 E-submission
E-submission TOTA
TOTA TOTS
TOTS
Articles
- Page Path
- HOME > J Musculoskelet Trauma > Volume 32(2); 2019 > Article
- Review Article Locked Plating in Elderly Patients with Distal Femur Fracture: How to Avoid Complications?
- Chul Young Jang, Je Hyun Yoo
-
Journal of Musculoskeletal Trauma 2019;32(2):112-119.
DOI: https://doi.org/10.12671/jkfs.2019.32.2.112
Published online: April 30, 2019
Department of Orthropaedic Surgery, Hallym University Sacred Heart Hospital, Anyang, Korea. oships@hallym.ac.kr
- 1,569 Views
- 33 Download
- 0 Crossref
- 0 Scopus
Abstract
Distal femur fractures in elderly patients with osteoporosis are complicated because poor bone quality makes screw purchase and fixation less secure, presenting many clinical challenges to the orthopedic surgeon. Minimally invasive locked plating using an angularly stable locking compression plate has become an integral tool for achieving secure fixation in osteoporotic distal femur fractures with improved biomechanical performance. On the other hand, complications, such as implant failure and periplate fracture, have still occurred. This paper describes the principles of internal fixation in minimally invasive lateral locked plating in elderly patients with osteoporotic distal femur fractures as well as how to avoid complications.
J Korean Fract Soc. 2019 Apr;32(2):112-119. Korean.
Published online Apr 16, 2019.
https://doi.org/10.12671/jkfs.2019.32.2.112
Published online Apr 16, 2019.
https://doi.org/10.12671/jkfs.2019.32.2.112
Copyright © 2019 The Korean Fracture Society. All rights reserved.
Review
Locked Plating in Elderly Patients with Distal Femur Fracture: How to Avoid Complications?
Chul-Young Jang , M.D.
and Je-Hyun Yoo, M.D., Ph.D.
, M.D.
and Je-Hyun Yoo, M.D., Ph.D.
, M.D.
and Je-Hyun Yoo, M.D., Ph.D.
Abstract
Distal femur fractures in elderly patients with osteoporosis are complicated because poor bone quality makes screw purchase and fixation less secure, presenting many clinical challenges to the orthopedic surgeon. Minimally invasive locked plating using an angularly stable locking compression plate has become an integral tool for achieving secure fixation in osteoporotic distal femur fractures with improved biomechanical performance. On the other hand, complications, such as implant failure and periplate fracture, have still occurred. This paper describes the principles of internal fixation in minimally invasive lateral locked plating in elderly patients with osteoporotic distal femur fractures as well as how to avoid complications.
Keywords
Distal femur, Osteoporotic fracture, Lateral locked plating, Complications
Figures

Fig. 1
Indirect reduction in the sagittal plane in a distal femur fracture. (A) Posterior angulation by deforming forces of the surrounding muscles. Reduction methods using a bump beneath the distal thigh (B) or a Schanz screw (C).
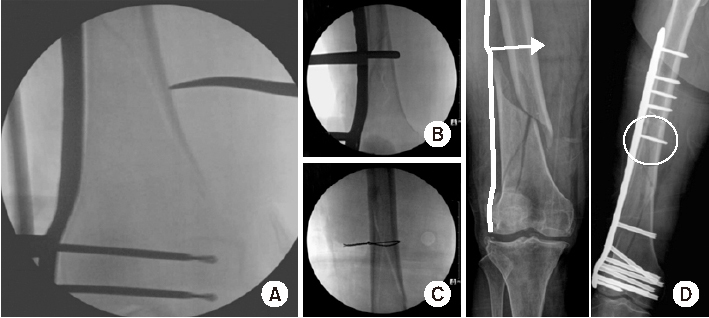
Fig. 2
Direct reduction methods in the coronal plane in distal femur fractures using a long hemostatic tonsil (A), Collinear reduction clamp (B), percutaneous wiring (C), or conventional cortical screw (D).
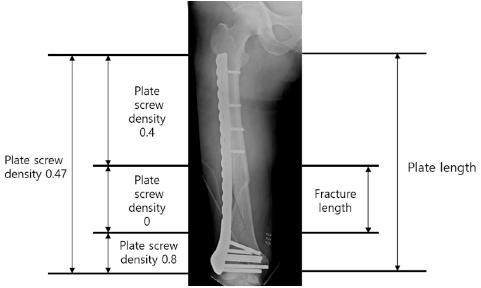
Fig. 3
Appropriate plate length and plate-screw density after minimally invasive plate osteosynthesis using a locking plate in osteoporotic distal femur fractures.
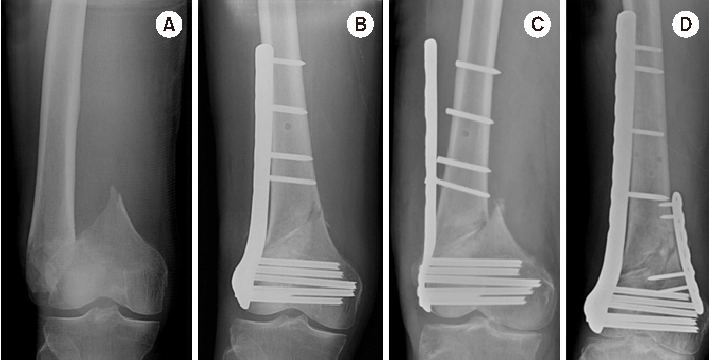
Fig. 4
(A) Distal femur fracture in a 70-year-old male. (B) Postoperative anteroposterior radiograph after minimally invasive locked plating. (C) Fixation failure along with broken locking screws two months after surgery. (D) Anteroposterior radiograph seven months after double plating showing bony union.
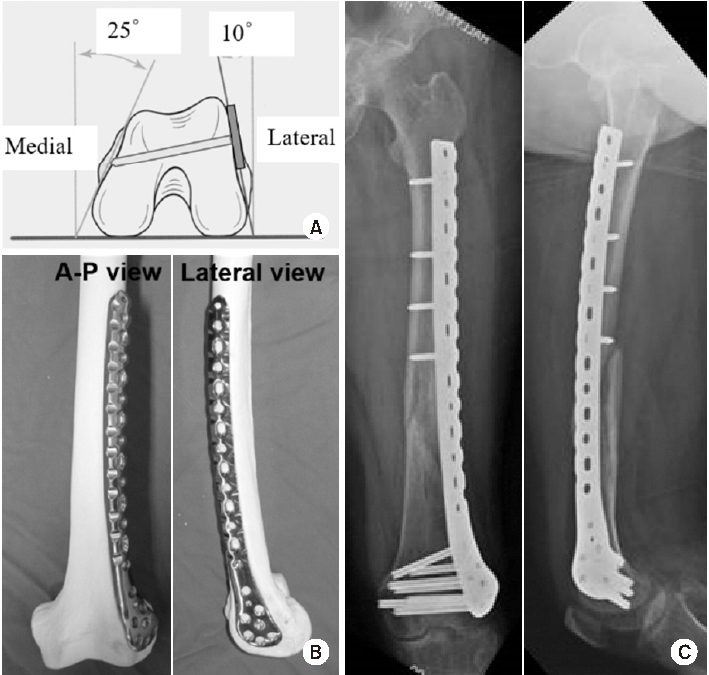
Fig. 5
(A) Schematic diagram showing the axial shape of the distal femur and the appropriate length of distal locking screw. (B) Anteroposterior (A–P) and lateral photos showing the appropriate position of the lateral anatomical locking plate in the distal femur model. (C) A–P and lateral radiographs showing the appropriate position of the locking plate fixed in a distal femur fracture of a 72-year-old female patient.
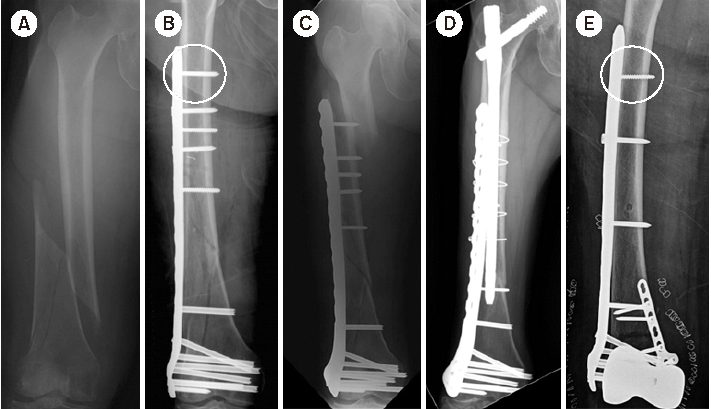
Fig. 6
(A) Radiograph of a distal femur fracture of a 74-year-old female after a ground-level fall. (B) Postoperative radiograph after a closed reduction and minimally invasive locked plating. (C) Six-week postoperative radiograph showing a stress riser fracture around the outermost locking screw after slip-down injury. (D) Radiograph showing bony union two years after overlapping intramedullary nailing. (E) Postoperative radiograph showing locked plating using a conventional cortical screw instead of a locking screw as a proximal outermost screw to minimize the stress riser.
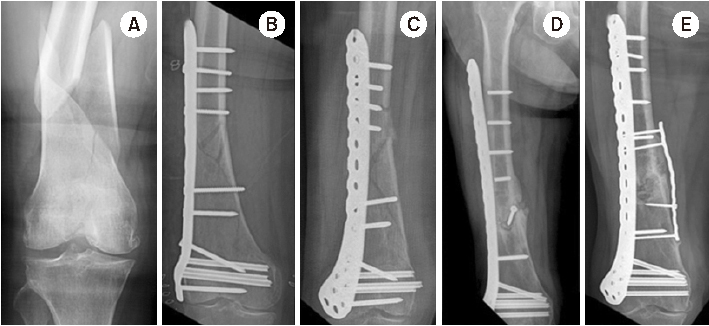
Fig. 7
(A) Radiograph of a distal femur fracture of a 74-year-old female after a ground-level fall. (B) Postoperative radiograph after a closed reduction and minimally invasive locked plating. (C) Six-week postoperative radiograph showing a stress riser fracture around the outermost locking screw after slip-down injury. (D) Radiograph showing bony union two years after overlapping intramedullary nailing. (E) Postoperative radiograph showing locked plating using a conventional cortical screw instead of a locking screw as a proximal outermost screw to minimize the stress riser.
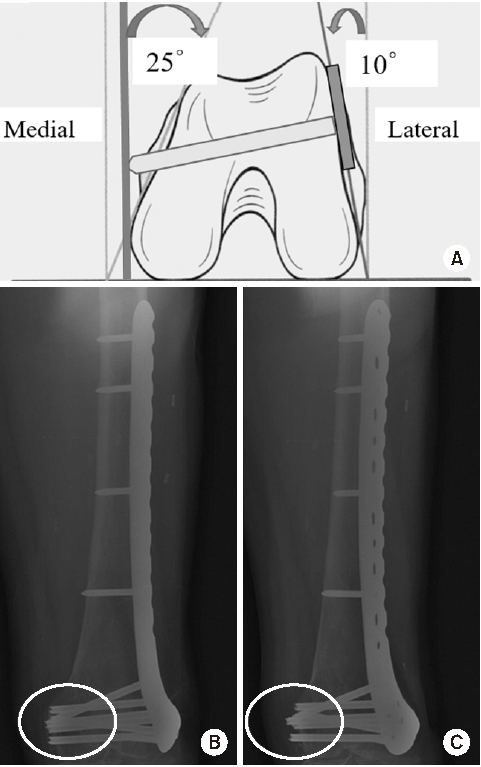
Fig. 8
(A) Schematic diagram showing the axial shape of the distal femur and the protrusion of distal locking screw. (B) True anteroposterior radiograph showing that the lengths of the distal locking screws appear to be appropriate. (C) Radiograph taken after rotating a thigh approximately 25° internally, showing the protrusion of multiple screws across the medial cortex.
Notes
Financial support:None.
Conflict of interests:None.
References
-
Krettek C, Müller M, Miclau T. Evolution of minimally invasive plate osteosynthesis (MIPO) in the femur. Injury 2001;32 Suppl 3:SC14–SC23.
-
-
Stover M. Distal femoral fractures: current treatment, results and problems. Injury 2001;32 Suppl 3:SC3–SC13.
-
-
Wong MK, Leung F, Chow SP. Treatment of distal femoral fractures in the elderly using a less-invasive plating technique. Int Orthop 2005;29:117–120.
-
-
Mast J, Jakob R, Ganz R. In: Planning and reduction technique in fracture surgery. Berlin, New York: Springer-Verlag; 1989.
-
-
Helfet DL, Shonnard PY, Levine D, Borrelli J Jr. Minimally invasive plate osteosynthesis of distal fractures of the tibia. Injury 1997;28 Suppl 1:A42–A47.discussion A47-A48.
-
-
Kinast C, Bolhofner BR, Mast JW, Ganz R. Subtrochanteric fractures of the femur. Results of treatment with the 95 degrees condylar blade-plate. Clin Orthop Relat Res 1989;(238):122–130.
-
-
Krettek C, Schandelmaier P, Miclau T, Tscherne H. Minimally invasive percutaneous plate osteosynthesis (MIPPO) using the DCS in proximal and distal femoral fractures. Injury 1997;28 Suppl 1:A20–A30.
-
-
Wagner M. General principles for the clinical use of the LCP. Injury 2003;34 Suppl 2:B31–B42.
-
-
Goyal T, Nag HL, Tripathy SK. Dynamization of locked plating on distal femur fracture. Arch Orthop Trauma Surg 2011;131:1331–1332.
-
-
Fulkerson E, Egol KA, Kubiak EN, Liporace F, Kummer FJ, Koval KJ. Fixation of diaphyseal fractures with a segmental defect: a biomechanical comparison of locked and conventional plating techniques. J Trauma 2006;60:830–835.
-
-
Gardner MJ, Griffith MH, Demetrakopoulos D, et al. Hybrid locked plating of osteoporotic fractures of the humerus. J Bone Joint Surg Am 2006;88:1962–1967.
-
-
Greiwe RM, Archdeacon MT. Locking plate technology: current concepts. J Knee Surg 2007;20:50–55.
-
-
Lill H, Hepp P, Korner J, et al. Proximal humeral fractures: how stiff should an implant be? A comparative mechanical study with new implants in human specimens. Arch Orthop Trauma Surg 2003;123:74–81.
-
-
Stoffel K, Dieter U, Stachowiak G, Gächter A, Kuster MS. Bio mechanical testing of the LCP: how can stability in locked internal fixators be controlled? Injury 2003;34 Suppl 2:B11–B19.
-
-
Rozbruch SR, Müller U, Gautier E, Ganz R. The evolution of femoral shaft plating technique. Clin Orthop Relat Res 1998;(354):195–208.
-
-
Gautier E, Sommer C. Guidelines for the clinical application of the LCP. Injury 2003;34 Suppl 2:B63–B76.
-
-
Kääb MJ, Frenk A, Schmeling A, Schaser K, Schütz M, Haas NP. Locked internal fixator: sensitivity of screw/plate stability to the correct insertion angle of the screw. J Orthop Trauma 2004;18:483–487.
-
-
Stoffel K, Klaue K, Perren SM. Functional load of plates in fracture fixation in vivo and its correlate in bone healing. Injury 2000;31 Suppl 2:S-B37–S-B50.
-
-
Ahmad M, Nanda R, Bajwa AS, Candal-Couto J, Green S, Hui AC. Biomechanical testing of the locking compression plate: when does the distance between bone and implant significantly reduce construct stability? Injury 2007;38:358–364.
-
-
Henderson CE, Kuhl LL, Fitzpatrick DC, Marsh JL. Locking plates for distal femur fractures: is there a problem with fracture healing? J Orthop Trauma 2011;25 Suppl 1:S8–S14.
-
-
Bottlang M, Doornink J, Byrd GD, Fitzpatrick DC, Madey SM. A nonlocking end screw can decrease fracture risk caused by locked plating in the osteoporotic diaphysis. J Bone Joint Surg Am 2009;91:620–627.
-
-
Yoo JH, Kim SW, Kwak YH, Kim HJ. Overlapping intramedullary nailing after failed minimally invasive locked plating for osteoporotic distal femur fractures: report of 2 cases. Injury 2015;46:1174–1177.
-
-
Kim SM, Yeom JW, Song HK, Hwang KT, Hwang JH, Yoo JH. Lateral locked plating for distal femur fractures by low-energy trauma: what makes a difference in healing? Int Orthop 2018;42:2907–2914.
-
-
Park JY, Yoo JH. Selection of plate in internal fixation of fractures; locking plate and compression plate. J Korean Fract Soc 2013;26:92–102.
-
-
Oh JK, Hwang JH, Lee SJ, Kim JI. Dynamization of locked plating on distal femur fracture. Arch Orthop Trauma Surg 2011;131:535–539.
-
-
Doornink J, Fitzpatrick DC, Boldhaus S, Madey SM, Bottlang M. Effects of hybrid plating with locked and nonlocked screws on the strength of locked plating constructs in the osteoporotic diaphysis. J Trauma 2010;69:411–417.
-
 PubReader
PubReader Cite
Cite
