 E-submission
E-submission TOTA
TOTA TOTS
TOTS
Articles
- Page Path
- HOME > J Musculoskelet Trauma > Volume 35(4); 2022 > Article
- Review Article Treatment of Scaphoid Fractures and Nonunions
- Wan-Sun Choi
-
Journal of Musculoskeletal Trauma 2022;35(4):182-189.
DOI: https://doi.org/10.12671/jkfs.2022.35.4.182
Published online: October 31, 2022
Department of Orthopaedic Surgery, Ajou University School of Medicine, Suwon, Korea
- 1,356 Views
- 9 Download
- 0 Crossref
- 0 Scopus
Abstract
A scaphoid fracture is one of the most common types of wrist fractures, and if treatment is delayed, there is a high possibility of nonunion due to anatomical factors such as limited blood supply to the injured bone. Therefore, it is important to suspect a scaphoid fracture based on the mechanism of wrist injury and physical examination of the patient. A computed tomography scan or magnetic resonance imaging can also aid early diagnosis of the fracture. Stable acute fractures can be treated conservatively, but unstable fractures require surgical treatment, and percutaneous screw fixation is usually performed. Nonunions require bone grafts and are treated with non-vascularized bone grafts and screw fixation. However, if the nonunion is located at the proximal pole, a vascularized bone graft may be considered because there is a possibility of avascular necrosis. Pedicled vascularized and free vascularized medial femoral condyle bone grafts are mainly used in such cases. The treatment of a proximal pole nonunion with impaired blood flow remains controversial. There are conflicting opinions on whether a nonvascularized bone graft is sufficient or whether a vascularized bone graft is necessary.
J Korean Fract Soc. 2022 Oct;35(4):182-189. Korean.
Published online Oct 20, 2022.
https://doi.org/10.12671/jkfs.2022.35.4.182
Published online Oct 20, 2022.
https://doi.org/10.12671/jkfs.2022.35.4.182
Copyright © 2022 The Korean Fracture Society.
Review
주상골 골절 및 불유합의 치료
Treatment of Scaphoid Fractures and Nonunions
Wan-Sun Choi , M.D., Ph.D.
, M.D., Ph.D.
, M.D., Ph.D.
초록
주상골 골절은 흔한 손목 골절 중의 하나이며, 제한된 혈류 공급 등의 해부학적 특징으로 인해 치료가 늦어지면 불유합이 잘 발생한다. 따라서 손목 손상 환자의 손상 기전과 병력 청취, 이학적 검사를 통해서 주상골 골절을 의심할 수 있어야 하고, CT나 MRI를 통해 초기에 정확히 진단해야 한다. 안정성 급성 골절은 보존적 치료가 가능하지만 불안정성 급성 골절은 수술적 치료가 필요하며 주로 경피적 나사못 고정술을 시행한다. 불유합의 경우는 골이식이 필요하며 주로 비혈관화 골이식과 나사못 고정술로 치료한다. 그러나 불유합의 위치가 근위극에 있을 경우 무혈성 괴사의 가능성이 있으므로 혈관화 골이식이 고려되기도 한다. 혈관화 골이식으로는 유경 혈관화 골이식과 대퇴골 내과 유리 골편 이식술 등이 주로 쓰인다. 혈류 장해가 동반된 근위극 불유합에 대한 치료는 아직 논쟁의 여지가 있는데 비혈관화 골이식으로 충분하다는 의견과 혈관화 골이식이 필요하다는 의견이 맞서고 있다.
Abstract
A scaphoid fracture is one of the most common types of wrist fractures, and if treatment is delayed, there is a high possibility of nonunion due to anatomical factors such as limited blood supply to the injured bone. Therefore, it is important to suspect a scaphoid fracture based on the mechanism of wrist injury and physical examination of the patient. A computed tomography scan or magnetic resonance imaging can also aid early diagnosis of the fracture. Stable acute fractures can be treated conservatively, but unstable fractures require surgical treatment, and percutaneous screw fixation is usually performed. Nonunions require bone grafts and are treated with non-vascularized bone grafts and screw fixation. However, if the nonunion is located at the proximal pole, a vascularized bone graft may be considered because there is a possibility of avascular necrosis. Pedicled vascularized and free vascularized medial femoral condyle bone grafts are mainly used in such cases. The treatment of a proximal pole nonunion with impaired blood flow remains controversial. There are conflicting opinions on whether a non-vascularized bone graft is sufficient or whether a vascularized bone graft is necessary.
Keywords
Scaphoid bone, Fractures, Ununited, Treatment, Surgery
주상골, 골절, 불유합, 치료, 수술
서론
주상골은 손목 부위에서 원위 요골 다음으로 골절이 흔하게 발생하는 뼈이다.1) 손목을 강하게 신전할 때 충격이 전달되기 쉬운 해부학적 형태와 위치를 갖기 때문이다. 주상골 골절은 흔하게 발생함에도 불구하고 초기에 진단을 놓치는 경우가 많다. 복잡한 모양 탓에 단순 방사선 영상을 다양한 각도로 면밀하게 관찰하지 않으면 골절을 놓칠 수 있다. 또한 주상골은 해부학적으로 혈액 공급이 충분하지 않아서 골절을 적절하게 치료하지 않으면 불유합이 발생할 가능성이 높다.2) 불유합은 심각한 합병증을 일으킬 수 있으므로 조기 진단과 치료가 매우 중요하다. 따라서 본 종설에서는 주상골 골절을 적극적으로 치료해야 하는 이유를 주상골의 해부학적 특징과 골절의 자연적 경과를 통해 알아보고, 급성 골절과 불유합의 진단 및 치료에 대해서 살펴보고자 한다.
불유합이 흔한 이유
대부분의 골절은 손상 부위가 구조적으로 안정되고 혈류 공급이 충분할 때 유합이 잘 이뤄진다. 그러나 주상골은 이 두 가지 측면에서 모두 취약할 수 있다. 우선, 구조적으로 주상골은 주위의 수근골 및 요골과 5개의 관절을 이루고 있고 손목 관절의 움직임 시 관절면을 통해 불규칙적인 외력을 전달받는다. 외력은 골절편의 전위를 유발할 수 있다. 주상골의 모양은 ‘ㄱ’형으로 종적인 힘(axial force)이 가해질 때 굴곡 변형이 되려는 경향이 크다.3) 이러한 구조적 특징들로 인해 적절한 고정과 보호가 없으면 골절 부위의 안정성을 유지하기 어렵다.
주상골의 혈류 공급 또한 매우 특징적이어서 골유합의 취약점이 될 수 있다. 주상골은 표면적의 70% 이상이 연골로 덮여 있기 때문에 혈관이 뼈 안으로 들어올 수 있는 공간이 제한되어 있다.3) Gelberman과 Menon2)이 1980년에 발표한 주상골의 혈류 공급에 대한 연구에 따르면, 요골 동맥으로부터 분지된 혈관이 역행적으로 주행하여 주상골 배부능(dorsal ridge)을 통해 뼈 안으로 들어와 근위부 70%-80%의 혈류 공급을 담당한다. 이 혈관이 골절 때문에 손상되면 근위극(proximal pole) 부위의 불유합 및 무혈성 괴사가 잘 발생한다. 반면에 원위부는 원위 결절(distal tuberosity)의 수장 측에서 혈관이 안으로 들어와 원위부 20%-30%의 혈류 공급을 담당한다.2) 미세 컴퓨터 단층촬영(micro-computed tomography [CT])을 이용한 최근의 주상골 혈관 연구에 따르면 주상골 허리(waist) 부위의 배부능에서 2개 이상의 체간 동맥(trunk artery)이 뼈 안으로 들어와 혈류 공급을 한다. Gelberman과 Menon2)의 연구와는 달리 배부능의 체간 동맥에서 연결된 골내 미세 혈관들이 허리 부위 및 근위부뿐만 아니라 원위부에도 주된 혈류 공급을 한다. 또한 가장 근위부체간 동맥의 평균적인 위치가 근위부의 42%에 위치하여 근위부 40% 내에 골절이 생길 경우 심각한 혈류 장해가 발생할 수 있다.4)
골절의 자연 경과 및 합병증
주상골 골절이 임상적으로 주목받는 이유는 초기 진단과 치료를 놓치게 되면 불유합이 흔하게 발생하기 때문이다. 그러나 역설적으로 증상이 그리 심하지 않아 모른 채로 지내다가 급성기가 훨씬 지난 후에 불유합으로 진단되는 경우도 많다. 실제 치료 받지 않은 주상골 불유합 환자의 자연 경과를 조사한 연구에서는 대부분의 환자가 보통(fair) 또는 좋음(good) 등급 이상의 임상 결과를 보였고 추가적인 수술 치료를 원하지 않았다.5) 그러나 환자의 대부분이 손목 관절운동 범위와 파지력(grip strength)이 줄었고 영상 검사상으로 퇴행성 관절염이 발생하였다.5) 조기에 진단과 치료를 받지 않은 주상골 골절은 약 12%에서 불유합으로 진행한다.6) 불유합은 연쇄적으로 수근 붕괴(scaphoid non-union induced carpal collapse, SNAC)를 초래할 수 있다.7) 불유합의 초기에는 증상이 미약할 수 있으나 종국에는 예상치 못한 심각한 관절염을 유발할 수 있으므로 손상된 주상골을 해부학적으로 복원하는 것이 중요하다.
주상골 골절 이후에 발생하는 근위극의 무혈성 괴사도 중요한 이슈 중의 하나이다. 해부학적으로 근위부 혈류 공급은 골내 혈관망을 통해서만 이루어지므로 골절로 인해 근위부의 혈류 공급이 차단될 수 있다. 따라서 많은 연구들에서 근위극의 혈류 상태(vascularity)는 주상골 불유합의 치료 성공과 연관된 인자로 언급되었다.8,9,10) 그러나 최근 Rancy 등11)은 수술 전 주상골 근위부의 자기공명영상(magnetic resonance imaging, MRI) 검사 소견과 수술 중 점상 출혈(punctate bleeding) 여부, 수술 후 조직학적 검사의 불일치성을 지적하며 근위부의 혈류상태와 불유합 수술의 성공 여부는 연관성이 적다고 하였다.
주상골 불유합으로 발생하는 굴곡변형(humpback deformity)은 수근 불안정성(carpal instability)을 유발할 수 있다. 이론적으로 굴곡변형은 삼각골의 신전 모멘텀(momentum)과 균형을 이루고 있던 주상골의 굴곡 모멘텀을 약화시켜 근위 수근열의 신전을 유발한다. 이로 인해 배측 수근골간 분절 불안정성(dorsal intercalated segmental instability, DISI)이 발생한다(Fig. 1).12,13) 따라서 주상골 불유합 치료 시에 골이식을 통해 주상골의 굴곡 및 단축 변형을 교정해야만 DISI를 회복시킬 수 있다.14)
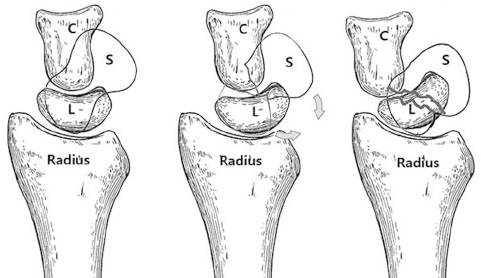
Fig. 1
DISI (dorsal intercalated segment instability) caused by the humpback deformity of the scaphoid nonunion (C: capitate, L: lunate, S: scaphoid).
분류
주상골 골절의 분류로는 해부학적 위치에 따라 구분하는 Russe 분류,15) Mayo 분류와 골절의 안정성을 기준으로 하는 Herbert 분류16)가 가장 널리 쓰인다. 이 중 Herbert 분류는 보존적 치료와 수술적 치료를 결정하는 데에 중요한 참고가 될 수 있다(Table 1). 결절(tubercle) 골절과 허리부의 불완전 골절은 안정형 골절인 A형에 해당하므로 보존적 치료가 가능하나, B형, C형, D형은 불안정형 골절 또는 지연유합, 불유합 골절이기 때문에 수술적 치료가 필요하다.
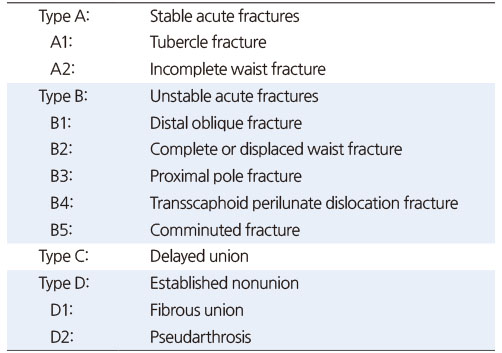
Table 1
Herbert and Fisher Classification of Scaphoid Fractures
진단
영상 검사를 시행하기 이전에는 환자의 병력과 손상기전, 이학적 검사로 주상골 골절 여부를 의심하는 것이 중요하다. 주로 젊은 나이(15-40세)의 환자가 손목이 과신전 및 요측 편위(radial deviation)되는 손상을 입은 경우 잘 발생할 수 있다. 이학적 검사로는 수장측의 주상골 결절부와 anatomical snuff box의 압통을 확인한다. 손목 관절운동 범위가 감소할 수 있고, 엄지의 움직임 또는 손목의 요측 편위 시에 통증을 호소할 수 있다. 그러나 앞서 언급하였듯이 주상골 골절의 증상 자체가 미미한 경우가 많아 이학적 검사의 특이도(specificity, true-negative rate)는 74%-80% 정도 수준이다.17,18) 주상골 손상이 의심된다면 단순 영상 검사로서 손목의 전후면 및 양측 사면 검사와 함께 손목을 척측으로 기울여 촬영하는 주상골면(scaphoid view)도 확인해야 한다. 그러나 단순 영상 검사도 최대 25%까지 위음성(false-negative)을 보일 수 있으므로19) CT나 MRI 검사와 같은 추가 검사가 필요하다. MRI는 민감도와 특이도가 거의 100%에 가까울 정도로 정확한 진단이 가능하며 인대와 같은 다른 구조물의 손상 여부와 주상골의 혈류 상태를 파악할 수 있다.19) CT는 3차원 복원이 쉽기 때문에 변형이 심한 급성 골절 및 불유합의 수술 전 계획을 세우는 데 유용하며 수술 후 추적 관찰 중에 골유합 여부를 확인하는 데에도 쓰인다. 이 외에 골주사 검사(bone scan)20)와 초음파 검사21)도 진단을 위해 쓰일 수 있다.
급성 주상골 골절의 치료
주상골 골절에 대한 치료는 크게 급성기 골절의 치료와 그 이후의 치료로 구분할 수 있다. 보통 수상 후 4주 이전에 치료가 이루어지면 3% 정도의 불유합이 발생하고, 그 이후에 치료하게 되면 최대 40%의 빈도로 불유합이 발생할 수 있다.22) 골절의 형태와 불안정성 등 여러 요인을 고려하여 수술 방법을 선택해야 하겠지만, 치료의 시기만을 고려했을 때는 4주 이후에 발견된 골절에 대해서는 지연 유합과 불유합의 가능성을 염두에 두고 골이식이 필요할 수 있다. 영상 검사상으로 완전한 불유합이 확인된 경우는 반드시 골이식이 필요하며 변형된 주상골의 모양을 복원하는 노력도 기울여야 한다.
1. 보존적 치료
주상골의 원위극(distal pole)과 허리 부위의 비전위성 골절, 수근 불안정성을 동반하지 않으면서 1 mm 이내의 전위가 있는 골절은 보존적 치료가 가능하다.23,24) Herbert 분류의 A형도 여기에 해당한다. 보존적 치료 시에 고정의 범위가 손목만인지 아니면 주관절까지 포함해야 하는지에 대해서는 논쟁이 있었다. 기존의 무작위 대조 연구(randomized controlled trial)들을 대상으로 한 메타분석 및 체계적 문헌고찰에서는 고정 범위와 치료 결과는 연관성이 없었다.25) 무지의 고정도 반드시 필요하지 않다는 연구도 보고되었다.26) 고정기간은 약 6-12주 정도이고 정기적으로 골유합 여부를 확인하여 석고 붕대의 제거 시기를 결정한다. 최근 연구에서는 안정형 골절에 대해서도 보존적 치료 대신에 초기에 수술하는 것이 비용을 절감하고 고정기간을 단축시키며 직장으로의 복귀를 앞당길 수 있다고 하였다.27)
2. 수술적 치료
보존적 치료의 적응증이 되지 않는 골절은 모두 수술적 치료의 대상이 된다. 급성기 골절에서는 주로 경피적 나사못 고정술이 사용되는데, 나사못의 삽입 방향에 따라 수장 접근법(volar approach)28)과 배부 접근법(dorsal approach)29)으로 구분된다. 수장 접근법은 겉에서도 잘 만져지는 주상골의 결절 부위에 나사못을 삽입하므로 술기가 쉽고 손목을 신전한 상태에서 수술하기 때문에 굴곡 전위된 골절 부위를 정복하면서 나사못을 삽입할 수 있는 장점이 있다. 단점으로는 주상골의 원위부와 관절을 이루는 대능형골이 나사못이 들어가는 부위를 막아서 나사못의 삽입 위치가 수장측 표면에 가까울 수밖에 없고, 이로 인해 주상골의 중심축에 나사못을 위치시키기 어렵다. 또한 근위부의 골편을 충분한 길이로 관통하지 못하여 고정이 불안정할 수 있다. 배부 접근법은 주상골의 중심축에 나사못을 위치시킬 수 있어 견고한 고정을 할 수 있다. 중심축에 가까울수록 골내 혈관망의 손상도 적어 골유합에도 유리한 장점도 있다.30) 또한 근위극부터 나사못이 통과하므로 수장 접근과 달리 근위골편을 보다 견고하게 고정할 수 있다. 그러나 나사못을 삽입하는 동안 손목을 굴곡시켜야 하므로 골절의 전위가 더 심해질 수 있는 단점이 있다.
전위가 심하지 않은 골절은 대부분 도수 정복 및 경피적 나사못 고정술로 치료할 수 있다. 그러나 전위가 심하고 불안정한 골절은 관혈적 정복이 필요할 수 있다. 특히 월상골 주위 손상과 동반된 주상골 골절은 월상골의 탈구와 함께 골절편이 전위되어 도수 정복이 어려울 수 있다. 이런 경우 관혈적으로 월상골 탈구와 주상골 골절을 정복하고 손상된 수근골간 인대는 봉합한다.31,32,33)
최근에는 관절경을 이용한 최소 침습적 수술이 널리 보급되면서 전위성 골절을 관절경 보조하에 정복하고 경피적 나사못 고정을 하는 술식도 보고되었다.34,35) 관절경 보조 술식은 주상골의 변형이 심하지 않은 불유합 골절에서도 사용될 수 있다. 관절경 술식의 장점은 최소 침습적이기 때문에 주상골 주위 혈관 손상을 줄일 수 있고, 동반된 연부조직 손상을 평가하여 함께 치료할 수 있다.35)
주상골 불유합의 치료
주상골 불유합은 초기 증상이 미미할지 몰라도 종국에는 관절염과 SNAC를 초래한다. 따라서 적극적인 치료가 필요하며, 치료의 목표는 골절의 유합과 해부학적 형태의 복원이다. 불유합에 대한 보존적 치료는 골절의 유합보다는 증상 완화에 초점을 둔다. 따라서 궁극적인 치료는 수술이며 골이식이 항상 필요하다. 골이식은 종류에 따라 비혈관화 골이식(non-vascularized bone graft)과 혈관화 골이식(vascularized bone graft)으로 구분할 수 있다.
1. 비혈관화 골이식
비혈관화 골이식은 가장 흔하게 쓰이는 방법이며 주로 자가 장골(autogenous iliac bone)이나 자가 원위 요골을 사용한다. Matti-Russe 술식15)과 Fernandez 술식36)이 가장 고전적인 방법으로 이것을 변형한 다양한 술식들이 쓰인다. Matti-Russe 술식은 수장측 접근으로 불유합 부위를 노출한 뒤 소파술을 시행하여 근위 및 원위 골편 안에 공간을 만들고 이곳에 막대 형태의 피질-해면골을 이식하는 방법이다. Fernandez 술식은 소파술 후 쐐기 형태의 피질-해면골을 이식하여 주상골의 굴곡 변형을 교정하는 방법이다. 불유합 부위의 골경화(sclerosis)와 낭종(bone cystic)은 소파술로 제거한다. 소파술은 점상 출혈이 확인될 때까지 충분히 시행하는 것이 좋다. 골이식 후에는 유관 나사나 K-강선으로 고정한다(Fig. 2). 유관 나사로 좀 더 견고한 고정을 할 수 있으나 근위골편이 작아서 충분히 관통하지 못하는 경우는 K-강선으로 고정한다.37) 주상골 허리 부위보다 원위부의 불유합은 대부분 이와 같은 비혈관화 골이식으로 좋은 결과를 얻을 수 있다.9) 그러나 무혈성 괴사가 동반될 수 있는 근위극 불유합의 경우는 치료가 어려울 수 있다.

Fig. 2
(A) A 15-year-old male had a scaphoid nonunion in his right wrist, computed tomography showed a severe humpback deformity of the scaphoid. (B) During the operation, the scaphoid waist showed pseudarthrosis. After sufficient curettage, a wedge strut bone graft was placed in the area of pseudarthrosis. (C) A cannulated screw was used for fixation. (D) Lateral radiographs of the right wrist showed a slight recovery of the DISI deformity after surgery.
2. 혈관화 골이식
근위극 무혈성 괴사에 대한 우려로 여러 가지 혈관화 골이식술이 보고되었다. 그 중 대표적인 술식은 Zaidemberg 등이 처음 보고한 1,2-intercompartmental supraretinacular artery (ICSRA) 혈관경 골이식38)과 원위 대퇴골 내과 유리 혈관화 골이식(free medial femoral condyle vascularized bone graft, free MFC-VBG)39) 등이 있다. 1,2-ICSRA 술식은 우선 손목의 후외측으로 접근하여 주상골 불유합 부위를 노출한 뒤 소파술을 시행한다. 이후 1, 2 신전 구획 사이를 지나가는 혈관을 찾아 주변 조직과 함께 박리하고 원위 요골과 연결된 부위에서 이식 골편을 혈관경과 함께 거상한다. 골편을 불유합 위치로 옮긴 후 K-강선이나 유경 나사로 고정한다(Fig. 3).40) Free MFC-VBG는 수장측으로 주상골에 접근하여 소파술을 시행한 후 대퇴 내과에서 descending genicular artery를 혈관경으로 하는 골편을 거상한다. 혈관을 끊기 전에 골편에 출혈이 잘 되는 것을 확인한다. 불유합 부위에 이식골을 넣을 때는 혈관경이 부착된 피질골이 수장측으로 향하게 놓아 혈관이 꼬이지 않게 한다. 혈관 문합은 요골 동맥에 end-to-side로 연결하고 정맥은 vena comitans나 cephalic vein과 end-to-end로 연결한다.41)

Fig. 3
(A) Computed tomography showed a large cystic lesion in the proximal pole and severe humpback deformity. (B) Considering the vascular impairment in the proximal pole, a 1,2-ICSRA (1,2 intercompartmental supraretinacular artery) pedicled vascularized bone graft was performed. (C) Bone union was achieved, but the deformity remained.
3. 근위극 불유합의 치료에 관한 논쟁
근위극은 골내 혈류 공급에만 의존하므로 골절로 인해 골내 혈관망이 손상되면 무혈성 괴사가 발생할 수 있다. 불유합의 위치가 근위극에 있더라도 무혈성 괴사가 없으면 비혈관화 골이식만으로도 좋은 결과를 얻을 수 있다.42) 그러나 골괴사가 있는 경우는 논쟁의 여지가 있다. 과거의 연구에서는 주상골 근위극의 혈류 상태가 불유합 골절 치료의 성공 여부를 결정하는 중요한 요인이 된다고 하였다.9,15) 최근에도 이와 같은 맥락으로 근위극의 무혈성 괴사는 비혈관화 골이식의 금기라고 여기는 연구자들도 많다.40,43,44) 그러나 Rancy 등45)은 체계적 문헌고찰 연구에서 비혈관화 골이식과 혈관화 골이식의 결과가 유의미한 차이가 있다는 주장은 현재까지 증거가 없다고 하였다. 또한 자신의 증례군 연구에서 주상골 불유합의 근위 골편을 MRI와 점상 출혈 여부, 조직학적으로 분석하였을 때 심각한 혈류 장해가 있음에도 불구하고 비혈관화 골이식만으로 충분히 골유합이 되었다고 하였다.11) 이 외에도 근위극 불유합에 대해서 비혈관 골이식의 좋은 결과를 보고한 연구들은 많다.46,47,48) 그러나 최근 Mayo group의 연구에 따르면 비혈관화 골이식과 1,2-ICSRA pedicle 골이식, free MFC-VBG를 비교하였을 때 혈관화 골이식이 비혈관화 골이식보다 높은 유합률을 보였다.49) 이처럼 최근까지도 근위극 불유합의 치료에 대한 논쟁은 이어지고 있으며 정교하게 설계된 무작위 대조군 연구를 통해서만 이 논쟁이 해소될 것으로 보인다.
Notes
Financial support:None.
Conflict of interests:None.
감사의 글
수술 사진(Fig. 3)을 제공해 주신 제주권역재활병원 이광현 병원장님께 깊은 감사의 말씀을 드립니다.
References
-
Hove LM. Epidemiology of scaphoid fractures in Bergen, Norway. Scand J Plast Reconstr Surg Hand Surg 1999;33:423–426.
-
-
Gelberman RH, Menon J. The vascularity of the scaphoid bone. J Hand Surg Am 1980;5:508–513.
-
-
Berger RA. The anatomy of the scaphoid. Hand Clin 2001;17:525–532.
-
-
Xiao Z, Xiong G, Zhang W. New findings about the intrascaphoid arterial system. J Hand Surg Eur Vol 2018;43:1059–1065.
-
-
Jerome JTJ. Revisiting the natural history of chronic scaphoid nonunions: a retrospective study of 20 cases. J Wrist Surg 2021;10:368–376.
-
-
Steinmann SP, Adams JE. Scaphoid fractures and nonunions: diagnosis and treatment. J Orthop Sci 2006;11:424–431.
-
-
Mack GR, Bosse MJ, Gelberman RH, Yu E. The natural history of scaphoid non-union. J Bone Joint Surg Am 1984;66:504–509.
-
-
Büchler U, Nagy L. The issue of vascularity in fractures and non-union of the scaphoid. J Hand Surg Br 1995;20:726–735.
-
-
Green DP. The effect of avascular necrosis on Russe bone grafting for scaphoid nonunion. J Hand Surg Am 1985;10:597–605.
-
-
Trumble TE. Avascular necrosis after scaphoid fracture: a correlation of magnetic resonance imaging and histology. J Hand Surg Am 1990;15:557–564.
-
-
Rancy SK, Swanstrom MM, DiCarlo EF, Sneag DB, Lee SK, Wolfe SW. Success of scaphoid nonunion surgery is independent of proximal pole vascularity. J Hand Surg Eur Vol 2018;43:32–40.
-
-
Lluch AL, Garcia-Elias M, Lluch AB. Arthroplasty of the scaphoid-trapezium-trapezoid and carpometacarpal joints. Hand Clin 2013;29:57–68.
-
-
Kim JH, Lee KH, Lee BG, Lee CH, Kim SJ, Choi WS. Dorsal intercalated segmental instability associated with malunion of a reconstructed scaphoid. J Hand Surg Eur Vol 2017;42:240–245.
-
-
Watanabe K. Analysis of carpal malalignment caused by scaphoid nonunion and evaluation of corrective bone graft on carpal alignment. J Hand Surg Am 2011;36:10–16.
-
-
Russe O. Fracture of the carpal navicular. Diagnosis, non-operative treatment, and operative treatment. J Bone Joint Surg 1960;42:759–768.
-
-
Herbert TJ, Fisher WE. Management of the fractured scaphoid using a new bone screw. J Bone Joint Surg Br 1984;66:114–123.
-
-
Grover R. Clinical assessment of scaphoid injuries and the detection of fractures. J Hand Surg Br 1996;21:341–343.
-
-
Parvizi J, Wayman J, Kelly P, Moran CG. Combining the clinical signs improves diagnosis of scaphoid fractures. A prospective study with follow-up. J Hand Surg Br 1998;23:324–327.
-
-
Jenkins PJ, Slade K, Huntley JS, Robinson CM. A comparative analysis of the accuracy, diagnostic uncertainty and cost of imaging modalities in suspected scaphoid fractures. Injury 2008;39:768–774.
-
-
Brismar J. Skeletal scintigraphy of the wrist in suggested scaphoid fracture. Acta Radiol 1988;29:101–107.
-
-
Jain R, Jain N, Sheikh T, Yadav C. Early scaphoid fractures are better diagnosed with ultrasonography than X-rays: a prospective study over 114 patients. Chin J Traumatol 2018;21:206–210.
-
-
Langhoff O, Andersen JL. Consequences of late immobilization of scaphoid fractures. J Hand Surg Br 1988;13:77–79.
-
-
Tada K, Ikeda K, Okamoto S, Hachinota A, Yamamoto D, Tsuchiya H. Scaphoid fracture--overview and conservative treatment. Hand Surg 2015;20:204–209.
-
-
Cooney WP, Dobyns JH, Linscheid RL. Fractures of the scaphoid: a rational approach to management. Clin Orthop Relat Res 1980;(149):90–97.
-
-
Doornberg JN, Buijze GA, Ham SJ, Ring D, Bhandari M, Poolman RW. Nonoperative treatment for acute scaphoid fractures: a systematic review and meta-analysis of randomized controlled trials. J Trauma 2011;71:1073–1081.
-
-
Buijze GA, Goslings JC, Rhemrev SJ, et al. Cast immobilization with and without immobilization of the thumb for nondisplaced and minimally displaced scaphoid waist fractures: a multicenter, randomized, controlled trial. J Hand Surg Am 2014;39:621–627.
-
-
Al-Ajmi TA, Al-Faryan KH, Al-Kanaan NF, et al. A systematic review and meta-analysis of randomized controlled trials comparing surgical versus conservative treatments for acute undisplaced or minimally-displaced scaphoid fractures. Clin Orthop Surg 2018;10:64–73.
-
-
Haddad FS, Goddard NJ. Acute percutaneous scaphoid fixation. A pilot study. J Bone Joint Surg Br 1998;80:95–99.
-
-
Slade JF 3rd, Jaskwhich D. Percutaneous fixation of scaphoid fractures. Hand Clin 2001;17:553–574.
-
-
Morsy M, Sabbagh MD, van Alphen NA, Laungani AT, Kadar A, Moran SL. The vascular anatomy of the scaphoid: new discoveries using micro-computed tomography imaging. J Hand Surg Am 2019;44:928–938.
-
-
Adkison JW, Chapman MW. Treatment of acute lunate and perilunate dislocations. Clin Orthop Relat Res 1982;(164):199–207.
-
-
Apergis E, Maris J, Theodoratos G, Pavlakis D, Antoniou N. Perilunate dislocations and fracture-dislocations. Closed and early open reduction compared in 28 cases. Acta Orthop Scand Suppl 1997;275:55–59.
-
-
Herzberg G, Comtet JJ, Linscheid RL, Amadio PC, Cooney WP, Stalder J. Perilunate dislocations and fracture-dislocations: a multicenter study. J Hand Surg Am 1993;18:768–779.
-
-
Slutsky DJ, Trevare J. Use of arthroscopy for the treatment of scaphoid fractures. Hand Clin 2014;30:91–103.
-
-
Geissler WB, Hammit MD. Arthroscopic aided fixation of scaphoid fractures. Hand Clin 2001;17(viii):575–588.
-
-
Fernandez DL. A technique for anterior wedge-shaped grafts for scaphoid nonunions with carpal instability. J Hand Surg Am 1984;9:733–737.
-
-
Merrell GA, Wolfe SW, Slade JF 3rd. Treatment of scaphoid nonunions: quantitative meta-analysis of the literature. J Hand Surg Am 2002;27:685–691.
-
-
Zaidemberg C, Siebert JW, Angrigiani C. A new vascularized bone graft for scaphoid nonunion. J Hand Surg Am 1991;16:474–478.
-
-
Doi K, Oda T, Soo-Heong T, Nanda V. Free vascularized bone graft for nonunion of the scaphoid. J Hand Surg Am 2000;25:507–519.
-
-
Steinmann SP, Bishop AT, Berger RA. Use of the 1,2 intercompartmental supraretinacular artery as a vascularized pedicle bone graft for difficult scaphoid nonunion. J Hand Surg Am 2002;27:391–401.
-
-
Jones DB Jr, Bürger H, Bishop AT, Shin AY. Treatment of scaphoid waist nonunions with an avascular proximal pole and carpal collapse. Surgical technique. J Bone Joint Surg Am 2009;91 Suppl 2:169–183.
-
-
Megerle K, Keutgen X, Müller M, Germann G, Sauerbier M. Treatment of scaphoid non-unions of the proximal third with conventional bone grafting and mini-Herbert screws: an analysis of clinical and radiological results. J Hand Surg Eur Vol 2008;33:179–185.
-
-
Derby BM, Murray PM, Shin AY, et al. Vascularized bone grafts for the treatment of carpal bone pathology. Hand (N Y) 2013;8:27–40.
-
-
Jones DB Jr, Rhee PC, Shin AY. Vascularized bone grafts for scaphoid nonunions. J Hand Surg Am 2012;37:1090–1094.
-
-
Rancy SK, Schmidle G, Wolfe SW. Does anyone need a vascularized graft? Hand Clin 2019;35:323–344.
-
-
Matsuki H, Ishikawa J, Iwasaki N, Uchiyama S, Minami A, Kato H. Non-vascularized bone graft with Herbert-type screw fixation for proximal pole scaphoid nonunion. J Orthop Sci 2011;16:749–755.
-
-
Putnam JG, DiGiovanni RM, Mitchell SM, Castañeda P, Edwards SG. Plate fixation with cancellous graft for scaphoid nonunion with avascular necrosis. J Hand Surg Am 2019;44:339.e1–339.e7.
-
-
Luchetti TJ, Rao AJ, Fernandez JJ, Cohen MS, Wysocki RW. Fixation of proximal pole scaphoid nonunion with non-vascularized cancellous autograft. J Hand Surg Eur Vol 2018;43:66–72.
-
-
Aibinder WR, Wagner ER, Bishop AT, Shin AY. Bone grafting for scaphoid nonunions: is free vascularized bone grafting superior for scaphoid nonunion? Hand (N Y) 2019;14:217–222.
-
 Cite
Cite
