 E-submission
E-submission TOTA
TOTA TOTS
TOTS
Search
- Page Path
- HOME > Search
Original Articles
- Relationship of lateral malleolar fracture patterns to posterior malleolar fracture morphology in supination-external rotation ankle fractures in Korea: a retrospective cohort study
- Jong-Eun Kim, Chan-Jin Park, Jun-Young Lee, Keun-Bae Lee, Gun-Woo Lee
- J Musculoskelet Trauma 2025;38(4):212-220. Published online October 24, 2025
- DOI: https://doi.org/10.12671/jmt.2025.00234
-
 Abstract
Abstract
 PDF
PDF - Background
Posterior malleolar fractures frequently accompany rotational ankle fractures. However, the morphological relationship between lateral and posterior malleolar fractures in supination-external rotation (SER) ankle fractures remains unclear. This study aimed to classify lateral malleolar fracture patterns in SER type 3 and 4 ankle fractures and investigated their associations with posterior malleolar fracture morphology.
Methods
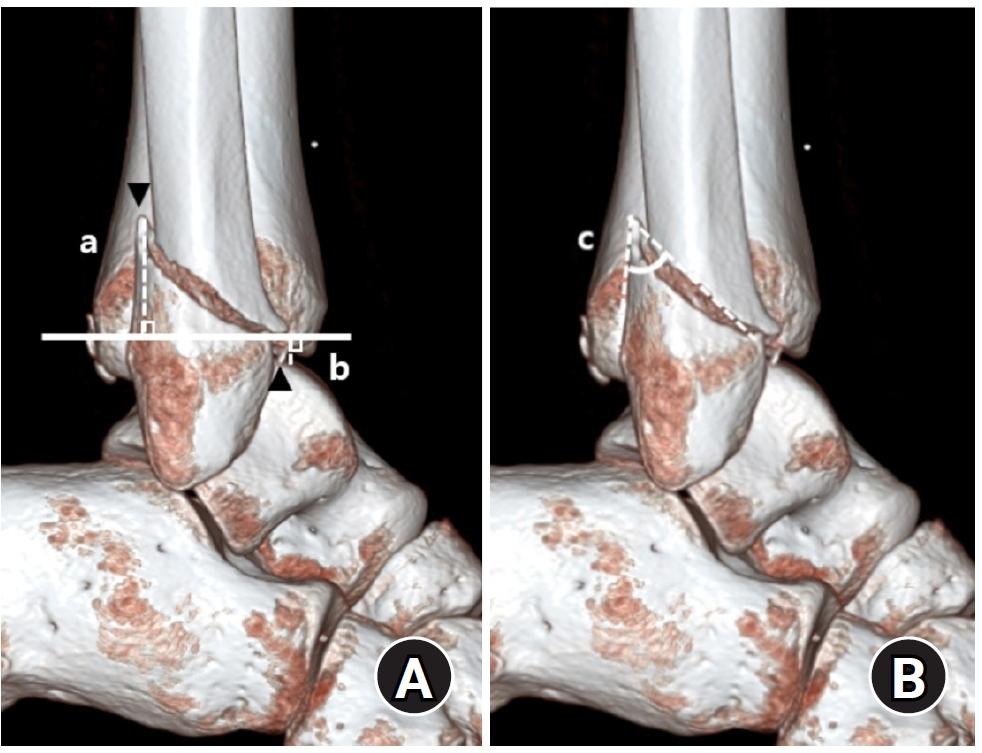
We retrospectively reviewed 132 patients with SER type 3 or 4 ankle fractures and concurrent posterior malleolar fractures between January 2016 and December 2021. Lateral malleolar fractures were categorized as fibular fractures extending <4.5 cm proximal to the ankle joint (102 ankles) or fibular fractures extending ≥4.5 cm proximal to the ankle joint (30 ankles) based on posterior cortex height measured using three-dimensional computed tomography (3D-CT). Posterior malleolar fracture morphology was assessed using the Haraguchi and Bartonicek classifications. Quantitative parameters—including fracture height, angle, and articular involvement—were analyzed using 3D-CT imaging.
Results
Fibular fractures extending ≥4.5 cm proximal to the ankle joint were associated with a significantly higher frequency of Haraguchi type II and Bartonicek types 3 and 4 posterior malleolar fractures. This group also exhibited greater articular involvement (19.2% vs. 12.0%) and posterior cortical height (55.4 mm vs. 24.8 mm) compared to the <4.5 cm group (all P<0.001).
Conclusions
In SER type 3 and 4 ankle fractures, a fibular fracture extending ≥4.5 cm proximal to the ankle joint may be associated with posterior malleolar fractures exhibiting greater articular involvement and medial extension. Preoperative evaluation of the lateral malleolar fracture pattern may provide useful insights into posterior malleolar morphology and assist in surgical planning. However, these findings should be interpreted with caution due to inherent study limitations. Level of evidence: IV
- 1,952 View
- 40 Download

- Prediction of Syndesmotic Instability according to the Lateral Malleolus Fracture Pattern in Supination-External Rotation Type Ankle Fractures: Short Oblique versus Long Oblique Fracture
- Chan-Jin Park, Min-Su Lee, Keun-Bae Lee
- J Korean Fract Soc 2024;37(1):39-45. Published online January 31, 2024
- DOI: https://doi.org/10.12671/jkfs.2024.37.1.39
-
Abstract
PDF
- Purpose
This study examined whether preoperative radiological evaluations can predict syndesmotic instability according to the lateral malleolus fracture pattern in supination-external rotation-type ankle fractures.
Materials and Methods
This study enrolled 132 patients (132 ankles) with supination-external rotation stage 3 and 4 ankle fractures. Three-dimensional computed tomography was used for the morphological classification of the lateral malleolus fractures. A long oblique fracture was defined when the posterior cortical bone height of the fracture was 4.5 cm or more from the plafond of the distal tibial articular surface. A short oblique fracture was defined when the height was less than 4.5 cm. The demographic characteristics and syndesmotic instability of the two groups were evaluated.
Results
Short oblique fractures were confirmed in 102 cases, and long oblique fractures were confirmed in 30 cases. Long oblique fractures occurred at a statistically significantly higher incidence in younger ages and among males compared to short oblique fractures. Syndesmotic instability was more common in long oblique fractures.
Conclusion
In supination-external rotation-type ankle fractures, syndesmotic instability was observed in approximately 13%. Specifically, when the fracture pattern of the lateral malleolus is long oblique, the incidence of syndesmotic instability is approximately three times higher than in short oblique fractures. Therefore, meticulous evaluations of the lateral malleolus fracture pattern and establishing an appropriate treatment plan before surgery are crucial. -
Citations
Citations to this article as recorded by
- Relationship of lateral malleolar fracture patterns to posterior malleolar fracture morphology in supination-external rotation ankle fractures in Korea: a retrospective cohort stduy
Jong-Eun Kim, Chan-Jin Park, Jun-Young Lee, Keun-Bae Lee, Gun-Woo Lee
Journal of Musculoskeletal Trauma.2025; 38(4): 212. CrossRef
- Relationship of lateral malleolar fracture patterns to posterior malleolar fracture morphology in supination-external rotation ankle fractures in Korea: a retrospective cohort stduy
- 1,198 View
- 14 Download
- 1 Crossref
- Comparison of the Size of the Posterior Malleolar Fragment in Trimalleolar Ankle Fractures Measured Using Lateral Plain Radiography and Three-Dimensional Computed Tomography
- Gun-Woo Lee, Dong-Min Jung, Woo Kyoung Kwak, Keun-Bae Lee
- J Korean Fract Soc 2022;35(3):91-96. Published online July 31, 2022
- DOI: https://doi.org/10.12671/jkfs.2022.35.3.91
-
Abstract
PDF
- Purpose
This study aimed to evaluate and compare the accuracy of the size of the posterior malleolar fragment measured using lateral plain radiography and three-dimensional computed tomography (3DCT) in patients with ankle trimalleolar fractures.
Materials and Methods
This study enrolled 80 patients (80 ankles) with ankle trimalleolar fractures and analyzed the size of the posterior malleolar fragments using plain radiography and 3D-CT. The articular involvement of the posterior malleolar fragments was measured as a percentage of the articular surface in the sagittal length of the tibial plafond using lateral plain radiography, and the articular surface area was directly measured using 3D-CT. In addition, we classified the patients into three groups based on the morphology of the posterior malleolar fracture, according to the Haraguchi classification method, and evaluated and compared the accuracy of the size of the posterior malleolar fragments.
Results
The mean articular involvement of the posterior malleolar fragments on plain radiography was 27.6% (range, 6.0%-53.1%), which was significantly higher than the mean of 21.9% (range, 4.7%-47.1%) measured using 3D-CT (p=0.004). In the analysis, according to the fracture morphology, the mean difference between the two methods was the largest for type I fractures at 9.1% (range, 1.8%-19.5%) and the smallest for type II fractures at 1.1% (range, –7.7% to 8.8%).
Conclusion
The articular involvement of posterior malleolar fragments measured using plain radiography showed low accuracy and significantly higher values than the actual articular involvement. Therefore, careful evaluation using 3D-CT is crucial for accurate analysis and optimal treatment in patients with ankle trimalleolar fractures. -
Citations
Citations to this article as recorded by- Relationship of lateral malleolar fracture patterns to posterior malleolar fracture morphology in supination-external rotation ankle fractures in Korea: a retrospective cohort stduy
Jong-Eun Kim, Chan-Jin Park, Jun-Young Lee, Keun-Bae Lee, Gun-Woo Lee
Journal of Musculoskeletal Trauma.2025; 38(4): 212. CrossRef
- Relationship of lateral malleolar fracture patterns to posterior malleolar fracture morphology in supination-external rotation ankle fractures in Korea: a retrospective cohort stduy
- 937 View
- 10 Download
- 1 Crossref
Review Article
- Current Management of Talar Fractures
- Gun-Woo Lee, Keun-Bae Lee
- J Korean Fract Soc 2022;35(1):31-37. Published online January 31, 2022
- DOI: https://doi.org/10.12671/jkfs.2022.35.1.31
-
Abstract
PDF
- Talar fracture management is one of the most challenging tasks for orthopedic surgeons. High complication rates and functional impairments after talar fractures have been well documented, and thus, surgical strategies capable of perfect anatomic reduction and stable fixation are important. The current review was undertaken to provide recommendations regarding updated surgical strategies that include surgical timing, approach, fixation methods, and the prevention and treatment of possible complications.
- 1,115 View
- 9 Download
Original Article
- Comparing Outcomes of Screw Fixation and Non-Fixation for Small-Sized Posterior Malleolar Fragment in Ankle Trimalleolar Fractures
- Jee-Wook Ko, Gun-Woo Lee, Keun-Bae Lee
- J Korean Fract Soc 2021;34(1):8-15. Published online January 31, 2021
- DOI: https://doi.org/10.12671/jkfs.2021.34.1.8
-
Abstract
PDF
- Purpose
This study was undertaken to compare outcomes of screw fixation and non-fixation of a small-sized posterior malleolar fragment involving less than 25% articular surface in ankle trimalleolar fractures. Materials and Methods: A total of 32 consecutive ankles (32 patients), with posterior malleolar fragment involving 15%-25% of the joint surface, were enrolled in the study. Patients were divided into 2 groups according to whether the fragment was fixed or not (fixed: 20 ankles, non-fixed: 12 ankles). The minimum follow-up period was 12 months. Median size of the posterior malleolar fragment in the fixed and non-fixed groups were 24.6% (range, 22.3%-25.0%) and 22.1% (range, 17.4%-24.3%), respectively. Complications as well as clinical and radiographic outcomes were compared and analyzed between the two groups. Results: Clinical outcomes, including American Orthopaedic Foot & Ankle Society (p=0.501), visual analogue scale (p=0.578), and ankle range of motion (p=0.552), showed no difference between groups at the final follow-up. No differences were obtained in the radiographic outcomes, including joint stepoff (p=0.289) and fragment gap (p=0.289). Complications, including 1 case of delayed union and 1 case of wound infection, were reported in the fixed group. Conclusion: Clinical outcomes and radiographic outcomes of the non-fixation group were satisfactory and comparable to the fixation group. Our results indicate that anatomical reduction with small-sized posterior malleolar fragment in ankle trimalleolar fractures is sufficient for satisfactory outcomes, without the need for additional internal fixation.
- 1,217 View
- 13 Download
 First
First Prev
Prev

