 E-submission
E-submission TOTA
TOTA TOTS
TOTS
Search
- Page Path
- HOME > Search
Original Articles
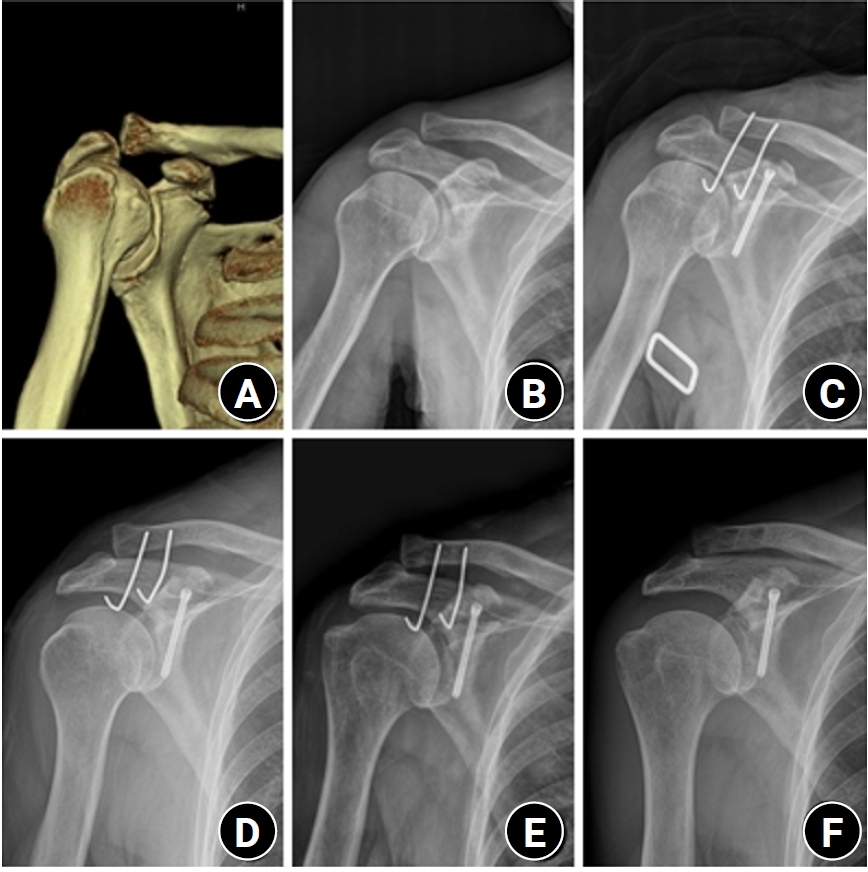
- Surgical outcomes of the coracoid process fracture associated with the acromioclavicular joint injury in Korea: a case series
- Dongju Shin, Sung Choi, Sangwoo Kim, Byung Hoon Kwack
- J Musculoskelet Trauma 2026;39(1):54-61. Published online January 14, 2026
- DOI: https://doi.org/10.12671/jmt.2025.00346
-
 Abstract
Abstract
 PDF
PDF - Background
Excluding technical reports and isolated case reports, there are no published studies evaluating coracoid process fixation with or without an acromioclavicular joint (ACJ) stabilization procedure for coracoid process fractures associated with ACJ injury. The purpose of this study was to assess the surgical outcomes of coracoid process fractures associated with ACJ injuries and to determine the usefulness of coracoid process fixation with or without an ACJ stabilization procedure.
Methods
From February 2006 to December 2015, patients with coracoid process fractures associated with ACJ injuries were enrolled. Radiological and clinical outcomes were analyzed in 12 patients who underwent coracoid process fixation with or without an ACJ stabilization procedure. A 3.5-mm cannulated screw with a washer or a 3.0-mm headless compression screw was used for coracoid process fixation, and either a clavicle hook plate or Kirschner (K)-wires were used for ACJ injuries when additional fixation was necessary.
Results
Bone union was achieved in 11 patients (91.7%), while one case was determined to be a nonunion at 6 months. Radiological union occurred at an average of 3 months (range, 1.5–4 months) in all patients except the nonunion case. At the final follow-up, the average clinical scores were a visual analogue scale (VAS) pain score of 1.5 (range, 0–4) and a UCLA score of 30.9 (range, 28–35). Clinical outcomes were satisfactory in all patients, including the patient with nonunion.
Conclusion
The clinical and radiological outcomes of treating coracoid process fractures associated with ACJ injuries using coracoid process fixation with or without ACJ stabilization were favorable. A cannulated screw with a washer and clavicle hook plate fixation may provide sufficient stability for both the coracoid process fracture and the ACJ injury when feasible. Level of evidence: IV.
- 862 View
- 20 Download

- A Comparison of Results between AO Hook Plate and TightRope for Acute Acromioclavicular Joint Dislocation
- Yong Gun Kim, Ho Jae Lee, Dong Won Kim, Jinmyoung Dan
- J Korean Fract Soc 2017;30(1):16-23. Published online January 31, 2017
- DOI: https://doi.org/10.12671/jkfs.2017.30.1.16
-
Abstract
PDF
- PURPOSE
The purpose of our study is to compare the radiographic and clinical outcomes with respect to acromioclavicular (AC) joint dislocation depending on the surgical method: Hook plate (HP) versus TightRope (TR).
MATERIALS AND METHODS
Between May 2009 and May 2012, 51 patients with Rockwood type III-V lesions received clinical and radiographic follow-up. Patients were divided into two groups according to the surgical methods (HP: n=32; TR: n=19). Radiological follow-up included comparative coracoclavicular distance (CCD) measurements as a percentage of the uninjured shoulder. For clinical follow-up, a standardized functional shoulder assessment with the Constant score, University of California at Los Angeles (UCLA) score, and Korea shoulder score (KSS) were carried out.
RESULTS
Comparing the functional results, no differences were observed between the two groups (Constant score: HP, 78.5; TP, 81.4; UCLA score: HP, 29.2; TP, 29.9; KSS: HP, 79.2; TP, 80.7). Time to restoration of the range of motion (ROM) above shoulder level was longer in the HP group than in the TR group. However, the ROM at 1 year postoperation and final follow-up revealed similar results between the two groups. The AC joints were well reduced in both groups, the CCD increased to 44.7% in the HP group and to 76.5% in the TR group at the final follow-up; however, no one was significantly superior to the others. Furthermore, there were 8 cases (25.0%) and 5 cases (26.3%) of AC joint arthritis in the HP group and TR group, respectively. However, the observed AC joint arthritis has a poor correlation between clinical symptom and radiological results in both groups.
CONCLUSION
Both HP and TR fixation could be a recommendable treatment option in acute unstable AC joint dislocation. Both groups showed excellent radiologic and functional results at the final visit. Moreover, there was no significant difference in statistics, except for the time to restoration of ROM above shoulder level. -
Citations
Citations to this article as recorded by
- Suture-Button Fixation Outperforms Hook Plate in Functional Outcomes After Acromioclavicular Joint Dislocation
Murat Aşçı, Mete Gedikbaş
Bozok Tıp Dergisi.2025; 15(4): 477. CrossRef - Arthroscopic Treatment of Acromioclavicular Joint Dislocations
Du-Han Kim, Chul-Hyun Cho
Journal of the Korean Orthopaedic Association.2023; 58(5): 384. CrossRef - Combination of Clavicular Hook Plate with Coracoacromial Ligament Transposition in Treatment of Acromioclavicular Joint Dislocation
Aikebaier Tuxun, Ajimu Keremu, Pazila Aila, Maimaitiaili Abulikemu, Zengru Xie, Palati Ababokeli
Orthopaedic Surgery.2022; 14(3): 613. CrossRef
- Suture-Button Fixation Outperforms Hook Plate in Functional Outcomes After Acromioclavicular Joint Dislocation
- 3,384 View
- 12 Download
- 3 Crossref
- Tension Band Wiring for Distal Clavicle Fracture: Radiologic Analysis and Clinical Outcome
- Seong Cheol Moon, Chul Hee Lee, Jong Hoon Baek, Nam Su Cho, Yong Girl Rhee
- J Korean Fract Soc 2014;27(2):127-135. Published online April 30, 2014
- DOI: https://doi.org/10.12671/jkfs.2014.27.2.127
-
Abstract
PDF
- PURPOSE
The purpose of this study is to evaluate the radiologic and clinical outcomes after tension band wire fixation of Neer type II distal clavicle fractures.
MATERIALS AND METHODS
Twenty-six patients with Neer type II distal clavicle fractures who underwent tension band wire fixation from March 2002 to May 2011 were included in the study. Fifteen cases were classified as Neer type IIa and 11 cases as type IIb. The postoperative mean follow-up period was 14.3 months. Clinical and radiologic evaluation was performed at two weeks, six weeks, three months, six months, and 12 months postoperatively.
RESULTS
Bony union on X-rays was observed at an average of 11.7 weeks (range 8-20 weeks) postoperatively. The overall visual analogue scale score for pain was 1.23+/-2.75 postoperatively. The overall postoperative University of California at Los Angeles score increased to 33.5+/-2.15 from the preoperative score of 21.6+/-1.91 (p<0.05).
CONCLUSION
Among various methods of treatment for Neer type II distal clavicle fracture, K-wire and tension band fixation was used and relatively satisfactory radiological and clinical results were obtained. This surgical method yields excellent clinical results, owing to its relatively easy technique, fewer complications, and allowance of early rehabilitation. -
Citations
Citations to this article as recorded by- Clinical and Radiologic Outcomes of Acute Acromioclavicular Joint Dislocation: Comparison of Kirschner's Wire Transfixation and Locking Hook Plate Fixation
Yong Girl Rhee, Jung Gwan Park, Nam Su Cho, Wook Jae Song
Clinics in Shoulder and Elbow.2014; 17(4): 159. CrossRef
- Clinical and Radiologic Outcomes of Acute Acromioclavicular Joint Dislocation: Comparison of Kirschner's Wire Transfixation and Locking Hook Plate Fixation
- 1,289 View
- 10 Download
- 1 Crossref
- Arthroscopic Treatment of Acromioclavicular Joint Dislocation Using TightRope(R): Preliminary Report
- Eui Sung Choi, Kyoung Jin Park, Yong Min Kim, Dong Soo Kim, Hyun Chul Shon, Byung Ki Cho, Ji Kang Park, Hyun Chul Lee
- J Korean Fract Soc 2010;23(3):310-316. Published online July 31, 2010
- DOI: https://doi.org/10.12671/jkfs.2010.23.3.310
-
Abstract
PDF
- PURPOSE
To evaluate the clinical and radiologic results of the arthroscopic treatment using TightRope(R) (Arthrex, Inc, Naples, FL) for management of acute acromioclavicular dislocation.
MATERIALS AND METHODS
Twelve patients with acromioclavicular joint dislocation Rockwood type V are underwent the arthroscopic acromioclavicular joint reconstruction using TightRope(R) between March, 2008 and March, 2009. The average age was 40.4 years (range 25~63 years) and mean follow-up was 10 months (range 8~16 months). The shoulders were evaluated using parameters include radiologic measurements by comparing the clavicle posteroanterior and lateral radiographs with the contralateral one. Clinical evaluation was made for pain, function, and range of joint motion by Constant score and KSS (Korean Shoulder Score).
RESULTS
All twelve patients returned to their work without pain in 3 months after operation. The average Constant score and KSS score was 98.4 (range 97~100) and 97.8 (range 97~100) at the last follow-up. Because of technical error and indication error, two patients showed failures of TightRope(R) fixation on the coracoid side and the acromioclavicular joint was redislocated, so these cases were excluded. 10 patients were satisfied with functional results and cosmetic appearance.
CONCLUSION
Considering its less morbidity, less hospitalization, excellent cosmesis, early rehabilitation, this new technique offers an attractive alternative in acromioclavicular joint stabilization if the early technical error would be overcome. -
Citations
Citations to this article as recorded by- Coracoclavicular Ligament Augmentation Using Tight-Rope®for Acute Acromioclavicular Joint Dislocation - Preliminary Report -
Seok Hyun Kweon, Sang Su Choi, Seong In Lee, Jeong Woo Kim, Kwang Mee Kim
The Journal of the Korean Shoulder and Elbow Society.2013; 16(2): 115. CrossRef - Coracoclavicular Ligament Augmentation Using Endobutton for Unstable Distal Clavicle Fractures - Preliminary Report -
Chul-Hyun Cho, Gu-Hee Jung, Hong-Kwan Sin, Young-Kuk Lee, Jin-Hyun Park
The Journal of the Korean Shoulder and Elbow Society.2011; 14(1): 1. CrossRef
- Coracoclavicular Ligament Augmentation Using Tight-Rope®for Acute Acromioclavicular Joint Dislocation - Preliminary Report -
- 929 View
- 5 Download
- 2 Crossref
- Modified Spring Plate for Treatment of Unstable Distal Clavicle Fractures
- Sang Myung Lee, Il Jung Park, Hyung Min Kim, Jae Chul Park, Sung Gil Cho, Yoon Chung Kim, Seung Koo Rhee
- J Korean Fract Soc 2010;23(1):64-68. Published online January 31, 2010
- DOI: https://doi.org/10.12671/jkfs.2010.23.1.64
-
Abstract
PDF
- PURPOSE
Unstable distal clavicle fractures should be treated surgically but may be difficult in firm fixation because of small distal fragment. Although a variety of fixation methods have been currently used, none of the methods seem to be firm fixation and little pain. We present a new technique using a spring plate which was modified from one third tubular plate and report the early results.
MATERIALS AND METHODS
Modified spring plate was made from one third tubular plate and the distal hole of the plate was cutting and sharpened by rasp. The sharp edge was bent just like an animal claw (C shape). Between May 2007 and June 2009, a total of six patients with distal clavicle fracture were treated using modified spring plate. A sling was applied in the immediate post operative period for six weeks and exercises were started immediately.
RESULTS
Union was achieved in all cases with excellent results without complication (mean Constant score, 96). All patients had returned to ordinary daily activities but mild limitation of abduction (150 degrees ) by seven weeks after surgery. After six months, the plate was removed.
CONCLUSION
The modified spring plate has provided stable fixation for unstable distal clavicle fixation without disturbance to the acromioclavicular joint, subacromial space, or rotator cuff.
- 588 View
- 1 Download
Case Report
- Clavicle Midshaft Fracture with Acromioclavicular Joint Dislocation: A Case Report
- Chul Hyun Cho, Chul Hyung Kang, Soo Won Jung, Hyuk Jun Seo
- J Korean Fract Soc 2009;22(4):297-299. Published online October 31, 2009
- DOI: https://doi.org/10.12671/jkfs.2009.22.4.297
-
Abstract
PDF
- Clavicle fracture or acromioclavicular joint dislocation is common injury in the upper extremity. But ipsilateral clavicle midshaft fracture with acromioclavicular joint dislocation is a extremely rare. Seven cases has been reported in the English literature, but it has never been reported in Korea. We report a case of clavicle midshaft fracture with acromioclavicular joint dislocation caused by motor vehicle accident and describe its presumed mechanism, diagnosis, treatment with a review of literature.
- 730 View
- 7 Download
Original Articles
- Long Term Follow up Results of the Operative Treatment of the Acromioclavicular Joint Dislocation with a Wolter Plate
- Ki Ser Kang, Han Jun Lee, Jae Sung Lee, Jae Yoon Kim, Yong Beom Park
- J Korean Fract Soc 2009;22(4):259-263. Published online October 31, 2009
- DOI: https://doi.org/10.12671/jkfs.2009.22.4.259
-
Abstract
PDF
- PURPOSE
To evaluate the long-term clinical and radiological results of the operative treatment of the acromioclavicular dislocation with a Wolter plate. MATERIALS AND METHODS: We reviewed clinical and radiological data of twenty patients (mean age: 37 years) who underwent the operative treatment of acromioclavicular joint dislocation using a Wolter plate from September, 1999 to December, 2002 with minimum of five years follow-up (average 6 years 7 months). The clinical outcomes of twenty patients were evaluated by UCLA scoring and radiological results of fifteen patients with available radiograph were evaluated by Zanca view and stress view. RESULTS: The mean UCLA score was mean 33 points (range, 27~35) at final follow up. By clinical evaluation, twelve cases (60%) were excellent, six cases (30%) were good and two cases were poor (10%). By radiological evaluation, eight cases (54%) were excellent (without displacement), five cases (33%) were good (displacement <5 mm) and two cases (13%) were poor (displacement >5 mm). Erosive change in acromioclavicular joint was seen in poor case. CONCLUSION: Wolter plate fixation may be a useful modality for treating acromioclavicular joint dislocation. Great care should be taken to make the hook hole at the appropriate position during operation for long-term prognosis. -
Citations
Citations to this article as recorded by- Clinical outcomes of bending versus non-bending of the plate hook in acromioclavicular joint dislocation
Min Su Joo, Hoi Young Kwon, Jeong Woo Kim
Clinics in Shoulder and Elbow.2021; 24(4): 202. CrossRef - Clinical Comparison of Two Types of Hook Plate in Surgical Treatment of Acromioclavicular Dislocation - AO Hook Plate and Wolter Plate -
Jea-Yeol Choi, Eugene Kim, Haw-Jae Jeong, Jin Whan Ahn, Hun-Kyu Shin, Se-Jin Park, Seung-Hee Lee, Jae-Wook Lee, Kyu-Bo Choi
The Journal of the Korean Shoulder and Elbow Society.2012; 15(2): 123. CrossRef
- Clinical outcomes of bending versus non-bending of the plate hook in acromioclavicular joint dislocation
- 920 View
- 2 Download
- 2 Crossref
- Modified Phemister Technique with Tension Band Wiring in Acromioclaviculr Joint Dislocation
- Yu Jin Kim, Hun Kyu Shin, Ji Won Lee
- J Korean Fract Soc 2006;19(4):431-436. Published online October 31, 2006
- DOI: https://doi.org/10.12671/jkfs.2006.19.4.431
-
Abstract
- PURPOSE
To evaluate the clinical and radiological result of surgical treatment of acromioclavicular joint dislocation, using modified Phemister technique with tension band wiring.
MATERIALS AND METHODS
We chose 17 patients who were able to follow up 1 year or more among the patients who were diagnosed as acromioclavicular joint dislocation in our hospital through January 2000 to Feburary 2005 and took modified Phemister technique with tension band wiring. Evaluation of the surgical results was done with the condition of pain, activity of daily living, range of motion, muscle tone by constant score system, and with preoperative, postoperative and last follow up radiographs.
RESULTS
Clinical evaluation was average 92 point by Constant score system from 84 point to 100 point. Subjective evaluation was 11 excellent (65%), 6 good (35%). Radiological evaluation was 9 excellent (54%), 6 good (38%), 2 fair (12%), and no poor group. On the final follow up, two cases showed inflammatory reaction at where pins were inserted, but after the removal of the pins, the inflammation was subsided.
CONCLUSION
The modified Phemister surgery for acromioclavicular dislocation is one of effective techniques, we can obtain firm fixation, exercise full range of motion early and there is no complication of re-dislocation.
- 665 View
- 0 Download
- Clinical and Functional Result after Internal Fixation of Severely Displaced Floating Shoulder
- Sang Hun Ko, Chang Hyuk Choe, Sung Do Cho, Jae Sung Seo, Jong Oh Kim, Jaedu Yu, Sang Jin Shin, In Ho Jeon, Kwang Hwan Jung, Jong Keun Woo, Ji Young Jeong, Gwon Jae No
- J Korean Fract Soc 2006;19(1):46-50. Published online January 31, 2006
- DOI: https://doi.org/10.12671/jkfs.2006.19.1.46
-
Abstract
- PURPOSE
To evaluate the follow-up result of 11 cases that were operated with internal fixation of scapular neck and internal fixation of clavicle or acromioclavicular dislocation for severely displaced floating shoulder which was high energy injury and unstable.
MATERIALS AND METHODS
We examined the scapular neck fracture with clavicle fracture or acromioclavicular joint dislocation by multidisciplinary research from August 1997 to July 2004. The scapular neck fractures were operated in the case of translational displacement of more than 25 mm and angular displacement of more than 45 degrees with 3.5 mm reconstruction plate fixation and internal fixation for clavicle fracture or acromioclavicular joint perpormed simultaneously. And we evaluated 11 cases that can be followed up for more than 9 months.
RESULTS
We achieved bony union in all cases. In ASES functional score, we got average 89.2 (75~95) points. In Rowe functional score, we got average 89.1 (75~100) points. In complication, there was external rotation weakness in 1 case.
CONCLUSION
In severely displaced floating shoulder due to high energy injury, we got good clinical and functional result after internal fixation for scapular neck and clavicle or acromioclavicular joint.
- 494 View
- 0 Download
- Result of Wolter Plate Fixation for the Treatment of Dislocation of Acromioclavicular Joint and Clinical Importance of Coracoclavicular Ligament Repair
- Jang Suk Choi, Ki Young Kim, Kyong Chil Chung, Heui Chul Gwak, Dong Jun Ha, Kyoung Whan Kim
- J Korean Fract Soc 2006;19(1):41-45. Published online January 31, 2006
- DOI: https://doi.org/10.12671/jkfs.2006.19.1.41
-
Abstract
- PURPOSE
To evaluate the clinical result of the Wolter plate fixation for the acromioclavicular joint dislocation and the necessity of coracoclavicular ligament repair with the operation.
MATERIALS AND METHODS
Twenty three patients operated between January 2003 to September 2005 with over 6 months of follow-up period were studied. The Constant-Murley scoring system was administered on 6 months postoperatively and stress films were taken for the surveillance of acromioclavicular joint and coracoclavicular distance after plate removal. All patients were classified into two groups in that coracoclavicular ligament was repaired (10 cases) or not (13 cases) and the clinical indices described above were compared.
RESULTS
With the Wolter plate fixation for the acromioclavicular joint dislocations, 20 cases of Constant-Murley scores were more than 'good' except complicated 3 cases. The scores of the repaired group were 7 cases of excellent, 2 cases of good and 1 case of moderate to poor, and that of not-repaired group were 6 cases, 5 cases and 2 cases respectively. With mean coracoclavicular interspace on x-ray at postoperative 6 months, repaired group showed residual 9% of displacement from initial 194% but not-repaired group showed 28% from initial 188%. There's no statistically significant difference in clinical scores between two group (p=0.072) and neither was residual coracoclavicular interspace displacement (p=0.067).
CONCLUSION
Short term follow-up of Wolter plate fixation for the acromioclavicular dislocation showed acceptable clinical results and there was no statistically significant difference between two groups of repaired coracoclavicular ligaments and not repaired.
- 477 View
- 0 Download
- Modified Phemister Technique with Mersilene Tape Augmentation in the Acute Acromioclavicular Joint Dislocation
- Hyun Dae Shin, Kwang Jin Rhee, Young Mo Kim, Kyung Cheon Kim, Choong Hui Lee
- J Korean Fract Soc 2005;18(2):83-88. Published online April 30, 2005
- DOI: https://doi.org/10.12671/jkfs.2005.18.2.83
-
Abstract
PDF
- PURPOSE
To find out the consequences of the surgical treatment of acromioclavicular joint dislocation, using modified Phemister technique with Mersilene tape augmentation.
MATERIALS AND METHODS
We chose 26 patients who were able to follow up 1 year or more among the patients who were diagnosed as acromioclavicular joint dislocation in our hospital through February 2001 to March 2003 and took modified Phemister surgery with Mersilene tape augmentation. Patients with clavicle fracture were excluded. Evaluation of the surgical results was done with the condition or pain, function, range of motion by using Imatani evaluation system, and preoperative, postoperative and last follow up radiographs.
RESULTS
Most of the cases showed satisfactory result. Clinical evaluations were 16 excellent (62%), 10 good (38%), radiological evaluations were 14 excellent (54%), 10 good (38%), 2 fair (8%), and no poor group. On the final follow up six cases showed vertical translation, but none had clinical symptoms. Seven cases showed a little inflammation at where pin were inserted, but after the removal of the pin, the inflammation was gone.
CONCLUSION
The modified Phemister surgery for acromioclavicle dislocation is simple, but we can obtain strong fixation, and there is no burden of the removal of the metal plate, or complication of re- dislocation after the removal of the pin, so it is thought as a very effective surgery.
- 670 View
- 4 Download
- The Treatment of Acromioclavicular Dislocation Comparison Study between Bosworth Screw and Wolter Plate Technique
- Jae Do Kang, Kwang Yul Kim, Hyung Chun Kim, Kyung Chil Jung, Mun Sup Lim, Jin Hyung Kim, Seong Joo Lee
- J Korean Soc Fract 2003;16(4):548-554. Published online October 31, 2003
- DOI: https://doi.org/10.12671/jksf.2003.16.4.548
-
Abstract
PDF
- PURPOSE
Acromioclavicular joint dislocation are frequently seen and various operation treatment modalities have been suggested. The purpose of this study is to compare the clinical results of two operative methods, Bosworth screw procedure and Wolter plate technique.
MATERIALS AND METHODS
We have analysed 30 patients with acromioclavicular dislocations, which had been treated by Bosworth screw & Wolter plate technique from June 1996 to February, 2002 with minimal 1 year follow up. All patients were assessed clinical and radiological results by ASES Score and UCLA Score.
RESULTS
Using the Shoulder evaluation scheme of ASES and UCLA Score at the one year follow up examination, 93.4% of the patients had excellent results in Wolter plate group. In Bosworth screw group, 4 complications such as loosening of the screw, or breakage of screw were seen. 2 complicated patients were over 40 years old and then conversions to Wolter plate operation was needed and obtained good results.
CONCLUSION
Bosworth procedure has a merit not to damage acromioclavicular joint, but the technique is difficult, sometimes may be encountered loss of fixation due to overcorrection and anterior displacement of the clavicle. However, Wolter plate implant provides enough stability for active postoperative physiotheraphy, and hence accelerates rehabilitation. Therefore, this technique is thought to be a good modality in the treatment of acute acromioclavicular seperation.
- 657 View
- 4 Download
- Comparison of Surgical Treatment for Acromioclavicular Joint Dislocation
- Tae Woo Park, Sung Do Cho, Yong Sun Cho, Bum Soo Kim, Sogu Lew, Jong Ken Woo
- J Korean Soc Fract 2002;15(1):59-64. Published online January 31, 2002
- DOI: https://doi.org/10.12671/jksf.2002.15.1.59
-
Abstract
PDF
- PURPOSE
To evaluate the result of modified Bosworth method augmented with Mersilene tape(MBM) compared with modified Bosworth method(MB).
MATERIALS AND METHODS
Thirty two acromiclavicular dislocation wrer treated with MB(15cares) or MBM(17 cases) and the mean follow up period was 26 months(12-43 months). We assessed the radiological and clinical evaluation(X-Ray & Weitzman Criteria) and complications.
RESULTS
Twenty nine cases(91%)(MB 13, MBM 16) were "excellent" or "good" according to the Weitzman criteria. At last follow-up, mean difference of the coracocalvialar distance between the normal and the injured site were 1.9mm(MB) and 1.6mm(MBM) and two ceses were developed the arthritis, and then performed the distal clavicle resection.
CONCLUSION
Modified Bosworth method augmented with Mersilene tape is a good option for acromioclavicular dislocation in stabilizing the joint, even if the screw loosening occurs with early postoperative ROM.
- 511 View
- 0 Download
- Modified Phemister Operation for Acromioclavicular Dislocation
- Jin Yung Park, Gun Nam Kim, Byung Sam Min, Moon Jib Yoo
- J Korean Soc Fract 2001;14(3):456-462. Published online July 31, 2001
- DOI: https://doi.org/10.12671/jksf.2001.14.3.456
-
Abstract
PDF
- PURPOSE
To evaluate the clinical results after modified Phemister operation for complete dislocation of acromioclavicular joint.
MATERIALS AND METHODS
Thirty-seven cases of Fifty-three cases complete dislocation of acromioclavicular joint which were treated modified Phemister operation, follow up for at least one year, were evaluated. After operation, applied Kenny-Howard brace for six weeks and removed the inserted pins at ten to twelve weeks postoperatively. The ROM exercise was started at postoperative six weeks and meticulous ROM exercise was begun at pin removal. The clinical results were evaluated with range of movement, comparision of the coracoclavicular distance after surgery with that of follow up, and complications.
RESULTS
The range of motion were forward elevation 150 degree, external rotation 71 degree, external rotation at 90 degree abduction 77 degree, and internal rotation T8. The comparision of coracoclavicular distance after surgery(0,6mm) with that of follow up(1.0mm) showed no significant ligament laxity. The complication were subluxation in 2 cases, heterotrophic calcification in 3cases, broken K-wire in 2cases, pin site infection in 7cases and distal clavicle osteolysis in 3cases, which were healed at follow up radiographically.
CONCLUSION
To prevent of redislocation of acromioclavicular joint, we tried to insert the pin during relatively long period for sufficient healing of ruptured coracoclavicular ligament. Although immobilization period was relatively long period, clinical results were good.
- 610 View
- 1 Download
Case Report
- Coracoid Process Fracture Associated with Acromioclayicular Dislocation and Partial Rupture of Coracoclavicular Ligament: A Case Report
- Seok Woong Yoon, Tae Sung Hwang, Byung Gue Park, Ki Hoon Kil
- J Korean Soc Fract 1999;12(3):693-697. Published online July 31, 1999
- DOI: https://doi.org/10.12671/jksf.1999.12.3.693
-
Abstract
PDF
- A coracoid process fracture associated with acromioclavicular dislocation has been reported infrequently. A coracoid process fracture associated with coracoclavicular ligament rupture has been reported only in two cases. Two separated injury mechanisms seem to be involved in this instance; one is direct trauma to the shoulder girdle causing dislocation of acromioclavicular joint, and the other is sudden avulsive pull on coracoid process by the conjoined tendons of short head of biceps brachialis and coracobrachialis, and pectoralis minor muscle causing fracture of the coracoid process. We reported one case of coracoid process fracture associated with acromioclavicular dislocation and partial rupture of coracoclavicular ligament. The lesion was treated by open reduction and interanl fixation using two Kirschner - wires for the acromioclavicular joint and a cortical screw for coracoid process, and the result was satisfactory without complication.
- 576 View
- 0 Download
Original Articles
- Treatment of Acute Acromioclavicular Dislocation with Modified Phemister Technique
- Myung Hwan Son, Byung Chul Kim, Nam Wook Kang, Tae Young Choi
- J Korean Soc Fract 1999;12(3):686-692. Published online July 31, 1999
- DOI: https://doi.org/10.12671/jksf.1999.12.3.686
-
Abstract
PDF
- There are various kinds of operative methods for the treatment of acute acromioclavicular dislocation but many complications such as posttraumatic arthritis, limitation of shoulder motion, and recurrence of dislocation would be developed. We have experienced 23 cases of acute acromioclavicular dislocation treated by modified Phemister technique from January 1992 to January 1997 and followed-up at least 1 year at Department of Orthopaedic Surgery, Pusan City Medical Center. The results were as follows: 1. The clinical results were evaluated by Weaver and Dunn were good in 19 cases, fair in 3 cases, poor in 1 case. 2. The radiological results were evaluated by the difference of the distance from the coracoid process to the clavicle between normal and injured site. The comparison of coraco-clavicular distance after surgery(1.76 mm) with that of follow up(2.41 mm) showed no significant difference(P>0.05, by Student t-test). 3. There was no posttraumatic arthritis and limitation of shoulder motion in all cases. So we suggest that modified Phemister technique is a good method for aute acromioclavicular dislocation.
- 505 View
- 0 Download
- AClinical Resutlt of Modified Phemister Method for Acute Acromioclavicular Dislocation
- Duk Yun Cho, Jae Hwa Kim, Kyung Chul Kim
- J Korean Soc Fract 1998;11(4):947-952. Published online October 31, 1998
- DOI: https://doi.org/10.12671/jksf.1998.11.4.947
-
Abstract
PDF
- There are many procedures for the treatment of acute A-C injury which have many complic ation such as limitation of shoulder motion, post traumatic arthritis and recurrence of dislocation etc. From July 1992 to June 1996 at National Medical Center, 21 patients with A-C injury had been treated by modified Phemister operation. The mean follow up time was 14.6 months. The following results are obtained. 1. There was no limitation of shoulder motion in 20 cases. 2. The comparison of coraco-clavicular distance after surgery ( 2.24 mm ) with that of fallow up ( 3.95 mm ) showed no significant difference. 3. Clinical resuls showed that good in 18 cases, fair in 2 cases, poor in 1 case. From the above result, we suggest that Modified Phemister method is simple and good procedure in the treatment of acute A-C dislocation.
- 441 View
- 0 Download
- Surgical Treatment of Acute acromioclavicular Dislocation
- Hyoun Oh Cho, Kyoung Duck Kwak, Byeung Yong Kim, su Min Sohn, Jin Kyoung Moon
- J Korean Soc Fract 1998;11(2):413-419. Published online April 30, 1998
- DOI: https://doi.org/10.12671/jksf.1998.11.2.413
-
Abstract
PDF
- We have reviewed 40 patients of acute acromioclavicular dislocation all treated by several operative procedure from January 1990 to July 1996. After about 12 months follow up period, we analyzed the relationship between the type of operation and the clinical results. Several operative mothods were demonstrated till now, but 4 techniques or their combinations are commonly used. Those are fixation of acromioclavicular joint, fixation of coracoclavicular ligament, resection of distal end of clavicle and dynamic muscle transfer. Modified Phemister technique, modified phemister technique with coracoclavicular fixation and modified Bosworth technique were used with or without repairment of coracoclavicular ligament at our hospital. Modified Phemister technique showed less good results than those of other techniques especially when repair of the coracoclavicular ligamentwas not made, and the repair of the coracoclavicular ligaments or fixation of the coracoclavicular joint is an important factor affecting the final results.
- 529 View
- 0 Download
- Results Following The Surgical Treatment of Acromioclavicular Joint dislocations; A Comparison of Phemister With Bosworth Operation
- Jin young Park, Suk Joo Lyu, Ki Hyuk Moon, Myung Ho Kim
- J Korean Soc Fract 1998;11(1):8-15. Published online January 31, 1998
- DOI: https://doi.org/10.12671/jksf.1998.11.1.8
-
Abstract
PDF
- To compare the results the Bosworth with Phemister operation, we performed the Bosworth operation in 7 case and then Phemister operation in 9 case serially from 1994 to 1997 and followed them up postoperatively. The average follow-up was 19.2 months, with the longest being 32 months, and the shortest being 12 months. The extraarticular coracoclavicular fixation was done with a cancellous screw in Bosworth operation, the transarticular fixation with two or three Kirschner wires in Phemister operation and the coracoclavicular ligaments were sutured to all patient in phemister operation group. The average immobilization period 6.8 weeks(S.D.:1.0 weeks) in Bosworth operation, 6.5 weeks(S.D.:1.4 weeks) in Phemister operation. The cancellous screw or the Kirschner wires were removed in 12.6 weeks(S.D.:1.6 weeks) postoperatively in Bosworth operation, 11.8 weeks(S.D.:1.7 weeks) in Phemister operation and physiotheraphy was progressed to obtain the full range of motion. All of the patients were evaluated on a subjective(pain, night pain, medication. instability, activities of daily living), objective(range of motion) and roentgenographic(degree of displacement) basis at last follow-up. Shoulder function was assessed according to the shoulder score devised by the American Shoulder and Elbow Surgeons. The pain of Shoulder persisted remained in 1 case of Bosworth operation and in 3 cases of Phemister operation. The night pain around acromioclavicular joint was remained in 2 cases of Phemister operation. Average shoulder function index in Bosworth operation was 95 points and in Phemister operation 87 points. Average range of motion of Bosworth operation was 176degree (S.D.:9degree in forward elevation, 68degree(S.D.:11degree in external rotation, 88.6degree(S.D.:12degree in cross-rotation at 90degreeabduction, 22cm (S.D.:11cm) in cross-body adduction and T9 in internal rotation and Phemister operation 147degree(S.D. 18degree in forward elevation, 72degree S.D.:12degree in external body adduction and T8 in internal ratation. All of the patients were satisfied for results of operation. After surgery, loss of reduction was found in 3 of 7 in Bosworth operation and all of the patients were over 40 years and then conversions to Phemister operation was needed. According to short-term follow-up we prefer the transarticular Phemister method and Bosworth operation may be avoided in patients over 40 yeras old.
- 543 View
- 0 Download
- Operative Treatment for Acromiclavicular Joint Dislocation
- Bum Soo Kim, Sung Do Cho, Ki Bong Kim
- J Korean Soc Fract 1998;11(1):1-7. Published online January 31, 1998
- DOI: https://doi.org/10.12671/jksf.1998.11.1.1
-
Abstract
PDF
- Acoromioclavicular dislocation occurs frequently in young athletes and recently in automobile accident victims and laborers, and there are various kinds of operative methods for this injury. Authors performed operative treatment for 45 cases of acromioclavicular dislocation: 30 cases of modified Phemister operation and 15 cases of modified Bosworth operation from March 1992 to June 1996. Authors analysed the result of the treatment and the results obtained were as follows. 1. The clinical results evaluated by Weitzman criteria were all satisfactory in both modified Phemister method and modified Bosworth method. 2. The radiologic results were evaluated by the difference of the distance from the coracoid process to the clavicle between the normal and the injured site. And the result was more satisfactory in modified Bosworth method. 3. There were less complications in modified Bosworth method.
- 608 View
- 1 Download
- Surgical Treatment of Acromioclayicular Joint Dislocation with Coracoclavicular Ligament Reconstruction using Coracoacromial Ligament
- Seung Rim Park, Hyoung Soo Kim, Joon Soon Kang, Woo Hyung Lee, Joo Hyung Lee, Min Seon Rim
- J Korean Soc Fract 1997;10(4):949-955. Published online October 31, 1997
- DOI: https://doi.org/10.12671/jksf.1997.10.4.949
-
Abstract
PDF
- Several treatment methods for complete acromioclavicular(AC) joint dislocation have been recommended. This study was performed to evaluate the results of the injuries that had been treated operatively with Bosworth technique combined with coracoclavicular ligament reconstruction using coiacoacromial ligament. Between September 1992 and October 1995, 19 cases were treated with this method. We made an assessment of the results suggested by Taft. Subjectively, fifteen patients had no pain or stiffness. 17 patients had normal strength and full range of motion objectively. On the roentgenographic bases, 16 cases showed normal findings and one showed the subluxation of the AC joint. The overall Taft score was 10.8 points and 84 % of the patients showed good or excellent results. The advantages of this method include anatomical reduction of the AC joint and early motion of shoulder. Ligament reconstruction enables early removal of the lag screw which precludes joint stiffness and metal problems. We conluded that this method was a good surgical method for complete AC joint dislocation.
- 545 View
- 0 Download
Comparative Study
- Treatment of Acromioclayicular Dislocation-Comparative Study between Operative and Conservative Method
- Young Su Lee, Min Ki Kim
- J Korean Soc Fract 1997;10(4):918-924. Published online October 31, 1997
- DOI: https://doi.org/10.12671/jksf.1997.10.4.918
-
Abstract
PDF
- There has been considerable controversy as to the method of treatment of acromioclavicular joint especially in grade III injury. We treated 27 cases of the complete dislocation of acromioclavicular dislocation with operative method(15 cases) and conservative method(12 cases) from October 1989 to November 1995. The purpose of this study is to compare the clinical and radiological result of two treatment method. The average follow up period was thirty nine months and the result as follows. 1. Of the 27 cases, there was 18 male and 9 female patients, and peak incidence was in 3rd and 4th decades(51%). 2. The most common causes of the injury was traffic atcident(49%). 3. The functional results were similiar to all treatment modalities, and coracoclavicular interval ratio was well manintained regardless of treatment. 4. Complication rate was more lower in the group of conservative treatment. 5. The conservative treatment was proven to be a valuable method for acromioclavicular dis- location except in a few situations.
- 491 View
- 0 Download
Original Article
- Fracture of the Coracoid Process Associated with Acromioclavicular Dislocation
- Ui Seoung Yoon, Yong Hoon Kim, Keun Woo Kim, Hak Jin Min, Kook Hyeung Cho, Ki Seung Kum, Il Myung Kim
- J Korean Soc Fract 1997;10(3):640-644. Published online July 31, 1997
- DOI: https://doi.org/10.12671/jksf.1997.10.3.640
-
Abstract
PDF
- Acromioclavicular dislocation with a concomitant coracoid process fracture occurs infrequently, as only several cases have been reported in the literature. This injury usually occurs in the second or third decade of life. The mechanism of injury were sports, motor vehicle and direct trauma. An axillary lateral radiograph of the shoulder often is needed to detect this fracture. The authors present two cases of coracoid process fracture associated with acromioclavicular dislocation. Satisfactory function with minimal residual cosmetic deformity may be achieved by nonoperative measures. Also surgical treatment can produce good result in complete third acromioclavicular separation combined with the significantly displaced coracoid fracture.
- 569 View
- 5 Download
Case Report
- Fracture of the Coracoid Process
- Sung Ho Hahn, Bo Kyu Yang, Chi Hong Kim, Tae Won Ahn, Dong Hyun Kim
- J Korean Soc Fract 1996;9(4):1085-1089. Published online October 31, 1996
- DOI: https://doi.org/10.12671/jksf.1996.9.4.1085
-
Abstract
PDF
- Fractures of the coracoid process arf rare and those associated with a complete acromioclavicular separation and clavicular shaft fracture are even more rare. The mechanism of injury may be by direct trauma or by avulsion when there is sudden and violent contraction of the biceps, corachobrachilalis, and pectoralis minor muscle. The fracture occurs most commonly through the base. Conservative treatment can produce good result. Unusually open reduction is indicated for marked displacement associating acromioclavicular dissociation or compiession of the brahial plexus. The authors report 2 cases of coracoid process fracture. one case combined with acromioclavicular separation and the other with fracture of clavicular mid shaft.
- 550 View
- 0 Download
Original Articles
- Treatment with bone block transfer of coracoacromial ligment in acromioclayicular injury
- Byung Chang Lee, Sang Soo Kim, Dae Moo Shim, Sang Do Cha
- J Korean Soc Fract 1996;9(1):146-153. Published online January 31, 1996
- DOI: https://doi.org/10.12671/jksf.1996.9.1.146
-
Abstract
PDF
- Several studies have shown the effectiveness of reconstruction of acromioclavicular ligament with coracoacromial ligament in treating the Grade III acromioclavicular joint injury. One of these is a bone block transfer of coracoacromial ligament into the medullary canal of the clavicle to prevent occasional pullout of the transfered ligament. Eleven cases with complete acromioclavicular dislocation(acute 3, chronic 8) were treated by this method. We modified slightly the original method described by Shoji et at. to increase the success rate. Failure of coracoclavicular reconstruction occurred in two cases. All except one patient regained nearly painlefs range of shoulder motion. One patient showed severe restriction of shoulder abduction and definite deformity. In functional evaluation by the Weitzman criteria, five were excellent, four good, one fair, and one poor. Radiologic results for restoration of coracoclavicular interval showed marked improvement but were not consistent with clinical results. Main technical problems were harvesting bone block and fixation of ligament. To obtain good osseus healing without pull out of transferred ligament, we found that preservation of bone ligament junction and careful harvest of full thickness acromiai bone block was important.
- 488 View
- 0 Download
- The Treatment of Acromioclayicular Dislocation Comparison Study between Modified Bosworth and Phemister Technique
- Kun Yung Lee, Myung Sik Park, Keun Kwon Kang, Myung Kon Nami
- J Korean Soc Fract 1995;8(1):193-198. Published online January 31, 1995
- DOI: https://doi.org/10.12671/jksf.1995.8.1.193
-
Abstract
PDF
- Acromioclavicular joint injuries are frequently seen with increase of traffic & industrial accidents & sports injury recently, There are many procedures which described for the treatment of acromioclavicular dislocation, but there are still controversies concerning the best treatment of the injuries. We have analysed 35 patients with acromioclavicular dislocations had been treated by modified Bosworth & Phemister technique at the department of orthopedic surgery Lee-Rha general hospital from June 1990 to December 1993 with minimal 1 year foll up The authors had obtained following results as modified Phemister technique and modified Bosworth technique treatment for acromioclavicular joint. 1. The complications were as follows: superficial infection at insertion site of k-wire and migration of k-wire in modified Phemister technique and loosening of screw and erosion of clavicle noted in modified Bosworth tecnique. But, there were no specific difference between two groups for pain and motion of shoulder joint. 2. In modified Bosworth technique, it was not necessary to fix the acromioclvicular joint with k-wire and also possible to perform early mobilization of shoulder joint than modified Phemister tecnique.
- 507 View
- 0 Download
- Surigcal Treatment for Acute Acromioclayicular Joint Dislocation
- Nam Yong Choi, In Ju Lee, Moon Ku Choi, Young Chae Lee, Han Jin Kim, Chong Ook Shin
- J Korean Soc Fract 1995;8(1):188-192. Published online January 31, 1995
- DOI: https://doi.org/10.12671/jksf.1995.8.1.188
-
Abstract
PDF
- Thirty-one patients who had a acromioclavicular joint dislocation that were treated by surgical operation, between January 1990 and December 1993 at St. Pauls & Holy Family hospital were analyzed. The results are as follows; 1. There were twenty-five males and six females. The mean age was 33 years, ranging from 17 to 52 years old. 2. Out of thirty-one cases, twenty-six had good to excellent functional results. 3. As regards complication, wire migration occurred in two cases, wire breakage in one case, screw loosening in one, and subluxation following wire or screw removal in four.
- 491 View
- 0 Download
- A clinical study of acromioclavicular separation treated withoperative method
- Yong Chan Lim, Jong Oh Kim, Taek Keun Ahn, Taek Sun Kim, Jae Ik Shim
- J Korean Soc Fract 1992;5(1):7-13. Published online May 31, 1992
- DOI: https://doi.org/10.12671/jksf.1992.5.1.7
- 504 View
- 0 Download
- Treatment of acute acromioclavicular dislocation with percutaneous pinning
- Hyoung Min Kim, Choong Seo Park, Youn Soo Kim, Jae Duk Ryu
- J Korean Soc Fract 1992;5(1):28-36. Published online May 31, 1992
- DOI: https://doi.org/10.12671/jksf.1992.5.1.28
- 459 View
- 1 Download
- Acromioclavicular dislocation treated by weaver and drum operation
- Dae Yong Han, Yeo Hon Yun, Jin Soo Park
- J Korean Soc Fract 1992;5(1):14-21. Published online May 31, 1992
- DOI: https://doi.org/10.12671/jksf.1992.5.1.14
- 465 View
- 0 Download
- The conservative treatment of acromioclaviclar dislocation
- Jae Do Kim, Jae Chang Lee, Kyu Yong Lee, Tae Jin Kim
- J Korean Soc Fract 1992;5(1):1-6. Published online May 31, 1992
- DOI: https://doi.org/10.12671/jksf.1992.5.1.1
- 543 View
- 1 Download
- Treatment of the Complete Separation of Acromioclavicular Joint by Coracoclavicular Wiring
- Chang Uk Choi, Yon Il Kim, Young Ho Kim, Min Ku Lee
- J Korean Soc Fract 1990;3(1):119-126. Published online May 31, 1990
- DOI: https://doi.org/10.12671/jksf.1990.3.1.119
-
Abstract
PDF
- Complete dislocation of the acromioclavicular joint is not a common jnjury. But there are many methods of treating for complete separation of acromioclavicular joint. From February, 1988 to March, 1989 at Soonshunyang university hospital, 14 pateints with complete acromioclavicular separation(Allmans type3) had been treated sugically by coraco-clavicular wiring. The results are follows. 1) The most common cause of injury is fraffic accident. 2) Ages in peak incidence are 3rd and 4th decades. 3) The shoulder pain and the limitation of external rotation, which are well known problem of transacromioclavicular fixation cant be found and the functional result were excellent in 12 cases good in 1 case and fair 1 case 4) We consider that over reduction and anatomical reduction of acromioclavicular joint may be prevent complications and obtain excellent results. 5) We can Prevent the anterior displacement of clvicle from the acromion and bony erosion by passing the wire loop through the drill hole on the center of clavicle which direction is from superior to inferior portion.
- 575 View
- 0 Download
- Complication Folloing Operative Treatment in Complete Acromioclavicular Joint Dislocation
- Sung Kwan Hwang, Jae In Ahn, Heui Jeon Park, Zi Hoan Cha
- J Korean Soc Fract 1988;1(1):64-70. Published online November 30, 1988
- DOI: https://doi.org/10.12671/jksf.1988.1.1.64
-
Abstract
PDF
- The conservative treatment such as plinting, bandaging and harnessing in the partial disrupton of the acromioclavicular joint(Grade II or less) has been successuful, but many surgeons prefer to operative treaments for complete A-C dislocation(Grade III). Though more than 55 operative methods of treatment were reported in the literature, they could be divided into four categories: 1) acromioclar reduction and acromioclavicular fixation, 2) acromicoclavicular reduction, coracoclavicular ligament repair, and coracoclavicular fixation, 3) distal clavicle excision, and 4) muscle transfers. Among numerous operative methods, we used Weaver-Dunn technic, A-O tension Band technic, and Modified bosworth technic in total 28 cases of complete A-C dislocation from March 1984 to June 1988 at the Yonsei University Wonju College of Medicine, Wonju Christian Hospital. In most cases, excellent or good results were obtained, but we stillfound swveral postperative complications. We experienced neither deep wound infection nor osteomyelitis. All 6 cases had fixation-related complications. After close examination of operation notes and X-rays, following suggestions were considered. 1. Reduce every A-C joint anatomically before inserting K-wires through A-C joints. 2. Start shoulder motion several days after operation to provide enough time form healing of deltoid and trapezius muscles. 3. Surgenous play a major role to prevent commplications such as malposition of fixatives and incomplete A-C joint reduction
- 517 View
- 0 Download
 First
First Prev
Prev

