 E-submission
E-submission TOTA
TOTA TOTS
TOTS
Articles
- Page Path
- HOME > > Ahead-of print articles > Article
-
Case report
- Radiocarpal subluxation after volar plating due to an insufficiently supported dorsal key fragment: a case report
-
Yeongyoon Koh1
 , Kanghun Yu2, Jong Woong Park2, In Cheul Choi2
, Kanghun Yu2, Jong Woong Park2, In Cheul Choi2 -
DOI: https://doi.org/10.12671/jmt.2026.00185
Published online: July 3, 2026
1Department of Orthopedic Surgery, Soonchunhyang University Seoul Hospital, Soonchunhyang University College of Medicine, Seoul, Korea
2Department of Orthopedic Surgery, Korea University Anam Hospital, Korea University College of Medicine, Seoul, Korea
- Correspondence to: In Cheul Choi Department of Orthopedic Surgery, Korea University Anam Hospital, 73 Koryeodae-ro, Seongbuk-gu, Seoul 02841, Korea Tel: +82-2-920-5924 Email: indolldr@korea.ac.kr
• Received: April 28, 2026 • Revised: May 13, 2026 • Accepted: May 13, 2026
© 2026 The Korean Orthopaedic Trauma Association
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/4.0/) which permits unrestricted noncommercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
- 66 Views
- 2 Download
Abstract
- Distal radius fractures are commonly managed using volar locking plate fixation, which provides stable fixation in most cases. However, certain fracture patterns involving dorsal key fragments may not be adequately stabilized with a volar approach alone, even when intraoperative reduction appears satisfactory. We report the case of a 58-year-old male patient with a complex intra-articular distal radius fracture involving a dorsoulnar corner (DUC) fragment. Preoperative computed tomography revealed a dorsal fragment associated with subtle dorsal radiocarpal subluxation. Despite this finding, the fragment was considered amenable to fixation through a volar approach because it was relatively large. Although satisfactory reduction was achieved intraoperatively, early postoperative imaging demonstrated progressive dorsal radiocarpal subluxation due to displacement of the DUC fragment, while overall alignment parameters remained preserved. Revision surgery with additional dorsal buttress fixation successfully restored stability. This case highlights the critical importance of recognizing dorsal key fragments and achieving adequate dorsal support during fixation, as failure to provide sufficient support may result in delayed instability despite acceptable initial reduction.
Introduction
Distal radius fractures are among the most common injuries encountered in orthopedic practice [1]. With the advancement of volar locking plate (VLP) systems and fixation techniques, most of these fractures can now be effectively managed through a volar approach alone, providing stable fixation and favorable clinical outcomes [2-4]. However, this technical progress has also introduced a potential pitfall. Even experienced surgeons may underestimate the need for a dorsal approach in certain fracture patterns or may be tempted to rely solely on volar fixation when the fracture appears adequately reducible intraoperatively.
The concept of key fragments, defined as osteoligamentous units that determine fracture stability and carpal alignment, emphasizes the biomechanical importance of specific fracture components [5]. Fractures involving the dorsoulnar corner (DUC) may represent a dorsal key fragment requiring mechanical support rather than simple fixation.
We present a case that highlights this pitfall and emphasizes the importance of recognizing dorsal key fragments in surgical decision-making.
Case presentation
This case report was approved by the Institutional Review Board (IRB) of Korea University Anam Hospital (IRB No. K2025-0977-001). Written informed consent was obtained from the patient for publication of this case report and accompanying images.
A 58-year-old male patient presented with a left wrist injury following a fall from a height of approximately 1.5 m.
Initial physical examination revealed swelling, tenderness, and limited range of motion without gross neurovascular deficit. The patient was right-hand dominant and had a medical history significant only for hypertension. He was independent in activities of daily living prior to the injury.
Preoperative radiographic and computed tomography (CT) evaluation demonstrated a complex intra-articular distal radius fracture classified as AO/OTA type 23-C3. Quantitative parameters measured on initial radiographs were as follows: radial height 12 mm, radial inclination 25°, volar tilt −30° (dorsal tilt), ulnar variance 9 mm, and articular step-off 3 mm (Fig. 1). A DUC fragment associated with subtle dorsal radiocarpal subluxation was identified. Although recognized, the fragment appeared relatively large on plain radiographs; however, CT imaging revealed dorsal cortical comminution. Nonetheless, stable fixation was anticipated using a volar approach based on the overall fragment size.
Open reduction and internal fixation were performed using a VLP (Medartis Aptus Volar Rim Plate, Medartis AG). Intraoperative fluoroscopy demonstrated satisfactory restoration of radial height, inclination, and volar tilt, with acceptable articular congruity. Immediate postoperative radiographs confirmed maintained reduction with no gross malalignment (Fig. 2).
Following surgery, the wrist was immobilized with a short arm splint, and the patient was instructed to avoid active wrist motion and loading. At 1-week follow-up, radiographs demonstrated dorsal radiocarpal subluxation despite this immobilization (Fig. 3). CT imaging confirmed displacement of the DUC fragment and loss of dorsal support, while conventional radiographic alignment parameters — including radial height, radial inclination, and volar tilt — remained within acceptable ranges; however, radiocarpal congruity was progressively compromised, as evidenced by worsening dorsal carpal translation.
Revision surgery was performed via a dorsal approach, and dorsal buttress fixation was applied to stabilize the DUC fragment. Postoperative imaging demonstrated restoration of radiocarpal alignment without residual subluxation (Fig. 4). The patient showed improved pain and functional recovery during follow-up.
At the 14-month postoperative follow-up, the patient had undergone removal of both the volar locking plate and the dorsal buttress plate via their respective approaches. Radiographic evaluation demonstrated complete bony union with maintained radiocarpal alignment. Clinically, the patient reported minimal pain with a visual analog scale score of 1. Grip strength was 65 pounds (29.5 kg) on the operated side compared to 70 pounds (31.8 kg) on the contralateral side. The Patient-Rated Wrist Evaluation score was 8. Wrist range of motion was as follows: flexion 50°, extension 70°, radial deviation 10°, ulnar deviation 30°, pronation 65°, and supination 80° (Fig. 5). The patient expressed a high level of satisfaction with the surgical outcome and was able to return to his pre-injury level of daily activity without significant limitation.
Discussion
This case highlights a key pitfall in distal radius fracture management in the era of VLP fixation. While VLP systems provide reliable fixation in most cases, certain fracture patterns require biomechanical consideration beyond alignment restoration [2-4]. Despite satisfactory intraoperative reduction, this case demonstrated delayed dorsal instability. This suggests that anatomical alignment alone does not ensure mechanical stability.
The DUC fragment represents a key osteoligamentous unit that contributes to radiocarpal stability. Displacement of this fragment may result in instability patterns not controlled by volar fixation alone. Previous studies have suggested that sufficiently large dorsal key fragments may be amenable to indirect reduction and fixation through a volar approach alone [5]. However, in our experience, dorsal key fragments are frequently associated with comminution, which limits the effectiveness of volar fixation. Therefore, even in cases where indirect reduction appears achievable, surgeons should exercise caution when considering volar fixation alone. Fragment-specific fixation principles support addressing such critical fragments directly [6].
A key distinction highlighted in this case is between fragment capture and fragment support. Although the fragment was captured by volar screws—as confirmed on intraoperative fluoroscopic imaging demonstrating screw tips engaging the DUC fragment (Fig. 2)—the absence of dorsal buttress support led to failure under physiological loading conditions [7].
While slight residual deformity may not significantly impact functional outcomes, this concept does not apply to cases involving structural instability [8]. Dorsal fixation using low-profile plates can effectively restore stability while minimizing complications.
The failure of volar fixation in this case should be interpreted in the context of two potentially coexisting mechanisms. First, technical factors related to screw purchase—including screw length and the ability to achieve adequate cortical purchase in a comminuted fragment—may have contributed to construct instability. In cases involving small or comminuted dorsal fragments, achieving reliable screw purchase through a volar approach is inherently challenging, and this limitation should not be overlooked. Second, and arguably more fundamentally, the failure reflects an underlying biomechanical limitation of volar-only fixation in the setting of a DUC fragment associated with carpal subluxation. Even with optimal screw placement, volar screws provide fragment capture rather than true buttress support; without direct dorsal support, the construct remains vulnerable to failure under physiological loading. Therefore, rather than attributing the failure to either technical or biomechanical factors alone, this case underscores the importance of recognizing both dimensions when planning fixation strategy. Stability in such cases is not achieved by screw purchase alone but requires restoring structural support through appropriate dorsal buttressing—particularly when the fragment is comminuted or associated with carpal subluxation.
This case has several limitations. As a single case report, the findings cannot be generalized to all fracture patterns involving dorsal key fragments. The relative contributions of technical and biomechanical factors to the observed failure could not be definitively determined, and the size threshold beyond which dorsal buttress fixation is required remains undefined.
In conclusion, dorsal key fragments must be carefully identified in distal radius fractures. Even when they appear amenable to volar fixation, they may require dorsal buttress support. Fluoroscopy alone cannot assess mechanical stability, and failure to address these fragments may result in delayed instability.
-
Author contributions
Conceptualization: YK, JWP, ICC. Data curation: YK, KY. Formal analysis: JWP. Investigation: YK. Methodology: ICC. Supervision: ICC. Validation: YK, KY. Writing–original draft: YK. Writing–review & editing: KY, JWP, ICC. All authors have read and approved the final manuscript.
-
Conflicts of interest
No potential conflict of interest relevant to this article was reported.
-
Funding
None.
-
Data availability
Not applicable.
-
Acknowledgments
None.
Article Information
Fig. 1.

Preoperative imaging. Preoperative radiographs (A, B) and computed tomography images (C, D) of the left wrist demonstrating a complex intra-articular distal radius fracture. Axial and sagittal computed tomography images revealed a dorsoulnar corner fragment associated with subtle dorsal radiocarpal subluxation. Yellow arrows indicate the dorsoulnar corner fragment.
Fig. 2.
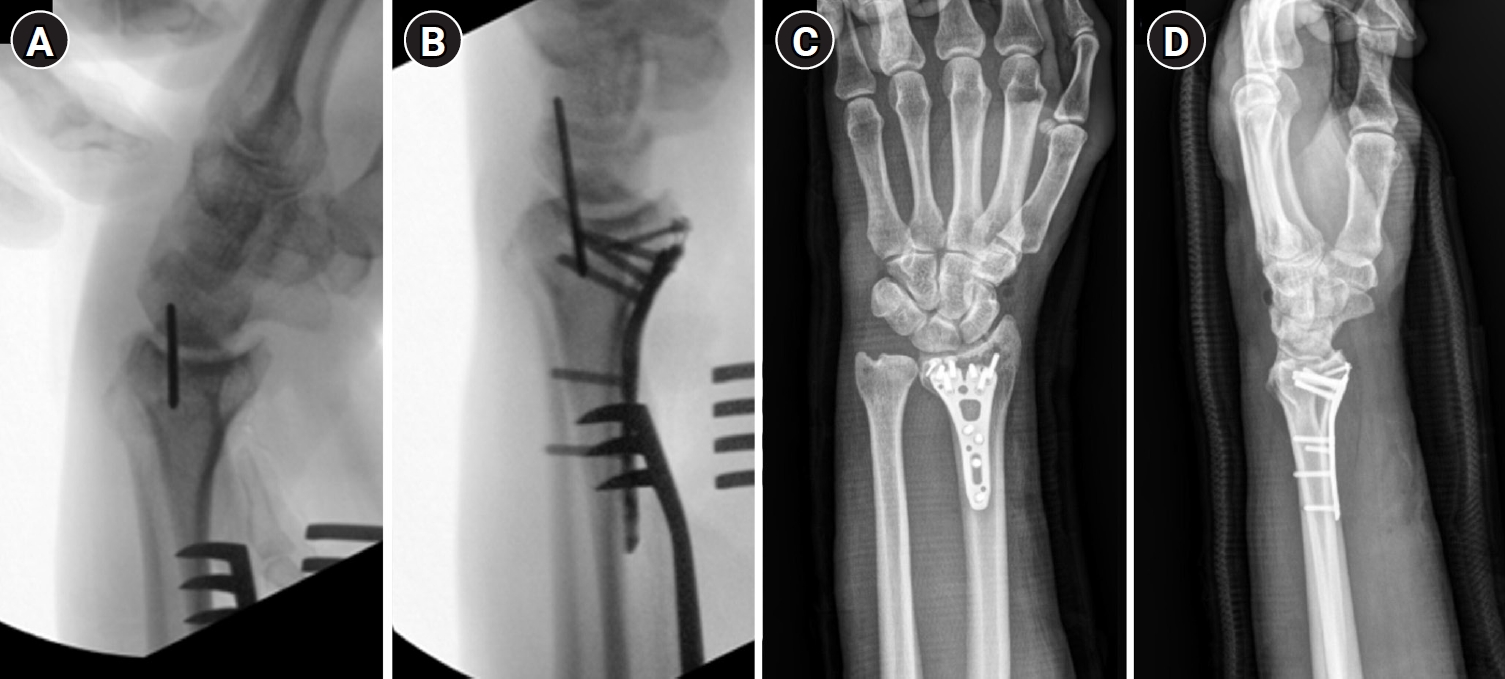
Intraoperative and immediate postoperative imaging. Intraoperative fluoroscopic images (A, B) demonstrated apparent restoration of radial height, inclination, and volar tilt following volar locking plate fixation. Immediate postoperative radiographs (C, D) demonstrated acceptable reduction without obvious dorsal translation or carpal malalignment.
Fig. 3.
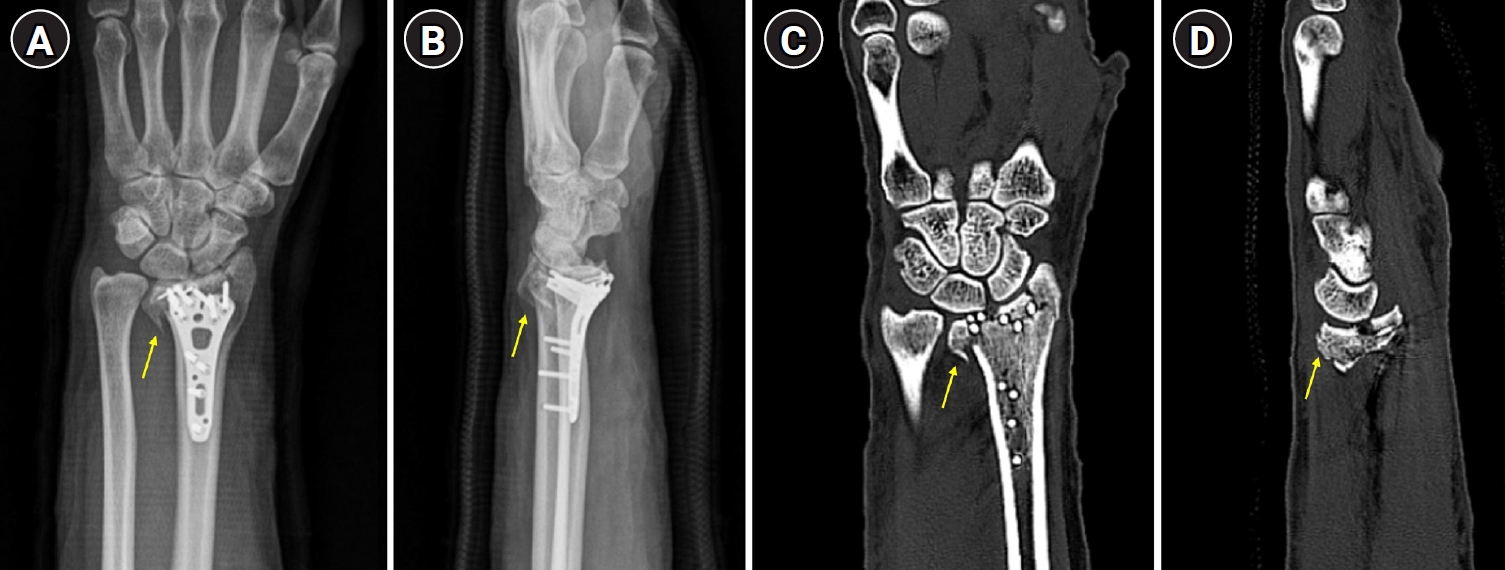
Early postoperative failure. Radiographs (A, B) and computed tomography images (C, D) obtained 1-week postoperatively demonstrated dorsal radiocarpal subluxation. Displacement of the dorsoulnar corner fragment was evident, resulting in loss of dorsal support despite preservation of overall alignment parameters. Yellow arrows indicate the dorsoulnar corner fragment.
Fig. 4.

Revision surgery and outcome. Postoperative radiographs obtained following revision surgery demonstrated restoration of radiocarpal alignment after additional dorsal fixation. (A) Posteroanterior view showing restored radial height and inclination with the dorsal buttress plate in situ. (B) Lateral view confirming restoration of volar tilt and absence of dorsal radiocarpal subluxation. (C) Radial oblique view demonstrating adequate fragment stabilization and articular congruity. (D) Ulnar oblique view confirming restoration of the dorsoulnar corner with no residual subluxation.
Fig. 5.
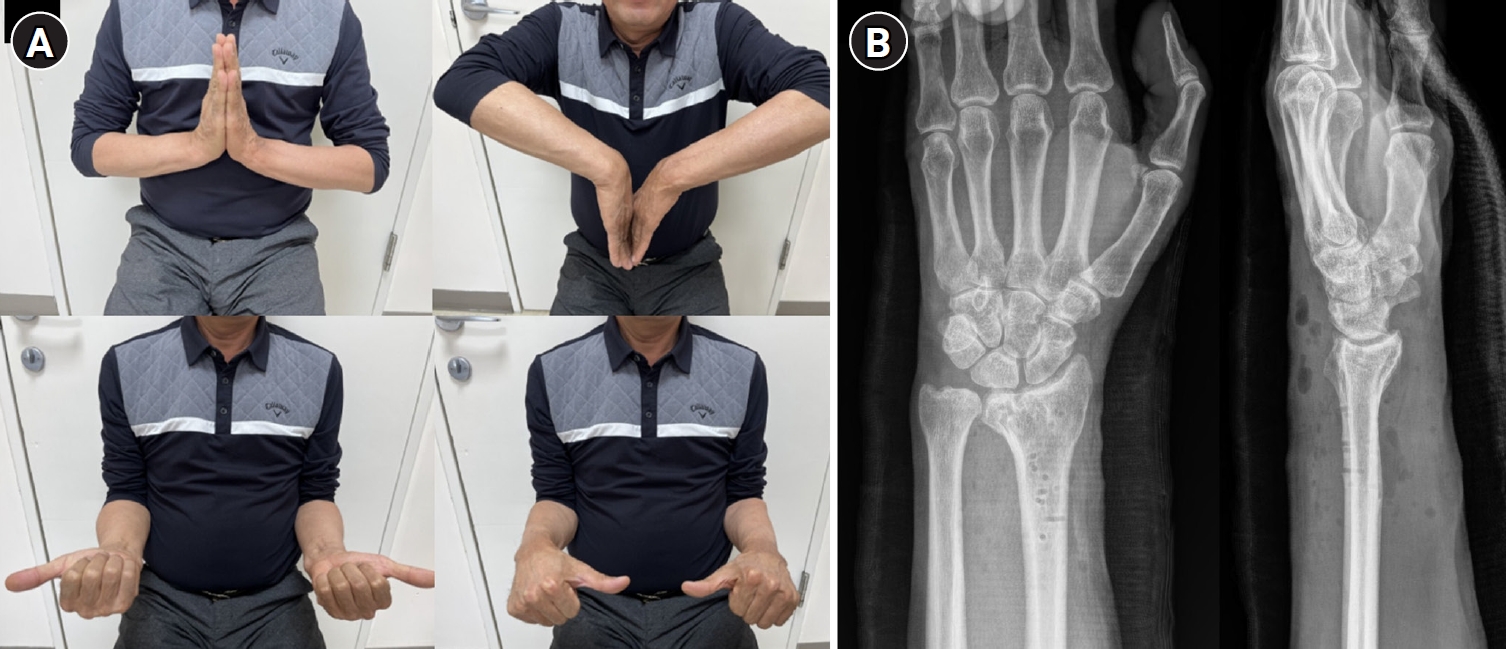
Final follow-up findings. (A) Clinical photographs demonstrating recovery of wrist range of motion, including flexion, extension, pronation, and supination. (B) Radiographs obtained at the final follow-up evaluation, showing complete bony union with maintained joint congruency and satisfactory radiocarpal alignment.
- 1. Chung KC, Spilson SV. The frequency and epidemiology of hand and forearm fractures in the United States. J Hand Surg Am 2001;26:908-15.ArticlePubMed
- 2. Drobetz H, Kutscha-Lissberg E. Osteosynthesis of distal radial fractures with a volar locking screw plate system. Int Orthop 2003;27:1-6.ArticlePubMedPMCPDF
- 3. Orbay JL, Fernandez DL. Volar fixation for dorsally displaced fractures of the distal radius: a preliminary report. J Hand Surg Am 2002;27:205-15.ArticlePubMed
- 4. Simic PM, Robison J, Gardner MJ, Gelberman RH, Weiland AJ, Boyer MI. Treatment of distal radius fractures with a low-profile dorsal plating system: an outcomes assessment. J Hand Surg Am 2006;31:382-6.ArticlePubMed
- 5. Hintringer W, Rosenauer R, Pezzei C, et al. Biomechanical considerations on a CT-based treatment-oriented classification in radius fractures. Arch Orthop Trauma Surg 2020;140:595-609.ArticlePubMedPMCPDF
- 6. Rikli DA, Regazzoni P. Fractures of the distal end of the radius treated by internal fixation and early function: a preliminary report of 20 cases. J Bone Joint Surg Br 1996;78:588-92.ArticlePubMed
- 7. Harness NG, Jupiter JB, Orbay JL, Raskin KB, Fernandez DL. Loss of fixation of the volar lunate facet fragment in fractures of the distal part of the radius. J Bone Joint Surg Am 2004;86:1900-8.ArticlePubMed
- 8. Falk SS, Mittlmeier T, Gradl G. Residual dorsal displacement following surgery in distal radial fractures: a cause for trouble. Eur J Trauma Emerg Surg 2023;49:843-50.ArticlePubMedPMCPDF
References
Figure & Data
REFERENCES
Citations
Citations to this article as recorded by 
 ePub Link
ePub Link Cite
CiteRadiocarpal subluxation after volar plating due to an insufficiently supported dorsal key fragment: a case report

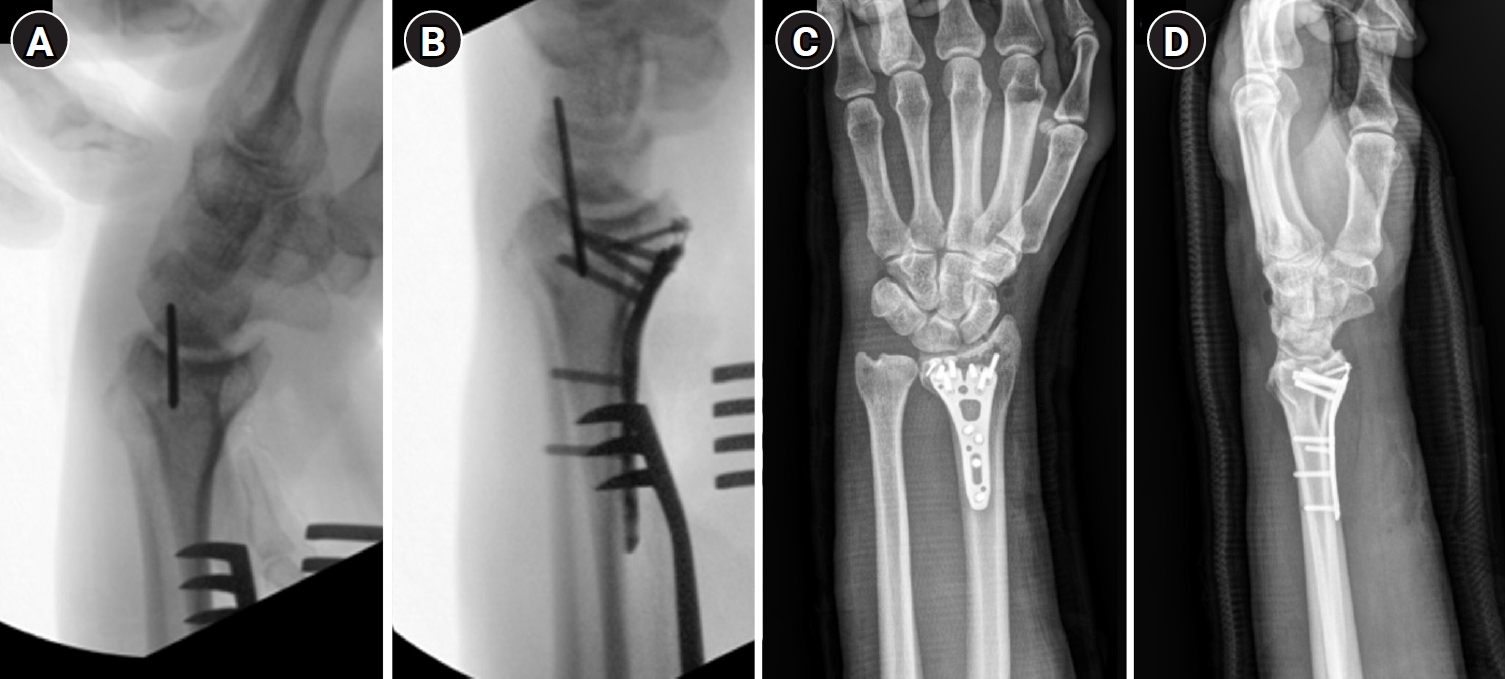
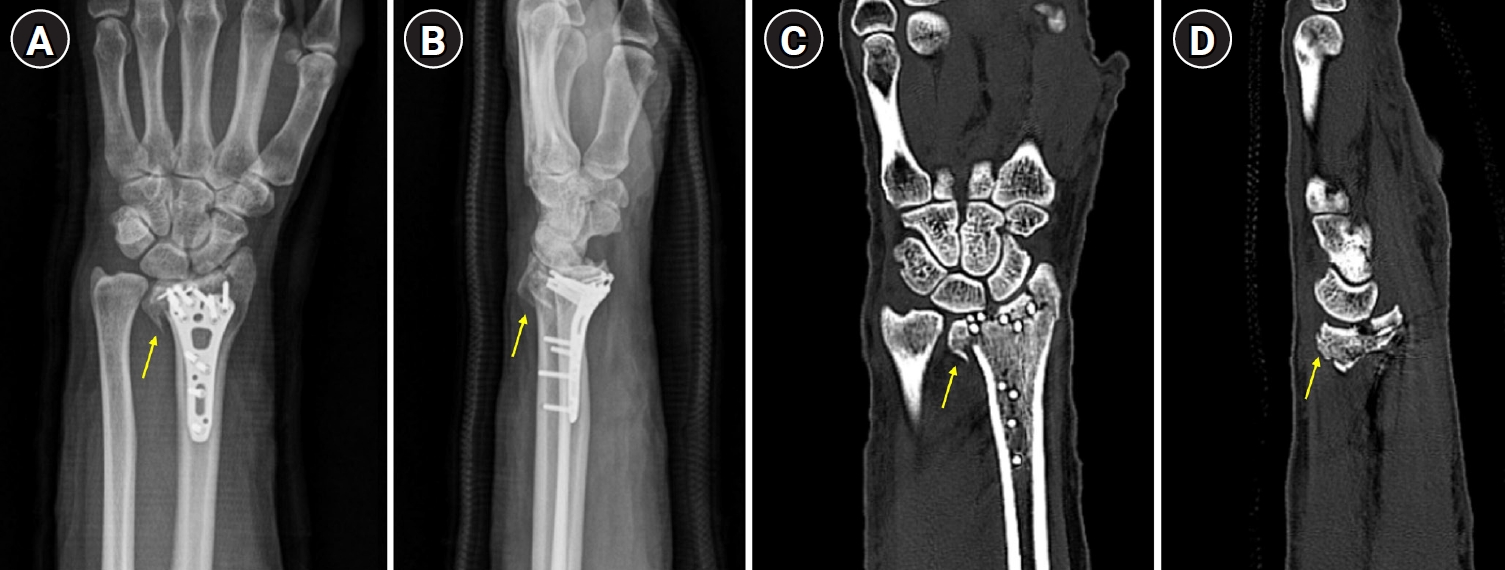

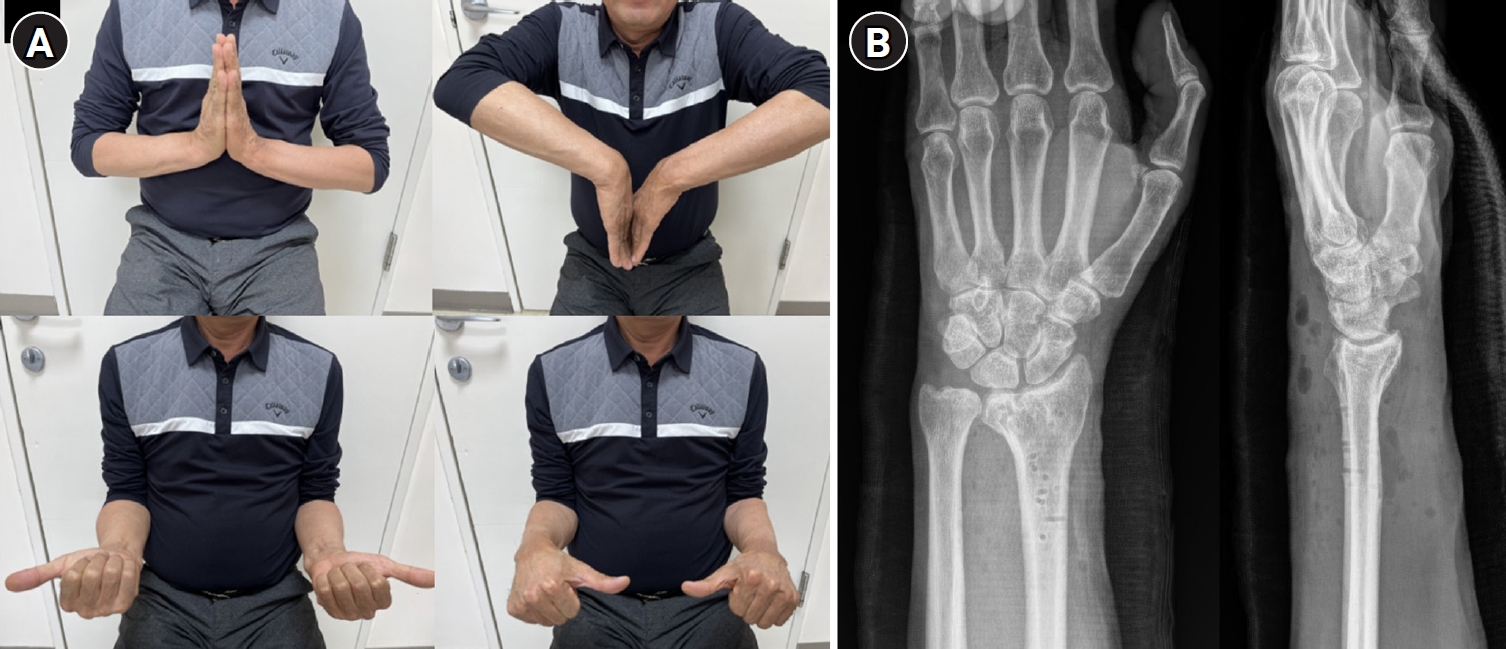
Fig. 1. Preoperative imaging. Preoperative radiographs (A, B) and computed tomography images (C, D) of the left wrist demonstrating a complex intra-articular distal radius fracture. Axial and sagittal computed tomography images revealed a dorsoulnar corner fragment associated with subtle dorsal radiocarpal subluxation. Yellow arrows indicate the dorsoulnar corner fragment.
Fig. 2. Intraoperative and immediate postoperative imaging. Intraoperative fluoroscopic images (A, B) demonstrated apparent restoration of radial height, inclination, and volar tilt following volar locking plate fixation. Immediate postoperative radiographs (C, D) demonstrated acceptable reduction without obvious dorsal translation or carpal malalignment.
Fig. 3. Early postoperative failure. Radiographs (A, B) and computed tomography images (C, D) obtained 1-week postoperatively demonstrated dorsal radiocarpal subluxation. Displacement of the dorsoulnar corner fragment was evident, resulting in loss of dorsal support despite preservation of overall alignment parameters. Yellow arrows indicate the dorsoulnar corner fragment.
Fig. 4. Revision surgery and outcome. Postoperative radiographs obtained following revision surgery demonstrated restoration of radiocarpal alignment after additional dorsal fixation. (A) Posteroanterior view showing restored radial height and inclination with the dorsal buttress plate in situ. (B) Lateral view confirming restoration of volar tilt and absence of dorsal radiocarpal subluxation. (C) Radial oblique view demonstrating adequate fragment stabilization and articular congruity. (D) Ulnar oblique view confirming restoration of the dorsoulnar corner with no residual subluxation.
Fig. 5. Final follow-up findings. (A) Clinical photographs demonstrating recovery of wrist range of motion, including flexion, extension, pronation, and supination. (B) Radiographs obtained at the final follow-up evaluation, showing complete bony union with maintained joint congruency and satisfactory radiocarpal alignment.
Fig. 1.
Fig. 2.
Fig. 3.
Fig. 4.
Fig. 5.
Radiocarpal subluxation after volar plating due to an insufficiently supported dorsal key fragment: a case report

