 E-submission
E-submission TOTA
TOTA TOTS
TOTS
Articles
- Page Path
- HOME > J Musculoskelet Trauma > Volume 24(2); 2011 > Article
-
Original Article
- Autogenous Iliac Bone Grafting for the Treatment of Nonunion in the Hand Fracture
- Joo-Yong Kim, M.D., Young-Keun Lee, M.D., Ph.D., Ki-Chan An, M.D., Tae-Woo Sung, M.D.
-
Journal of the Korean Fracture Society 2011;24(2):163-168.
DOI: https://doi.org/10.12671/jkfs.2011.24.2.163
Published online: April 13, 2011
Department of Orthopedic Surgery, Pusan Paik Hospital, College of Medicine, Inje University, Busan, Korea.
*Department of Orthopedic Surgery, Dason Orthopaedic Clinic, Jeonju, Korea.
- Address reprint requests to: Young-Keun Lee, M.D. Department of Orthopedic Surgery, Dason Orthopaedic Clinic, 1572-8, Inju-dong, Deokjin-gu, Jeonju 561-232, Korea. Tel: 82-63-249-8300, Fax: 82-63-246-6900, trueyklee@yahoo.co.kr
• Received: August 22, 2010 • Revised: December 15, 2010 • Accepted: February 16, 2011
Copyright © 2011 The Korean Fracture Society
- 1,183 Views
- 8 Download
- 1 Crossref
Abstract
-
Purpose
- To evaluate autogenous iliac bone graft for nonunion after hand fracture.
-
Materials and Methods
- From October 2006 through September 2008, we analyzed 35 patients, 37 cases of autogenous iliac bone graft for nonunion after hand fracture that have followed up for more than 12 months. We analyzed about etiology, fracture site, initial treatment, time to bone graft, grafted bone size, grafted bone fixation method, radiologic time of bony healing and bone union rate retrospectively. Also we evaluated VAS and range of motion of each joints (MCP, PIP, DIP) at final follow-up assessment.
-
Results
- Etiology was open fracture 23 cases (62.2%), crushing injury 12 cases (32.4%), direct trauma 2 cases (5.4%). Fracture site was metacarpal bone 7 cases, proximal phalanx 17 cases, middle phalanx 8 cases, distal phalanx 5 cases. Time to bone graft was average 20.7 weeks. Grafted bone fixation method was fixation with K-wire 27 cases (73.0%), fixation with only plate 6 cases (16.2%), fixation with K-wire plus plate 2 cases (5.4%), fixation with K-wire plus cerclage wiring 2 cases (5.4%). Grafted bone size was average 0.93 cm3 and bony union time was average 11.1 weeks and we had bone union in all cases.
-
Conclusion
- Autogenous iliac bone graft is the useful method in the reconstruction of non-union as complication after hand fracture.
- 1. Barton NJ. Fractures of the shafts of the phalanges of the hand. Hand, 1979;11:119-133.ArticlePDF
- 2. Duncan RW, Freeland AE, Jabaley ME, Meydrech EF. Open hand fractures: an analysis of the recovery of active motion and of complications. J Hand Surg Am, 1993;18:387-394.Article
- 3. Freeland AE, Rehm JP. Autogenous bone grafting for fractures of the hand. Tech Hand Up Extrem Surg, 2004;8:78-86.Article
- 4. Gonzalez MH, McKay W, Hall RF Jr. Low-velocity gunshot wounds of the metacarpal: treatment by early stable fixation and bone grafting. J Hand Surg Am, 1993;18:267-270.Article
- 5. Gross TP, Cox QG, Jinnah RH. History and current application of bone transplantation. Orthopedics, 1993;16:895-900.ArticlePubMed
- 6. Jupiter JB, Koniuch MP, Smith RJ. The management of delayed union and nonunion of the metacarpals and phalanges. J Hand Surg Am, 1985;10:457-466.Article
- 7. Rinaldi E. Autografts in the treatment of osseous defects in the forearm and hand. J Hand Surg Am, 1987;12:282-286.Article
- 8. Saint-Cyr M, Gupta A. Primary internal fixation and bone grafting for open fractures of the hand. Hand Clin, 2006;22:317-327.Article
- 9. Saint-Cyr M, Miranda D, Gonzalez R, Gupta A. Immediate corticocancellous bone autografting in segmental bone defects of the hand. J Hand Surg Br, 2006;31:168-177.ArticlePDF
- 10. Smith FL, Rider DL. A study of the healing of one hundred consecutive phalangeal fracture. J Bone Joint Surg Am, 1935;17:91-109.
- 11. Stahl S, Lerner A, Kaufman T. Immediate autografting of bone in open fractures with bone loss of the hand: a preliminary report. Case reports. Scand J Plast Reconstr Surg Hand Surg, 1999;33:117-122.
- 12. Sundine M, Scheker LR. A comparison of immediate and staged reconstruction of the dorsum of the hand. J Hand Surg Br, 1996;21:216-221.ArticlePDF
REFERENCES
Fig. 1
A 28-year-old man sustained middle phalanx fracture of right index finger by belt injury.
(A) The anteroposterior view of the preoperative X-ray shows bony gap of the fracture site at 3 months after initial operation.
(B) Immediate postoperative X-ray shows autogenous iliac bone graft and K-wire fixation.
(C) At eight weeks after autogenous iliac bone graft, the X-ray shows the medullary bridge of the fracture site.
(D) The anteroposterior view of the X-ray after K-wire removal shows the filling of the bony gap.
(E) Finger extension and (F) Flexion at final evaluation. He ultimately recovered 70% of his finger motion, had no pain, and used his finger in pinching and griping activities.
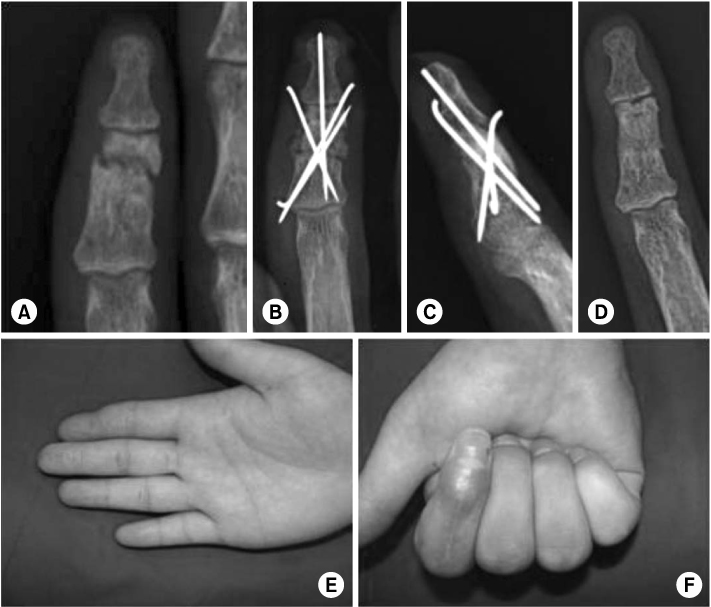
Fig. 2
A 22-year-old man sustained distal phalanx open fracture of left index finger. The osteomyelitis was developed after K-wires fixation at local clinic.
(A) The anteroposterior view of the preoperative X-ray shows osteolytic lesion of distal phalanx.
(B) Antibiotics mixed cement was inserted after debridement and curettage.
(C) At four weeks after antibiotics mixed cement insertion, autogenous iliac bone graft and K-wire fixation was done.
(D) The X-ray after K-wire removal shows the bony union.
(E) Finger extension and (F) Flexion at final evaluation. He ultimately recovered nearly complete of his finger function.

Fig. 3
A 52-year-old woman sustained middle phalanx open fracture of left index finger.
(A) The anteroposterior view of the X-ray shows after initial opertaion.
(B) Preoperative X-ray shows bony gap of the fracture site at 3 months after initial operation.
(C) Immediate postoperative X-ray shows autogenous iliac bone graft and K-wire fixation.
(D) The X-ray after K-wire removal shows the bony union.
(E) Finger extension, 0° and (F) Flexion, 70° at final evaluation.
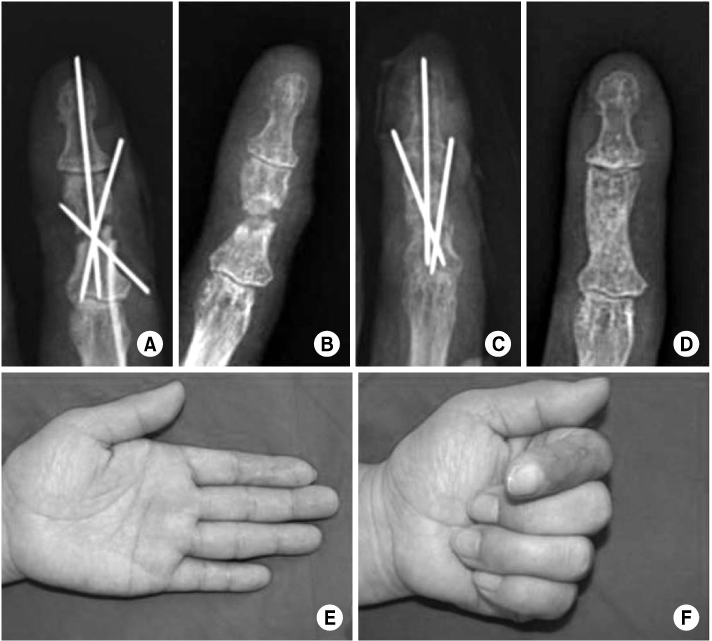
Fig. 4
A 39-year-old woman sustained multiple open fracture and dislocation of left hand by machine injury. Multiple fractures were fixed mulitple K-wires at the time of injury.
(A) Preoperative view shows non-union of 5th metacarpla fracture site at 3 months after initial operation.
(B) Immediate postoperative X-ray shows autogenous iliac bone graft and miniplate fixation.
(C) At 10 weeks after autogenous iliac bone graft, the anteroposterior view of the X-ray shows cortical continuity of the fracture site.
(D) The anteroposterior view of the X-ray after miniplate removal shows the filling of the bony gap.
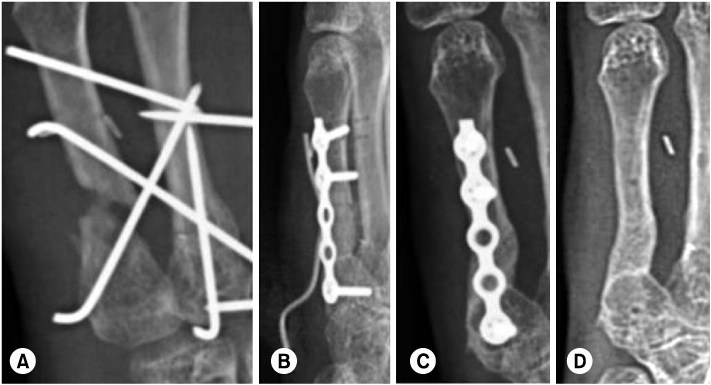
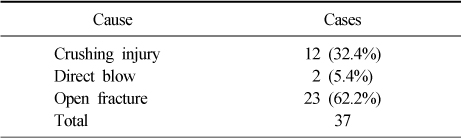
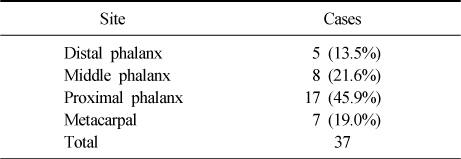

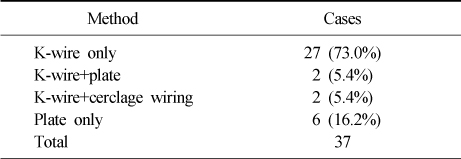
Figure & Data
REFERENCES
Citations
Citations to this article as recorded by 
- Staged treatment with bone cement insertion and autogenous iliac bone grafting for subacute/chronic phalangeal osteomyelitis in the hand
Young-Keun Lee, Ji Woong Ho
Journal of Orthopaedic Surgery.2025;[Epub] CrossRef
 Cite
CiteAutogenous Iliac Bone Grafting for the Treatment of Nonunion in the Hand Fracture


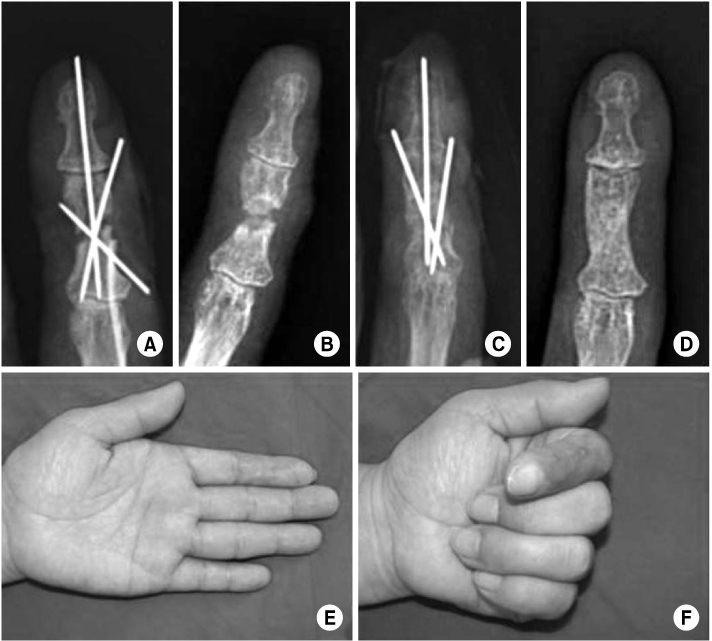
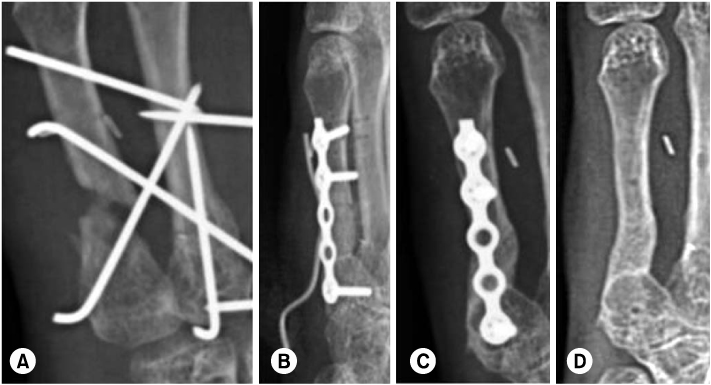
Fig. 1
A 28-year-old man sustained middle phalanx fracture of right index finger by belt injury.
(A) The anteroposterior view of the preoperative X-ray shows bony gap of the fracture site at 3 months after initial operation.
(B) Immediate postoperative X-ray shows autogenous iliac bone graft and K-wire fixation.
(C) At eight weeks after autogenous iliac bone graft, the X-ray shows the medullary bridge of the fracture site.
(D) The anteroposterior view of the X-ray after K-wire removal shows the filling of the bony gap.
(E) Finger extension and (F) Flexion at final evaluation. He ultimately recovered 70% of his finger motion, had no pain, and used his finger in pinching and griping activities.
Fig. 2
A 22-year-old man sustained distal phalanx open fracture of left index finger. The osteomyelitis was developed after K-wires fixation at local clinic.
(A) The anteroposterior view of the preoperative X-ray shows osteolytic lesion of distal phalanx.
(B) Antibiotics mixed cement was inserted after debridement and curettage.
(C) At four weeks after antibiotics mixed cement insertion, autogenous iliac bone graft and K-wire fixation was done.
(D) The X-ray after K-wire removal shows the bony union.
(E) Finger extension and (F) Flexion at final evaluation. He ultimately recovered nearly complete of his finger function.
Fig. 3
A 52-year-old woman sustained middle phalanx open fracture of left index finger.
(A) The anteroposterior view of the X-ray shows after initial opertaion.
(B) Preoperative X-ray shows bony gap of the fracture site at 3 months after initial operation.
(C) Immediate postoperative X-ray shows autogenous iliac bone graft and K-wire fixation.
(D) The X-ray after K-wire removal shows the bony union.
(E) Finger extension, 0° and (F) Flexion, 70° at final evaluation.
Fig. 4
A 39-year-old woman sustained multiple open fracture and dislocation of left hand by machine injury. Multiple fractures were fixed mulitple K-wires at the time of injury.
(A) Preoperative view shows non-union of 5th metacarpla fracture site at 3 months after initial operation.
(B) Immediate postoperative X-ray shows autogenous iliac bone graft and miniplate fixation.
(C) At 10 weeks after autogenous iliac bone graft, the anteroposterior view of the X-ray shows cortical continuity of the fracture site.
(D) The anteroposterior view of the X-ray after miniplate removal shows the filling of the bony gap.
Fig. 1
Fig. 2
Fig. 3
Fig. 4
Autogenous Iliac Bone Grafting for the Treatment of Nonunion in the Hand Fracture
Cause of injury
Fracture site
Initial treatment
CRIF: Closed reduction and internal fixation, ORIF: Open reduction and internal fixation.
Grafted bone fixation method
Table 1
Cause of injury
Table 2
Fracture site
Table 3
Initial treatment
CRIF: Closed reduction and internal fixation, ORIF: Open reduction and internal fixation.
Table 4
Grafted bone fixation method

