 E-submission
E-submission TOTA
TOTA TOTS
TOTS
Search
- Page Path
- HOME > Search
Original Article
-
NSAID-induced suppression of type X collagen and VEGF expression in the early phase of rat femoral fracture healing

- Maria Zafar, Rana Mohammad Zeeshan, Safia Tasawar, Muhammad Saad Ilyas, Amer Aziz, Uruj Zehra
- J Musculoskelet Trauma 2026;39(2):162-173. Published online April 10, 2026
- DOI: https://doi.org/10.12671/jmt.2025.00367
-
 Abstract
Abstract
 PDF
PDF Supplementary Material
Supplementary Material - Background
The current literature presents conflicting evidence regarding the effects of nonsteroidal anti-inflammatory drugs (NSAIDs) on fracture healing. This experimental study aimed to evaluate and compare the histological and immunohistochemical changes during femoral fracture healing in rats treated with a nonselective cyclooxygenase (COX) inhibitor (diclofenac sodium) and a selective COX-2 inhibitor (celecoxib).
Methods
Thirty-six male Wistar (standard outbred) albino rats weighing 200–400 g underwent standardized mid-diaphyseal femoral fracture surgery. The animals were randomized into three groups (n=12 per group): group 1 received diclofenac sodium, group 2 received celecoxib, and group 3 served as the control group and received 1 mL of distilled water orally once daily. Six rats from each group were euthanized at the end of the 2nd and 7th weeks after fracture for sample collection. Histological examination was complemented by immunohistochemical analysis, and the expression of type X collagen and vascular endothelial growth factor (VEGF) was assessed using the immunoreactive score (IRS) method.
Results
Healing scores were significantly higher in the control group at both time points (2nd week, P=0.01; 7th week, P=0.03). At the 2nd week, rats treated with diclofenac sodium demonstrated significantly greater fibrosis (P=0.01), and by the 7th week, they exhibited impaired bone formation (P=0.003) along with increased bone defects (P=0.01). IRS values for type X collagen and VEGF were significantly higher in the control group than in both treatment groups during the 2nd week (P=0.01 and P=0.005, respectively).
Conclusions
These findings suggest that, in this rat model, NSAIDs, particularly nonselective COX inhibitors, may disrupt the early phases of bone repair by affecting hypertrophic chondrocyte differentiation and reducing angiogenic activity. Although these results indicate a potential risk to optimal healing, they are preclinical observations, and their relevance to clinical fracture management should be interpreted with caution. Level of evidence: V.
- 807 View
- 19 Download

Review Articles
- Combined acetabular and pelvic ring injuries: a reference-frame algorithm for definitive fixation sequencing
- Jeong-Hyun Koh, Seungyeob Sakong
- J Musculoskelet Trauma 2026;39(2):83-92. Published online April 9, 2026
- DOI: https://doi.org/10.12671/jmt.2026.00031
-
Abstract
PDF
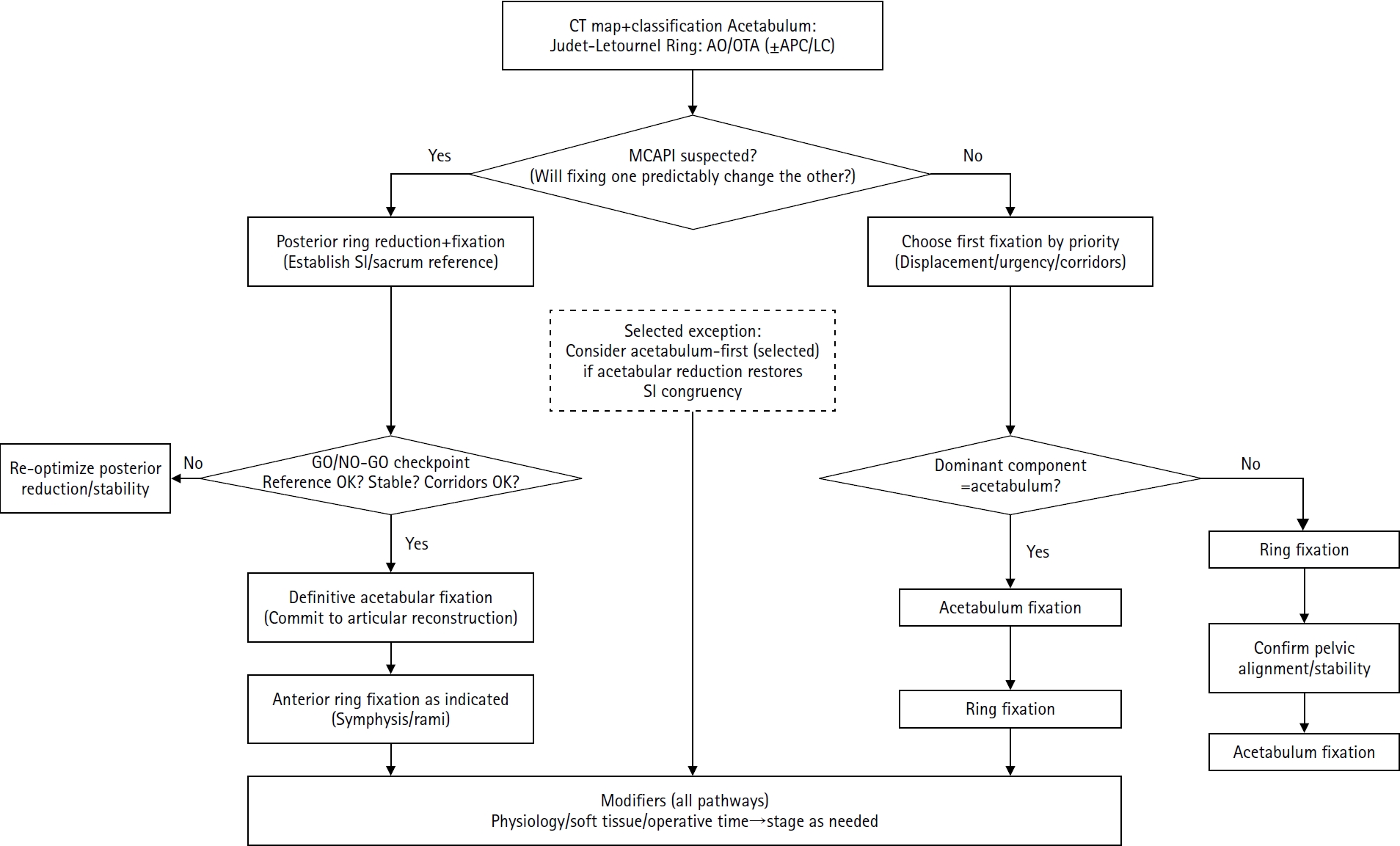
- Combined acetabular and pelvic ring injuries are not simply “two fractures in one patient.” Reduction and fixation of one component can alter the alignment and reducibility of the other, rendering operative sequencing a primary decision variable rather than a secondary consideration. These injuries typically result from high-energy trauma, frequently occur in patients with polytrauma, and are further influenced by physiological tolerance and the feasibility of available operative corridors. The existing evidence base remains constrained by retrospective study designs, inconsistent definitions, variable classification systems, and heterogeneous outcome reporting, all of which limit the strength of comparative recommendations. This state-of-the-art review presents a surgeon-facing, algorithmic approach grounded in a reference-frame mindset. We emphasize computed tomography (CT)-based mapping and the use of consistent terminology to characterize acetabular morphology, pelvic ring instability, deformity vectors, suspicion of mechanical coupling, and feasible operative corridors. Mechanically connected acetabular and pelvic ring injuries (MCAPI) are introduced as a working framework for identifying patterns in which reduction or fixation of one injury predictably influences the other. In cases of suspected MCAPI, a posterior ring-based sequence is generally preferred, typically consisting of posterior ring reduction and fixation, definitive acetabular reconstruction, and subsequent anterior ring fixation. We propose an explicit intraoperative “GO/NO-GO” checkpoint (reference acceptable, stable, corridors feasible) to prevent acetabular reconstruction on a moving target. Acetabulum-first strategies may be appropriate only in selected anteroposterior compression- type configurations in which acetabular fixation plausibly restores sacroiliac congruency and posterior stabilization remains technically feasible. We summarize key outcome domains and complication patterns, highlighting hip dislocation as an important risk factor associated with both neurologic deficits and overall complications. Standardized CTbased definitions and outcome instruments, together with multicenter cohorts employing predefined decision pathways, are required to test sequencing strategies and to determine whether improved radiographic reduction translates into durable functional benefit.
- 998 View
- 25 Download
- Definitive fixation for traumatic pelvic ring injuries: a dynamically informed, posterior-referenced framework
- Jeong-Hyun Koh, Seungyeob Sakong
- J Musculoskelet Trauma 2026;39(2):73-82. Published online March 24, 2026
- DOI: https://doi.org/10.12671/jmt.2026.00045
-
Abstract
PDF
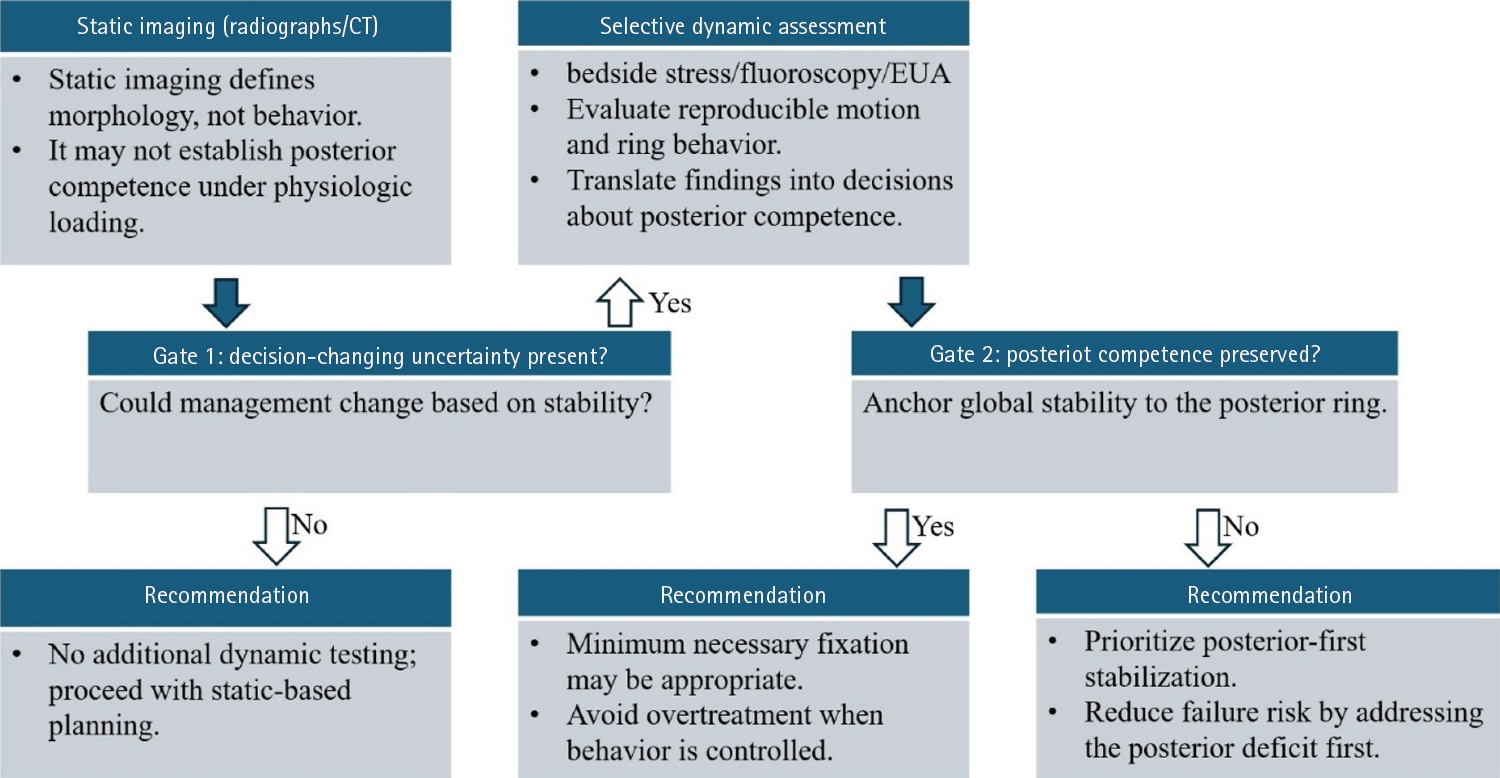
- Optimal definitive fixation for traumatic pelvic ring injuries remains challenging because static radiographs and computed tomography, although essential for defining morphology, do not consistently predict load-dependent behavior during early mobilization. This uncertainty contributes to substantial practice variation and continued reliance on simplified displacement thresholds, such as the 2.5 cm rule. Such rules can misclassify instability by underrepresenting posterior competence and by privileging static measurements over functional behavior. In this narrative review, we propose a dynamically informed, posterior- referenced framework composed of three linked elements: (1) decision-linked terminology that explicitly distinguishes dynamic instability, radiographic change, and clinical failure; (2) selective stress-based assessment when uncertainty is likely to alter management; and (3) escalation along a fixation continuum that weighs incremental stability against operative burden. When static imaging cannot establish posterior competence with confidence, we outline selective stress-based approaches to assess pelvic ring behavior and to translate demonstrated instability into fixation selection along a defined continuum. Across all steps, the framework emphasizes minimum necessary fixation and explicitly incorporates the cost of selection as a primary decision variable. The operative question, therefore, shifts from gap width alone to clinically relevant motion and preservation of posterior competence. In doing so, this approach aims to reduce both undertreatment and overtreatment and to improve the consistency and defensibility of definitive fixation strategies across diverse practice environments.
- 1,508 View
- 35 Download
- Current concepts in the management of phalangeal fractures in the hand
- Hyun Tak Kang, Jun-Ku Lee
- J Musculoskelet Trauma 2025;38(3):109-123. Published online July 22, 2025
- DOI: https://doi.org/10.12671/jmt.2025.00136
-
Abstract
PDF
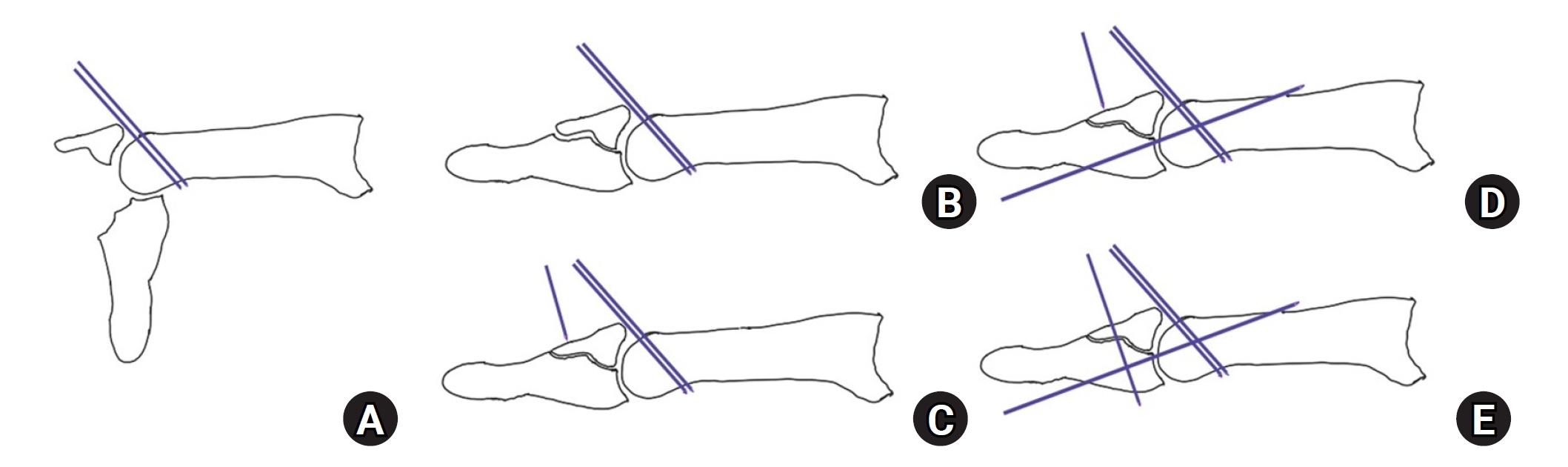
- This review focuses on the treatment of hand fractures based on the anatomical location of the fractured phalanx, excluding the thumb, and examines recent studies on the topic. The main points are as follows: in most cases of hand fractures, conservative treatment should be prioritized over surgical intervention. The three key factors in determining whether surgical treatment is necessary are (1) whether the fracture is intraarticular, (2) the stability of the fracture itself, and (3) the extent of damage to surrounding soft tissues. The primary surgical treatment is closed reduction and Kirschner-wire fixation. The risk of rotational deformity increases with fractures closer to the proximal region. Intra- articular fractures may lead to subsequent stiffness and arthritis; thus, computed tomography is recommended to assess the fracture pattern. Anatomic reduction of intraarticular fragments is required, along with correction of the inherent joint instability. No surgical method has proven to be superior; it is advantageous for the surgeon to choose a surgical approach they are familiar with and confident in, based on the specific fracture and patient factors. Complications in hand fractures are various; the most frequent is stiffness, and nonunion is uncommon. Early joint motion is crucial in minimizing the risk of stiffness.
-
Citations
Citations to this article as recorded by
- Imaging of hand and wrist injuries in alpine skiing: common injury mechanisms, imaging findings, and treatment
Andreas Josef Walch, Andreas Schweizer, Reto Sutter
Skeletal Radiology.2026;[Epub] CrossRef
- Imaging of hand and wrist injuries in alpine skiing: common injury mechanisms, imaging findings, and treatment
- 37,548 View
- 702 Download
- 1 Crossref
Original Article
- Computational simulation of coracoclavicular screw insertion through the superior distal clavicular plate for clinical applications in Korean cadavers
- Hyung-Lae Cho, Ji Han Choi, Se-Lin Jeong, Gu-Hee Jung
- J Musculoskelet Trauma 2025;38(3):143-151. Published online July 22, 2025
- DOI: https://doi.org/10.12671/jmt.2025.00122
-
Abstract
PDF
- Background
The study was conducted to determine the practical area for inserting the coracoclavicular (CC) screw through the plate by analyzing three-dimensional (3D) shoulder models featuring virtually implanted, actual-size plates and screws.
Methods
Ninety cadaveric shoulders (41 males and 49 females) underwent continuous 1.0-mm slice computed tomography scans. The data were imported into image-processing software to generate a 3D shoulder model, including the scapula and clavicle. The overlapping area between the clavicle and the horizontal portion of the coracoid process (horizontal portion_CP) was analyzed in the cranial view. A curved pelvic recon plate was virtually placed on the upper surface of the distal clavicle, and an actual-size (3.5 mm) CC screw was inserted through the plate.
Results
The distal clavicle directly overlapped with the horizontal portion_CP in the vertical direction. The overlapping area was sufficient to place the 3.5 mm and 4.5 mm-sized screws. In all shoulder models, the CC screw could be inserted through the plate into the vertical direction, with an average length of 35.5 mm (range, 26.2–62.5 mm; standard deviation, 1.2 mm). In 87 models, the CC screw was inserted through the third hole from the lateral end of the plate. Two models were inserted through the second hole, and one model through the fourth hole.
Conclusions
The upper surface of the clavicle has sufficient overlapping area to place CC screws through the plate in the vertical direction in the corresponding hole. Supplemental CC screw fixation through the plate can be performed without additional or special equipment. Level of evidence: IV
- 1,171 View
- 25 Download
Review Articles
- Atypical femoral fractures: an update
- Won-Tae Cho, Jeong-Hyun Koh, Seungyeob Sakong, Jung-Taek Kim
- J Musculoskelet Trauma 2025;38(2):41-52. Published online March 28, 2025
- DOI: https://doi.org/10.12671/jmt.2025.00031
-
Abstract
PDF
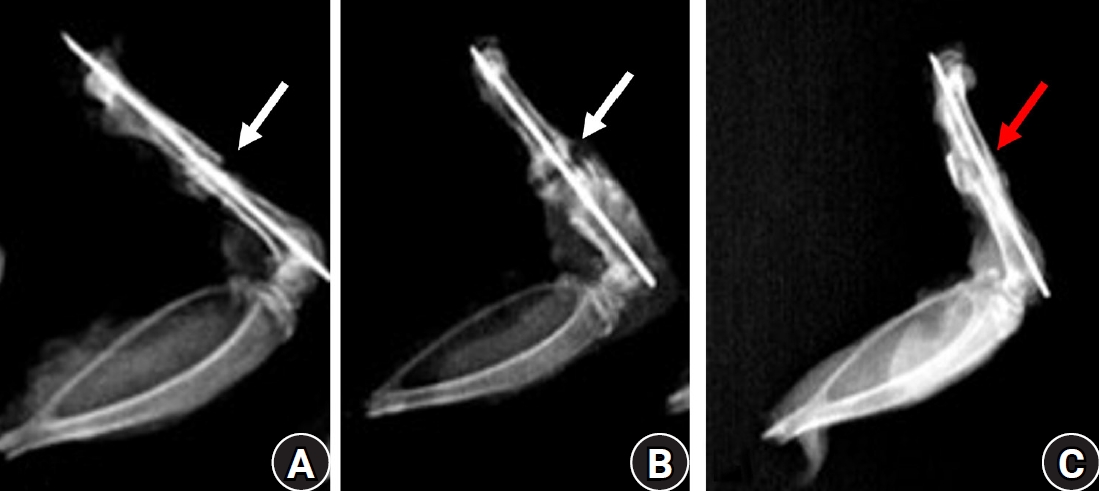
- This narrative review provides an up-to-date overview of atypical femoral fractures (AFFs), emphasizing diagnostic criteria, epidemiology, pathophysiology, risk factors, and evaluation with screening strategies. AFFs are rare but significant complications associated with prolonged bisphosphonate (BP) therapy for osteoporosis. Although the pathogenesis of AFFs has not been fully elucidated, its primary mechanism is thought to involve impaired bone remodeling, leading to unhealed microfractures that progress to stress fractures under repetitive loading. AFFs can occur in various regions of the femur, influenced by femoral geometry and the lower limb axis. Other risk factors include prolonged steroid use, arthroplasty, genetic predispositions, and metabolic bone disorders. The diagnosis of AFFs is based on criteria established by the American Society for Bone and Mineral Research. Key radiographic features include lateral cortical transverse fracture lines and localized cortical thickening, typically with minimal or no comminution on the medial cortex. Dual-energy X-ray absorptiometry for screening tests and magnetic resonance imaging as an advanced imaging modality enable the early detection of incomplete fractures. This multi-modal approach facilitates the prompt identification of prodromal cortical changes, reducing the risk of complete fractures in high-risk populations, particularly patients undergoing prolonged BP therapy. Level of Evidence: V
-
Citations
Citations to this article as recorded by- Clinical Images: Bisphosphonate‐associated atypical femoral fracture with contralateral cortical beaking
Andreina Martinez Paulino, Valentin Marian
ACR Open Rheumatology.2026;[Epub] CrossRef - Atypical femoral fracture: The periprosthetic variant about two cases without bisphosphonate use
Guillaume Auberger, Thomas Aubert, Younes Kerroumi, Philippe Leclerc, Simon Marmor
SICOT-J.2026; 12: 41. CrossRef - Atypical Femur Fractures Without Bisphosphonate Exposure (AFFwB): A Retrospective Report of 21 Cases
Lorenzo Lucchetta, Carmelinda Ruggiero, Samuele Berardi, Alice Franceschi, Michele Bisaccia, Giuseppe Rinonapoli
Journal of Clinical Medicine.2025; 15(1): 25. CrossRef
- Clinical Images: Bisphosphonate‐associated atypical femoral fracture with contralateral cortical beaking
- 65,535 View
- 655 Download
- 3 Crossref
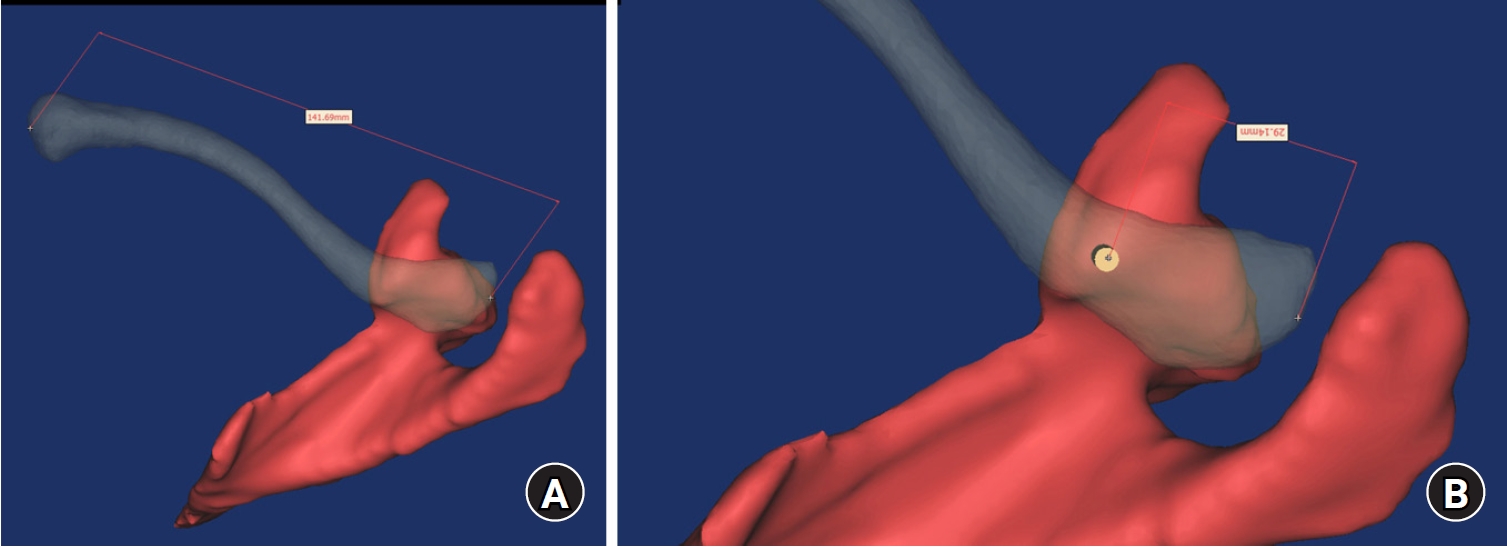
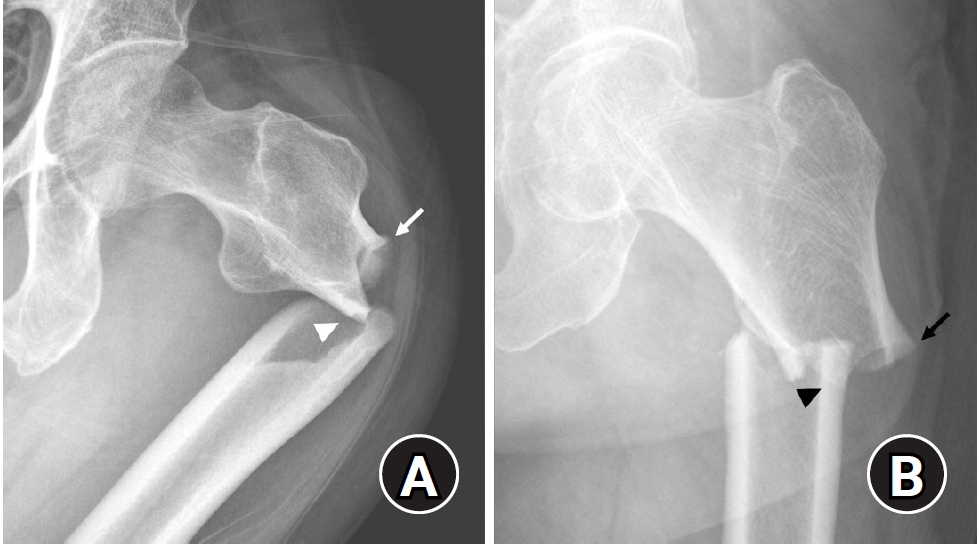
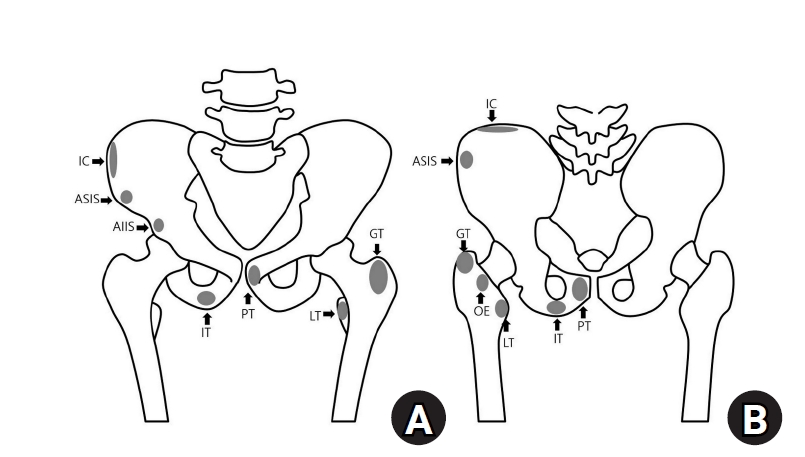
- Avulsion fractures around the hip joint and pelvis
- Won-Sik Choy, Yonghan Cha, Jung-Taek Kim, Jun-Il Yoo, Jin-Woo Kim
- J Musculoskelet Trauma 2025;38(2):53-62. Published online March 24, 2025
- DOI: https://doi.org/10.12671/jmt.2025.00010
-
Abstract
PDF
- Avulsion fractures occur when tendons or ligaments are subjected to forces greater than they can withstand at the apophysis or enthesis, regardless of fusion status. The pelvis and hip joint are vulnerable to these injuries due to the diverse muscular structures in these structures, which serve as origins for multiple muscles leading to the lower extremities. Pelvic avulsion fractures commonly affect young athletes, but can also occur in adults. The diagnosis typically involves assessing trauma history, a clinical examination, and radiographic imaging. If the diagnosis is unclear, additional tests such as computed tomography and magnetic resonance imaging may assist in the diagnosis and provide useful information for treatment decisions. While most avulsion fractures respond well to conservative treatment, surgical intervention may be preferred in severe displacements, cases of significant retraction in active athletes, or when a faster recovery is necessary. Chronic or neglected injuries may lead to excessive osseous formation around the pelvis, causing impingement syndromes. Recognizing characteristic radiological findings based on pelvic anatomy helps to make an accurate diagnosis, as chronic injuries can mimic tumors or infectious conditions, necessitating a careful differential diagnosis.
-
Citations
Citations to this article as recorded by- Avulsion Fracture of the Lesser Trochanter and the Use of Conservative Treatment
Dawid Bartosik, Bartlomiej Cwikla, Anna Kowalczyk, Michalina Loson-Kawalec, Anna Palka-Szymaniec, Bartosz Starzynski, Alina Keska, Jakub Szkuta, Klaudia Wojcik
Cureus.2026;[Epub] CrossRef - Outcomes of Conservative Versus Surgical Treatment of Adolescent Pelvic and Hip Avulsion Fractures: A Systematic Review and Meta-Analysis
Lindsey L. Molina, Andrew M. Block, Sasha Carsen, Allison E. Crepeau, Tyler J. Stavinoha, Michael M. Chau, Jeffrey J. Nepple
Journal of Pediatric Orthopaedics.2026;[Epub] CrossRef - Diagnostic Accuracy of Ultrasound for Adolescent Pelvic Avulsion Fractures: A Blinded Multirater Study
Meena Meiyyappan, Robert Van Pelt, Kate Lampe, Jane Chung, Matthew Ditzler, Shane Miller, Henry Ellis, Hamza Alizai, Matthew Hammer, Ben Johnson, Charles Wyatt, Jacob Jones
Journal of Clinical Ultrasound.2026;[Epub] CrossRef
- Avulsion Fracture of the Lesser Trochanter and the Use of Conservative Treatment
- 18,509 View
- 200 Download
- 3 Crossref
- Easily missed nondisplaced fractures accompanying complete fractures in the lower extremity and pelvis: a narrative review
- Young-Chang Park
- J Musculoskelet Trauma 2025;38(1):5-12. Published online January 24, 2025
- DOI: https://doi.org/10.12671/jmt.2025.00017

-
Abstract
PDF
- Nondisplaced fractures accompanying complete fractures are often difficult to detect on plain radiographs or computed tomography scans, posing a diagnostic challenge. The diagnosis of these frequently overlooked injuries can be delayed, potentially leading to suboptimal patient outcomes. This review discusses four commonly missed fracture patterns in the lower extremity and pelvis, including posterior involvement in fragility fractures of the pelvis, intertrochanteric extensions in isolated greater trochanter fractures, ipsilateral femoral neck fractures in high energy femoral shaft fractures, and posterior malleolar fractures in distal spiral tibial shaft fractures. An accurate diagnosis of these accompanying nondisplaced fractures is critical for optimizing surgical outcomes. Surgeons should incorporate thorough preoperative evaluations into their clinical practice to facilitate early detection and appropriate treatment strategies. Prompt identification and comprehensive management remain essential for improving patient outcomes.
-
Citations
Citations to this article as recorded by- Selective Anterior Fixation for Rami Fractures in Anteroposterior Compression-Type Pelvic Ring Injuries: Impact of Posterior Stability
Jeong-Hyun Koh, Sumin Lim, Won-Tae Cho, Seungyeob Sakong, Wan-Sun Choi, Daehyun Han, Hyung Keun Song
Journal of Clinical Medicine.2026; 15(10): 3773. CrossRef - Initial lateral stress radiographs predict instability in fragility fractures of the pelvis type I and II: a prospective observational study
Kyu-Hyun Yang, Jun-Young An, Young-Chang Park
Scientific Reports.2026;[Epub] CrossRef
- Selective Anterior Fixation for Rami Fractures in Anteroposterior Compression-Type Pelvic Ring Injuries: Impact of Posterior Stability
- 3,279 View
- 63 Download
- 2 Crossref
Original Article
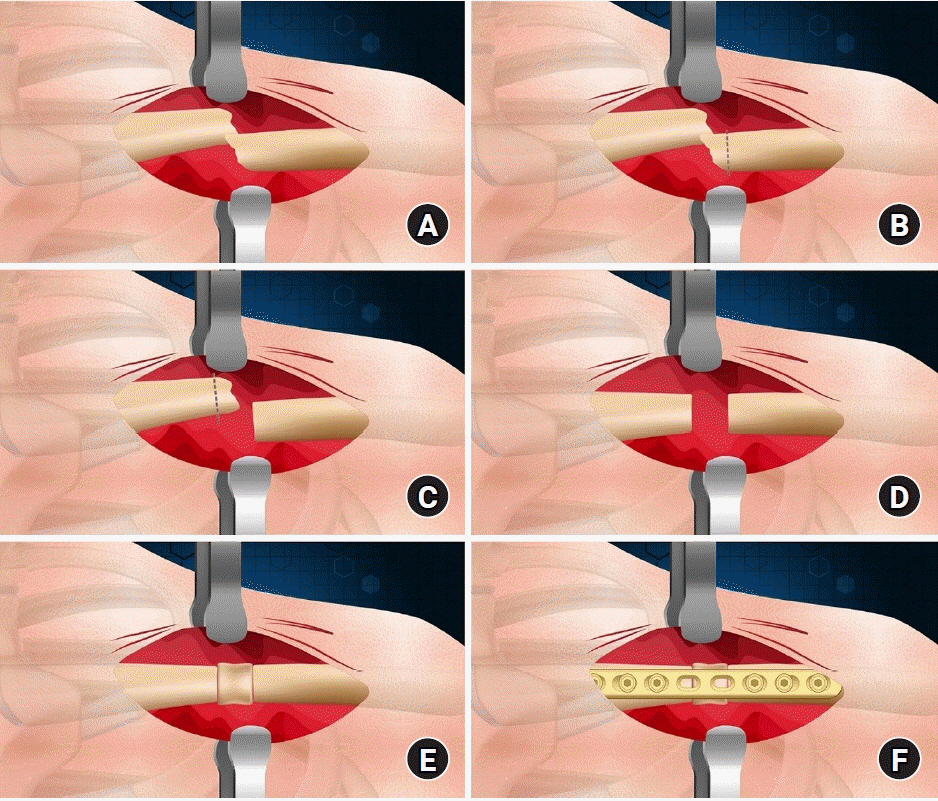
- Interpositional tricortical iliac bone graft in nonunion of midshaft clavicular fractures
- Eun-Seok Son, Bum-Soon Park, Chang-Jin Yon, Chul-Hyun Cho
- J Musculoskelet Trauma 2025;38(1):23-31. Published online January 24, 2025
- DOI: https://doi.org/10.12671/jmt.2025.00004
-
Abstract
PDF
- Background
The purpose of this study was to investigate the radiological and clinical outcomes after interpositional tricortical iliac bone graft with plate fixation for the nonunion of clavicle midshaft fractures. Methods: Between 2007 and 2020, 17 cases who were treated by interpositional tricortical iliac bone graft with plate fixation for the clavicle midshaft nonunion combined with bone defect were investigated. The mean age was 53 years (range, 22–70 years). The mean follow-up period was 102.2 months (range, 18–193 months). Serial plain radiographs were used to evaluate radiological outcomes. The University of California, Los Angeles (UCLA) score, American Shoulder and Elbow Surgeons (ASES) score, and Quick-disabilities of the arm, shoulder, and hand (DASH) score were used to evaluate clinical outcomes. Complications were also evaluated. Results: All cases achieved complete bony union with mean healing time of 17.6 weeks (range, 14–22 weeks). The mean clavicle length difference was significantly decreased from 9.1 mm preoperatively to 2.6 mm postoperatively (P<0.001). The mean UCLA and ASES scores were significantly improved from 18.1 and 52.2 before surgery to 30.6 and 88.6 after surgery (both P<0.001), respectively. The mean final Quick-DASH score was 18.0. Three cases (17.6%) developed postoperative complications including two cases of shoulder stiffness and one case of screw irritation. Conclusions: Interpositional tricortical iliac bone graft with plate fixation for the clavicle midshaft nonunion demonstrated excellent radiological and clinical outcomes. In cases of atrophic nonunion combined with bone defect, this technique is an effective option that can provide structural support and restore clavicle length. Level of evidence: Level IV, case series.
- 3,609 View
- 59 Download
Review Article
- Fracture-Related Complication: Fat Embolism Syndrome
- Beom-Soo Kim
- J Korean Fract Soc 2023;36(3):95-102. Published online July 31, 2023
- DOI: https://doi.org/10.12671/jkfs.2023.36.3.95
-
Abstract
PDF
- Fat embolization is a common occurrence after trauma or during orthopedic procedures involving intramedullary manipulation. Although uncommon, fat embolism syndrome (FES) with respiratory failure, neurologic dysfunction, and petechial rash can be fatal to patients. Two theories are proposed for the manifestation of FES: in the mechanical theory, FES occurs when fat tissue in the bone marrow enters the bloodstream and mechanically blocks it; the biochemical theory proposes that FES occurs due to an inflammatory reaction caused by free fatty acids. There are currently no clear diagnostic criteria for FES, and symptoms and signs are typically nonspecific. For the treatment of FES, conservative and supportive management is performed for the specific symptoms, and close monitoring of the respiratory and neurologic systems is required in high-risk groups. Early fracture fixation of long bones helps prevent and reduce the severity of fat embolism.
- 2,001 View
- 17 Download
Original Articles
- Delayed Operative Treatment of Long Bone Fractures in Patients with Brain Injury
- Hong Moon Sohn, Sang Ho Ha, Jun Young Lee, Young Kwan Lee
- J Korean Fract Soc 2006;19(2):157-162. Published online April 30, 2006
- DOI: https://doi.org/10.12671/jkfs.2006.19.2.157
-
Abstract
- PURPOSE
To evaluate the postoperative progress and outcomes of bone injured patients with long bone fracture showing callus formation and deformity due to delayed surgical treatment.
MATERIALS AND METHODS
10 cases with more than 1 year follow up were chosen from 12 patients with long bone fracture whose surgical treatment was delayed due to brain injury. Exuberant callus formation and deformations were observed. Average delayed period was 6.7 weeks (4~10 weeks). Preoperative callus formation, shortening and angulation were evaluated using plain radiographs. Total operation time and transfusion amount were compared with that from operations done within 2 weeks following accident. Postoperative bone union was checked.
RESULTS
In all cases, preformed angulation and hypertrophic ossification made reduction difficult and this increased total operation time and transfusion amount but had no statistical importance. In patients with humerus and femur fractures accompanying brain injury, massive hypertrophic ossification was observed both in preoperative period and in postoperative period. Average bone union period was 13.5 weeks in humerus fractures, 17.9 weeks in femur fractures. The bone union period was shorter in subject group but had no statistical importance.
CONCLUSION
Early surgical treatment is essential to patients with long bone fracture accompanying brain injury but if early surgical treatment can not be done, proper immobilization to fracture site should be done. -
Citations
Citations to this article as recorded by- Alterations in Serum Levels of Receptor Activator of Nuclear Factor-κB Ligand and Osteoprotegerin in Patients with Head Injury and Fracture
Shin Young Park, Kuen Tak Suh, Chang Hoon Ryu, Seung Hun Woo, Jung Sub Lee, Seong-Gang Kim
Journal of the Korean Fracture Society.2008; 21(2): 145. CrossRef
- Alterations in Serum Levels of Receptor Activator of Nuclear Factor-κB Ligand and Osteoprotegerin in Patients with Head Injury and Fracture
- 1,453 View
- 0 Download
- 1 Crossref
- Use of Cancellous Bone Allograft in the Treatment of Long bone Fractures
- Keun Bae Lee, Taek Rim Yoon, Jae Yoon Chung, Sung Taek Jung, Jae Joon Lee
- J Korean Soc Fract 2001;14(4):776-782. Published online October 31, 2001
- DOI: https://doi.org/10.12671/jksf.2001.14.4.776
-
Abstract
PDF
- PURPOSE
The goal of our study was to evaluate the usefulness of frozen cancellous bone allograft in the treatment of long bone fractures that had bone defect and nonunion.
MATERIALS AND METHODS
22 cases of long bone fractures(femur and tibia) with severe comminution or bone defect and nonunion were treated by operation using frozen cancellous bone allograft from March 1998 through May 2000. Thirteen were male and nine were female. The average age was 55 years old (range, 17-76 years) and the mean duration of follow-up was 20.1 months(range, 10-37 months). Eleven cases were femoral fractures, 7 cases of tibial fractures, and 4 cases of nonunion. Allografts were achieved from the patients of femoral neck fracture or osteoarthritis of the hip, and cadaveric donors. The specimens were carefully evaluated based on medical history and laboratory examination about the acute or chronic infection, and bloodtransmitted diseases. The results were evaluated by clinically, such as infection, pain at fracture site, immunological rejection and by radiologically union or resorption of allografts.
RESULTS
Radiologically, bone union was obtained in 14 cases(63.6%) at 6 months after operation, in all except two cases(90.9%) at 9 months after operation. Clinically, pain at fracture site, infection, and immunologic rejection were not observed.
CONCLUSION
In the treatment of severe comminuted fracture or nonunion of long bones, cancellous allograft transplantation after strict donor selection and appropriate screening was a good substitution for autograft avoiding of donor site morbidity or limitation in quantity. -
Citations
Citations to this article as recorded by- Influence of Process Conditions on the Quality Characteristics of Beef-Bone Broth
Byung-Su Kim, Gye-Won Kim, Jae-Yong Shim
Food Engineering Progress.2014; 18(1): 15. CrossRef
- Influence of Process Conditions on the Quality Characteristics of Beef-Bone Broth
- 991 View
- 0 Download
- 1 Crossref
- Surgical Treatment of Concomitant Ipsilateral Humerus and Forearm Fractures
- Jeung Tak Suh, Sung Hun Kim, Chong Il Yoo
- J Korean Soc Fract 1994;7(2):316-321. Published online November 30, 1994
- DOI: https://doi.org/10.12671/jksf.1994.7.2.316
-
Abstract
PDF
- The term "floating elbow" refers to concomitant ipsilateral humeral and forearm bone fractures. This type of fractures is relatively rare and has few guidelines for treatment. Author reviewed 14 cases of these fractures which were treated by open reduction and rigid internal fixation in Pusan National University Hospital from January 1983 to January 1993. In follow up study, Author obtained that good results in 10 cases(71%) of patient, and fair results in 3 cases of patient. Author advocate the patient with concomitant ipsilateral humerus and forearm bone fractures should requires open reduction and stable internal fixation of the both humerus and forearm bone, as soon as possible.
- 643 View
- 0 Download
 First
First Prev
Prev

