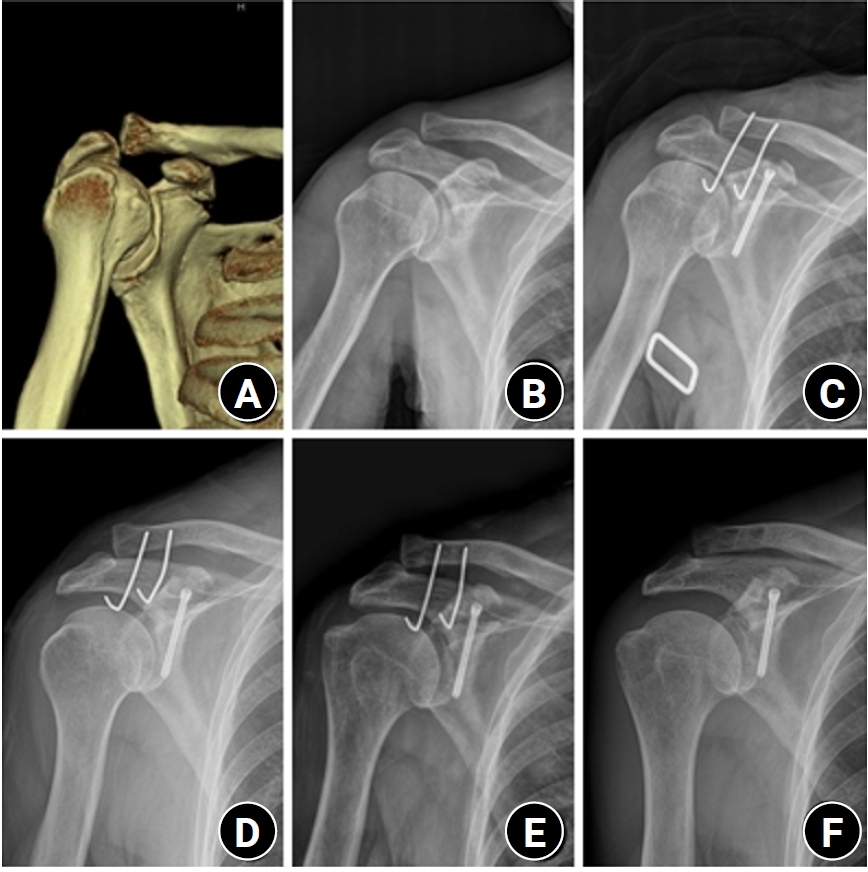
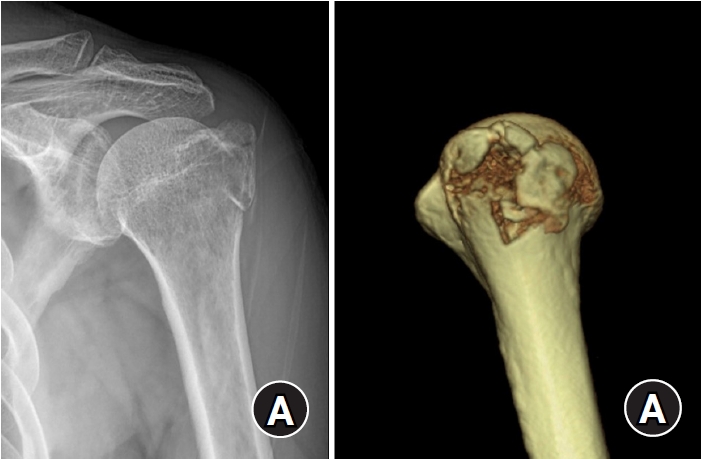
From February 2006 to December 2015, patients with coracoid process fractures associated with ACJ injuries were enrolled. Radiological and clinical outcomes were analyzed in 12 patients who underwent coracoid process fixation with or without an ACJ stabilization procedure. A 3.5-mm cannulated screw with a washer or a 3.0-mm headless compression screw was used for coracoid process fixation, and either a clavicle hook plate or Kirschner (K)-wires were used for ACJ injuries when additional fixation was necessary.
Results
Bone union was achieved in 11 patients (91.7%), while one case was determined to be a nonunion at 6 months. Radiological union occurred at an average of 3 months (range, 1.5–4 months) in all patients except the nonunion case. At the final follow-up, the average clinical scores were a visual analogue scale (VAS) pain score of 1.5 (range, 0–4) and a UCLA score of 30.9 (range, 28–35). Clinical outcomes were satisfactory in all patients, including the patient with nonunion.
Conclusion
The clinical and radiological outcomes of treating coracoid process fractures associated with ACJ injuries using coracoid process fixation with or without ACJ stabilization were favorable. A cannulated screw with a washer and clavicle hook plate fixation may provide sufficient stability for both the coracoid process fracture and the ACJ injury when feasible. Level of evidence: IV.
- 1,234 View
- 31 Download
- Outcomes of open reduction and internal fixation using 2.0/2.4 mm locking compression plate in isolated greater tuberosity fractures of humerus
- Sung Choi, Dongju Shin, Sangwoo Kim, Byung Hoon Kwack
- J Musculoskelet Trauma 2025;38(1):32-39. Published online January 24, 2025
- DOI: https://doi.org/10.12671/jmt.2025.00005
-
Abstract
PDF
- Background
The purpose of this study was to retrospectively evaluate the radiographic and clinical results of a small single or double low-profile plate fixation of 2.0/2.4 mm locking compression plate (LCP) in treating isolated greater tuberosity (GT) fractures of the humerus. Methods: From June 2015 to October 2022, patients who underwent LCP in treating isolated GT fractures of the humerus were included in this study. The radiological and clinical results were analyzed in 15 patients who underwent open reduction and internal fixation used 2.0/2.4 mm LCP. Results: Bone union was achieved in 14 patients (93.3%) and one failed case was treated with a 2.4 mm single LCP fixation. Radiological union was achieved within 10–20 weeks. Complications occurred in two patients (13.3%), including the reduction failure and shoulder stiffness. At the final follow-up, the average clinical scores were as follows: a visual analog scale for pain of 2.1 (range, 0–5) and a University of California, Los Angeles score of 27.2 (range, 18–31). Regarding range of motion (ROM), the average active ROMs were 142° for forward flexion (range, 120°–150°), 147.1° for abduction (range, 120°– 180°), and 59.3° for external rotation (range, 45°–80°). For internal rotation, the average was observed to reach the 10th thoracic vertebra (range, 1st lumbar vertebra–7th thoracic vertebra). Conclusions: The clinical and radiologic outcomes of treating isolated GT fracture using 2.0/2.4 mm LCP were favorable, and double low-profile plate fixation may be beneficial for sufficient fracture stability if possible. Level of evidence: Level IV, case series.
- 3,570 View
- 76 Download
 First
First Prev
Prev

