 E-submission
E-submission TOTA
TOTA TOTS
TOTS
Search
- Page Path
- HOME > Search
Case Report
- Fixation with two headless compression screws and a distal-radius bone graft for proximal scaphoid nonunion with dorsal intercalated segment instability deformity: a report of three cases
- Seonjeong Lee, Won Sun Lee, Jae Kwang Kim
- Received March 27, 2026 Accepted May 11, 2026 Published online July 7, 2026
- DOI: https://doi.org/10.12671/jmt.2026.00136 [Epub ahead of print]
-
 Abstract
Abstract
 PDF
PDF - Proximal scaphoid nonunion is difficult to treat because the proximal fragment is small and biologically compromised. Secure fixation can be especially challenging when dorsal intercalated segment instability (DISI) is present and requires correction. We report three male patients with proximal scaphoid nonunion and DISI deformity who underwent volar fixation with two 2.4-mm headless compression screws and cancellous bone graft harvested from the distal radius at the Lister tubercle. Preoperative computed tomography confirmed a proximal nonunion line and proximal fragment dimensions considered sufficient for dual-screw fixation, and magnetic resonance imaging showed no definite avascular necrosis. Early postoperative computed tomography showed maintained fixation and alignment in all three patients. Although CT-confirmed union at final follow-up was not uniformly available, radiographic union defined on plain radiographs was achieved in all cases without loss of alignment or carpal collapse. Carpal alignment improved in two patients, but DISI persisted in one. One patient underwent secondary removal of a preexisting loose body and one screw. This small case series suggests that dual-screw fixation with cancellous grafting may be technically feasible in selected proximal scaphoid nonunions with concomitant DISI. Level of evidence: IV.
- 49 View
- 1 Download

Original Article
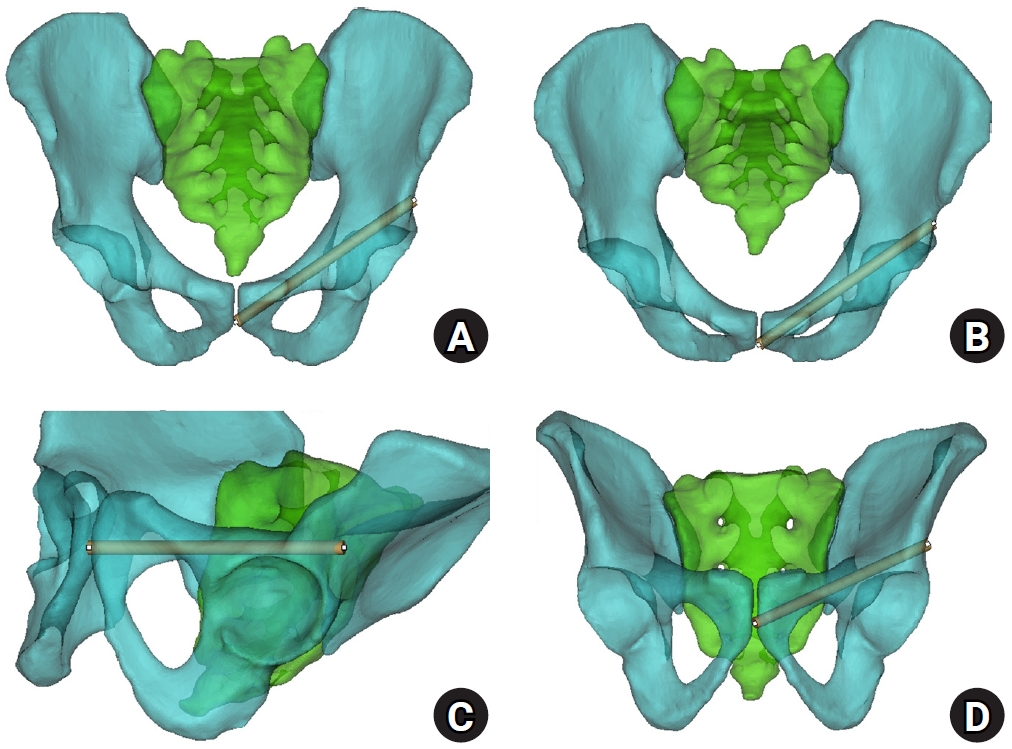
- Sex-specific bottlenecks and risk zones in the retrograde superior pubic ramus screw corridor: a 3D CT-based morphometric cadaver study
- Ji Won Jeong, Jung Tae Ahn, Gu Hee Jung, Kun Tae Kim
- J Musculoskelet Trauma 2026;39(2):103-116. Published online March 26, 2026
- DOI: https://doi.org/10.12671/jmt.2026.00066
-
Abstract
PDF
 Supplementary Material
Supplementary Material - Background
Superior ramus screw fixation is commonly used to stabilize anterior pelvic ring injuries but is constrained by a narrow, irregular, and curved intraosseous corridor. Trajectory-based morphometric analysis may assist in screw diameter selection and enable identification of reproducible anatomic constriction zones.
Methods
We conducted a cross-sectional computed tomography (CT)-based morphometric study of 82 cadaveric pelvises (42 males, 40 females). Bottleneck diameter was defined as the diameter of the largest fully contained virtual cylinder along the planned trajectory, and cylinder length was recorded. Orthogonal cross-sections at 9.5-mm intervals (up to 12 segments) were generated to measure segment-wise effective diameter (defined as twice the minimum centerline-to-cortex distance) and cortical clearance, which was used as a diameter-based safety margin. Segments were realigned to the acetabular start segment to define relative segment positions (Δ seg). Feasibility was assessed for prespecified screw diameters ranging from 3.5 to 7.3 mm.
Results
Mean bottleneck diameter was larger in males than in females (7.34±1.10 vs. 5.93±0.98 mm), whereas trajectory length was similar between sexes (127.85±8.54 vs. 128.85±8.20 mm). Δ seg realignment localized corridor constriction to two discrete zones: a preacetabular zone (Δ seg −6 to −4) and a periacetabular zone (Δ seg 1 to 2), where effective diameter and cortical clearance were most limited. Feasibility rates were 100% at 3.5–4.5 mm, 95.2% vs. 82.5% at 5.0 mm, 81.0% vs. 27.5% at 6.5 mm, and 59.5% vs. 10.0% at 7.3 mm in males and females, respectively.
Conclusions
Female models demonstrated smaller trajectory-wide bottleneck diameters and segment-wise effective diameters than male models. Acetabular-referenced Δ seg realignment identified two reproducible anatomic risk zones: a preacetabular zone adjacent to the obturator neurovascular bundle and a periacetabular zone near the external iliac vessels. At diameters ≥6.5 mm, cortical proximity increased more prominently in females than in males. Level of evidence: III.
- 906 View
- 25 Download
 First
First Prev
Prev

