 E-submission
E-submission TOTA
TOTA TOTS
TOTS
Articles
- Page Path
- HOME > J Musculoskelet Trauma > Volume 39(3); 2026 > Article
-
Case Report
- Successful reconstruction and functional recovery of a pediatric medial malleolus defect in an 8-year-old girl using autologous iliac crest bone grafting in Korea: a case report
- Sung Yoon Jung1, Dong-hee Kim2, Sang Hyun Lee3, Ki-Hun Kim3
-
Journal of Musculoskeletal Trauma 2026;39(3):245-251.
DOI: https://doi.org/10.12671/jmt.2026.00059
Published online: April 8, 2026
1Department of Orthopedic Surgery, Dong-A University Hospital, Dong-A University School of Medicine, Busan, Korea
2Department of Orthopedic Surgery, Samsung Changwon Hospital, Sungkyunkwan University School of Medicine, Changwon, Korea
3Department of Orthopedic Surgery, Pusan National University Hospital, Pusan National University School of Medicine, Busan, Korea
- Correspondence to: Sang Hyun Lee Department of Orthopedic Surgery, Pusan National University Hospital, Pusan National University School of Medicine, 179 Gudeok-ro, Seo-gu, Busan 49241, Korea Tel: +82-51-240-7248 Email: handsurgeon@pusan.ac.kr
• Received: January 15, 2026 • Revised: February 13, 2026 • Accepted: March 4, 2026
© 2026 The Korean Orthopaedic Trauma Association
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/4.0/) which permits unrestricted noncommercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
- 712 Views
- 11 Download
Abstract
-
An 8-year-old girl presented after a traffic accident with a severe crush and degloving injury of the medial right ankle and foot, a distal tibiofibular fracture, and medial midfoot bone defects. After staged irrigation and debridement with temporary external fixation, definitive reconstruction was performed on August 6, 2016. The medial malleolar defect (2.5×2.0 cm) was reconstructed using a contoured autologous iliac crest bone graft secured with internal fixation, and medial stability was augmented using harvested gluteal fascia as a deltoid ligament substitute fixed with suture anchors. A bone-cement spacer was placed adjacent to the injured physis to mitigate physeal bridging, and the extensive soft-tissue defect was covered with a free anterolateral thigh flap and skin graft. During follow-up, progressive varus deformity and contracture were managed with corrective osteotomy and plating, Achilles tendon lengthening, Z-plasty, and Ilizarov fixation. At the final follow-up (March 6, 2025), the limb-length discrepancy was 5 mm, active ankle dorsiflexion was 0° (passive dorsiflexion 5°), and the patient was pain-free with full participation in daily activities, including hiking and dancing. This case emphasizes the value of an integrated staged strategy that combines bony reconstruction, medial stabilization, physeal management, and durable soft-tissue coverage during skeletal growth.
-
Level of evidence V.
Introduction
Salter-Harris type VI physeal injuries represent rare lesions characterized by loss of a portion of the physis and adjacent osteochondral/perichondrial structures, frequently associated with high-energy trauma and extensive soft-tissue injury [1,2]. In the distal tibia, traumatic loss of the medial malleolus is particularly consequential in skeletally immature patients because it simultaneously threatens physeal integrity and ankle stability, including potential growth disturbance from physeal bar formation and medial instability due to deltoid ligament deficiency [1-3]. Management is therefore challenging and must balance limb salvage, infection control, durable soft-tissue coverage, structural reconstruction, and long-term growth-related alignment preservation [3]. We report a pediatric case of traumatic medial malleolar loss managed with staged debridement, autologous iliac crest bone graft reconstruction with medial stabilization, physeal management using a bone-cement spacer, free anterolateral thigh (ALT) flap coverage, and subsequent deformity correction, resulting in long-term functional recovery through growth.
Case report
This study was approved by the Institutional Review Board (IRB) of Pusan National University Hospital (IRB No. 2601-031-159), and written informed consent was obtained from the patient’s legal guardian for publication of this report, including all clinical images.
An 8-year-old girl presented on June 14, 2016 after a traffic accident with a severe crush/degloving injury involving the medial aspect of the right ankle and foot. The family’s main concerns were limb salvage and the risk of growth-related deformity and long-term functional limitation. She had no relevant past medical history.
At presentation, extensive soft-tissue loss of the medial ankle/foot was noted, consistent with a high-energy crush/degloving mechanism (Fig. 1). The wound severity raised concerns for soft-tissue viability, contamination, and subsequent infection risk, and suggested the need for a staged approach with temporary stabilization followed by definitive reconstruction.
Initial plain radiographs demonstrated a distal tibiofibular fracture in a skeletally immature patient, with associated medial-sided midfoot injuries (first metatarsal, medial cuneiform, and medial navicular bone defects) (Fig. 1). During staged management, traumatic loss of the distal tibial medial malleolus was identified, consistent with a Salter-Harris type VI injury pattern and raising concern for physeal bar formation and medial ankle instability due to deltoid ligament deficiency [2,3]. The medial malleolar bony defect was measured intraoperatively as 2.5×2.0 cm to guide graft contouring. Given the severity of the soft-tissue injury, a staged strategy was adopted [1,4].
Stage 1 (damage control; June 14, 2016)
The patient underwent irrigation and debridement with temporary stabilization using an external fixator (Fig. 2). Serial irrigation and debridement procedures (marginal debridement) were performed as needed until the wound condition allowed definitive reconstruction.
Stage 2 (definitive reconstruction; August 6, 2016)
The medial malleolar defect (2.5×2.0 cm) was reconstructed using an autologous iliac crest bone graft harvested and contoured to match the defect (Fig. 3) [4,5]. The graft was secured with internal fixation, and postoperative clinical appearance and radiographs confirmed reconstruction and stabilization (Fig. 4). To restore medial ankle stability, harvested gluteal fascia was used as a deltoid ligament substitute and fixed using suture anchors [1]. To mitigate physeal bridging in the residual void adjacent to the injured physis, a bone-cement spacer was placed [4,5]. The extensive soft-tissue defect was covered using ALT flap and skin graft, achieving stable coverage (Fig. 5) [6,7].
Stage 3 (deformity correction; January 9, 2017)
Progressive varus deformity during follow-up was treated with corrective osteotomy and plate fixation (Fig. 6).
Stage 4 (alignment and contracture management; May 29, 2017)
The patient was observed for more than 6 months after plate fixation, and bone union was achieved for the remaining fracture sites. However, varus deformity gradually occurred (lateral distal tibial angle, 111.5º; tibiotalar tilt, 0.4º). As the patient was relatively young and had substantial remaining growth, early correction was considered advantageous and was therefore performed. Residual deformity tendency and contracture were managed with additional procedures including Achilles tendon lengthening and Z-plasty for tendon/skin contracture release. The bone-cement spacer was removed during this phase. Alignment correction/overcorrection and continued alignment management were supported with an Ilizarov external fixator (Fig. 7). After applying the Ilizarov external fixator for 3 months, radiologic indices were corrected (lateral distal tibial angle, 97.6º; tibiotalar tilt, 0.3º).
At the final follow-up on March 6, 2025, clinical photographs and radiographs demonstrated healed soft tissue, maintained alignment, and functional recovery without recurrent deformity (Fig. 8). Limb-length discrepancy was 5 mm. Active ankle dorsiflexion was 0° with passive dorsiflexion of 5°. The patient reported no pain and returned to unrestricted activities of daily living, including hiking and dancing. Complications during the treatment course were limited to superficial skin/soft-tissue problems, without reported deep infection (Table 1).
Discussion
Salter-Harris type VI physeal injuries are rare and usually occur after high-energy trauma with substantial soft-tissue compromise. In the distal tibia, loss of the medial malleolus is particularly problematic because it combines a risk of physeal bar formation with subsequent angular deformity, limb-length discrepancy and loss of the medial buttress with potential deltoid ligament insufficiency and chronic instability [1-3].
In adults with extensive medial malleolar loss or nonreconstructable tibiotalar articular damage, tibiotalar arthrodesis is often selected as a definitive solution. In children, however, ankle fusion sacrifices a growing joint and may be followed by progressive varus/valgus deformity, limb-length discrepancy, and adjacent-joint overload as growth continues. Therefore, we prioritized a joint-preserving strategy aimed at restoring the medial malleolar buttress and medial stability while actively managing the injured physis [2,3].
A staged pathway (serial debridement and temporary external fixation followed by definitive reconstruction) allowed infection control and optimization of the wound bed before structural reconstruction. After initial temporary fixation with fibular pinning, fibular length was largely maintained. However, by the time of definitive reconstruction, the fibula had begun to unite with surrounding soft-tissue contracture involving the syndesmosis, precluding anatomic reduction to a neutral position. The reconstruction was therefore completed with some residual varus, followed by flap coverage. The medial malleolar defect was reconstructed with a contoured autologous iliac crest graft and rigid fixation, consistent with prior pediatric reports using iliac crest-derived graft to reconstitute the distal medial tibial epiphysis. Medial stability was augmented by reconstructing the deltoid complex using autologous fascia and suture anchors [1,6].
Because type VI injuries involve loss of the perichondral ring and are prone to partial growth arrest, physeal management is a key parallel objective. Interpositional techniques (classically fat interposition after physeal bridge resection or anticipatory procedures) have been advocated to prevent or delay physeal bridging; in the present case, a temporary bone-cement spacer was used as a barrier adjacent to the injured physis during the reconstructive phase and was removed once alignment management was undertaken [1,4,5]. Compared to fat interposition, cement spacers have the advantage of space-occupying properties, allowing them to conform to their original shape during flap wound implantation. They also offer the advantage of weight bearing. In principle, they are not removed unless there are specific concerns. However, in this case, the cement spacer itself could induce soft-tissue tethering during the correction of varus deformity, so it was removed and gradually corrected.
Durable soft-tissue coverage is equally important for limb salvage in these injuries. A free ALT flap provides reliable coverage for pediatric foot and ankle defects and was instrumental in maintaining a stable envelope that permitted subsequent osteotomy and gradual correction during growth [7,8].
This case also highlights the need for prolonged surveillance through skeletal maturity: even after successful initial reconstruction, progressive deformity and contracture can emerge as growth proceeds, requiring timely osteotomy, soft-tissue procedures, and, when necessary, circular external fixation to protect alignment and function [2,3].
Limitations include the inherent constraints of a single case, the lack of standardized patient-reported outcome measures, and the absence of a comparator strategy. In addition, computed tomography was not performed due to concerns regarding radiation exposure, and magnetic resonance imaging was not performed due to artifacts from metallic implants. The authors postulated that differential growth between the flap-covered and native tissues contributed to the observed deformity. Accordingly, early correction was performed to prevent progression of residual deformity. This may be attributed to several factors, including residual varus alignment after plate fixation, incomplete accommodation of longitudinal growth by the flap-covered soft tissue, and persistent soft-tissue tethering, including involvement of the syndesmosis.
Nevertheless, the long-term follow-up to 9 years after injury demonstrates that an integrated, joint-preserving staged strategy can achieve durable function while minimizing growth-related sequelae in pediatric medial malleolar loss.
-
Author contributions
Conceptualization: SYJ, SHL. Methodology: SYJ, DK, KHK. Supervision: SHL. Visualization: KHK, SHL. Writing–original draft: SYJ. Writing–review & editing: SYJ, DK, SHL, KHK. All authors read and approved the final manuscript.
-
Conflicts of interest
No potential conflict of interest relevant to this article was reported.
-
Funding
This work was supported by a clinical research grant from Pusan National University Hospital in 2025.
-
Data availability
Not applicable.
-
Acknowledgments
This case report was presented in the Case Discussion section of the 2026 Annual Congress of the Korean Orthopaedic Trauma Association (KOTA).
-
Supplementary materials
None.
Article Information
Fig. 1.
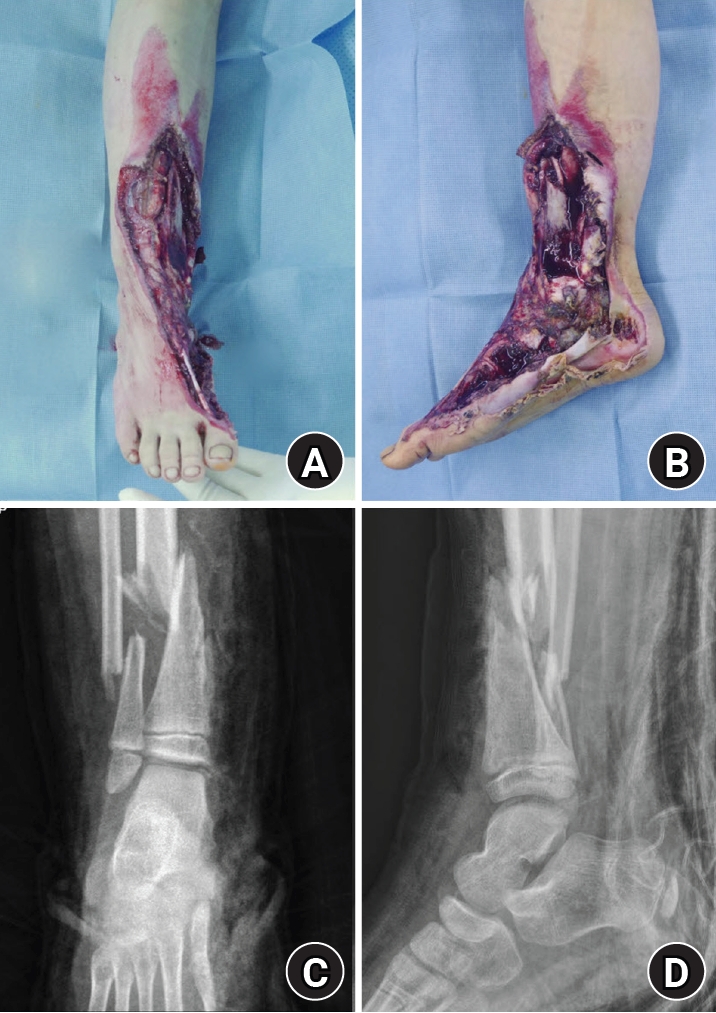
Initial injury on June 14, 2016. (A) Anteroposterior gross photograph obtained at presentation showing a severe crush and degloving injury involving the medial aspect of the right ankle and foot. (B) Lateral gross photograph obtained at presentation demonstrating extensive soft-tissue loss and degloving injury of the medial right ankle and foot. (C) Anteroposterior radiograph obtained at presentation showing an associated distal tibiofibular fracture in a skeletally immature patient. (D) Lateral radiograph obtained at presentation demonstrating the distal tibiofibular fracture.
Fig. 2.
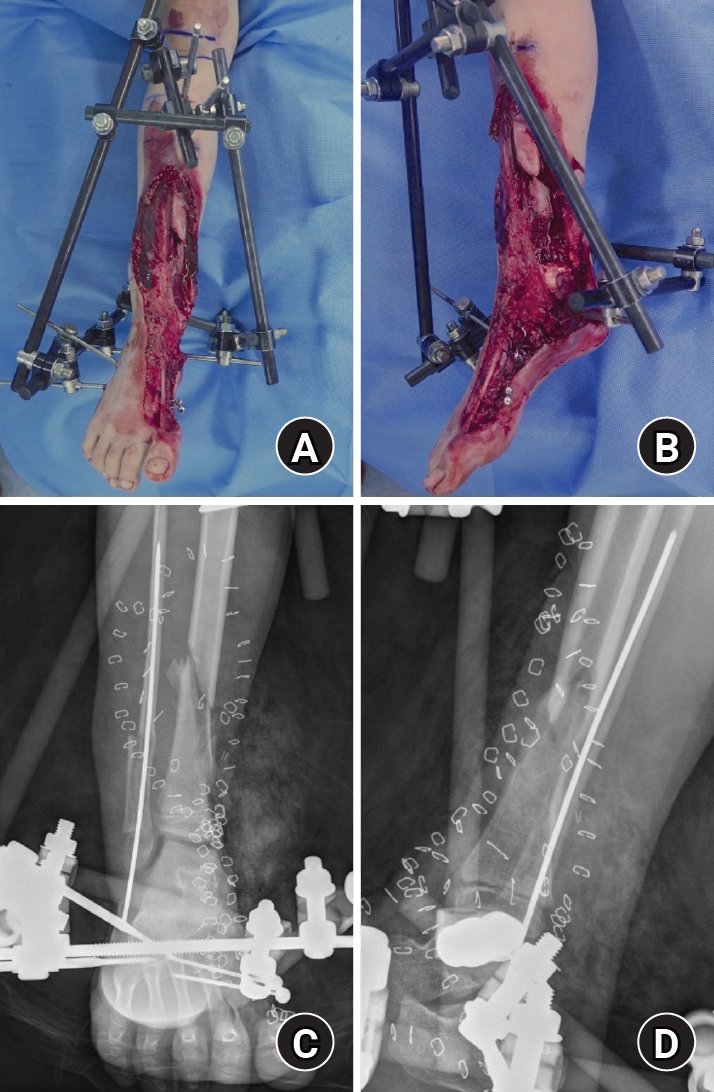
Postdamage control stabilization with external fixation. (A) Anteroposterior gross photograph obtained after initial irrigation and debridement, showing temporary stabilization with an external fixator. (B) Lateral gross photograph obtained after initial irrigation and debridement, demonstrating temporary stabilization with an external fixator. (C) Anteroposterior radiograph obtained after initial irrigation and debridement, showing temporary stabilization with an external fixator. (D) Lateral radiograph obtained after initial irrigation and debridement, demonstrating temporary stabilization with an external fixator.
Fig. 3.

Autologous iliac crest bone graft. Intraoperative photograph of the harvested autologous iliac crest bone graft prepared for medial malleolus reconstruction (defect size, 2.5×2.0 cm).
Fig. 4.
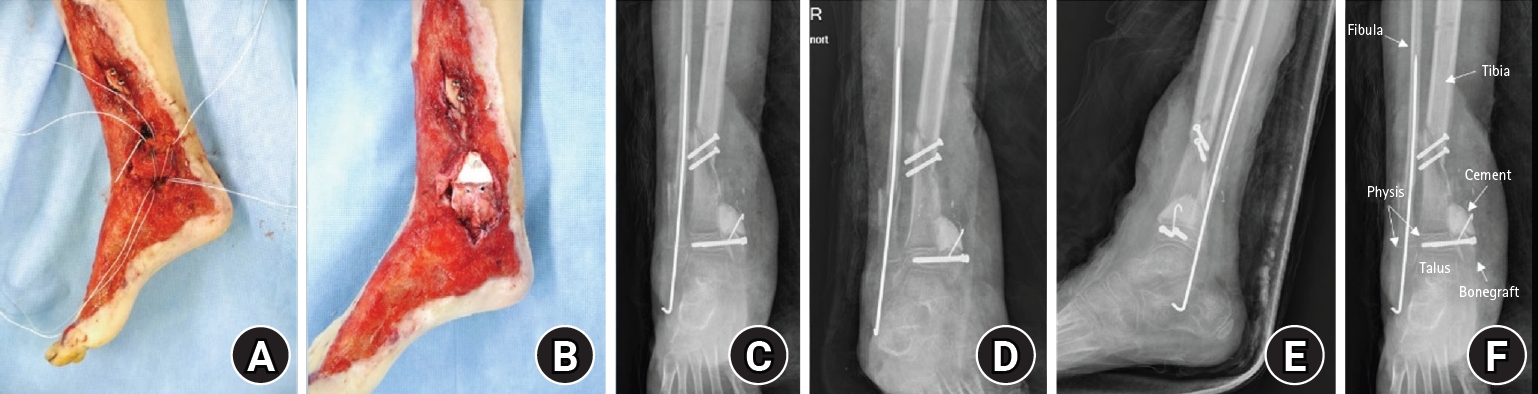
Postmedial malleolus reconstruction. (A) Medial clinical photograph obtained after reconstruction of the medial malleolus using an autologous iliac crest bone graft with internal fixation. (B) Medial clinical photograph obtained after reconstruction, showing restoration of the medial malleolar contour and soft-tissue coverage. (C) Anteroposterior postoperative radiograph demonstrating reconstruction of the medial malleolus with internal fixation. (D) Mortise postoperative radiograph demonstrating reconstruction of the medial malleolus with internal fixation. (E) Lateral postoperative radiograph demonstrating reconstruction of the medial malleolus with internal fixation. (F) Anteroposterior radiograph, showing the reconstructed medial malleolus and surrounding anatomical structures.
Fig. 5.

Soft-tissue coverage with a free anterolateral thigh flap. (A) Lateral gross photograph obtained after coverage of the medial ankle and foot defect using a free anterolateral thigh flap. (B) Anteroposterior gross photograph obtained after coverage of the medial ankle and foot defect using a free anterolateral thigh flap.
Fig. 6.

Corrective osteotomy for progressive varus deformity. (A) Preoperative anteroposterior radiograph obtained during follow-up, showing progressive varus deformity of the ankle. (B) Preoperative lateral radiograph obtained during follow-up. (C) Preoperative mortise radiograph obtained during follow-up. (D) Postoperative anteroposterior radiograph obtained after corrective osteotomy and plate fixation. (E) Postoperative lateral radiograph obtained after corrective osteotomy and plate fixation. (F) Postoperative mortise radiograph obtained after corrective osteotomy and plate fixation.
Fig. 7.
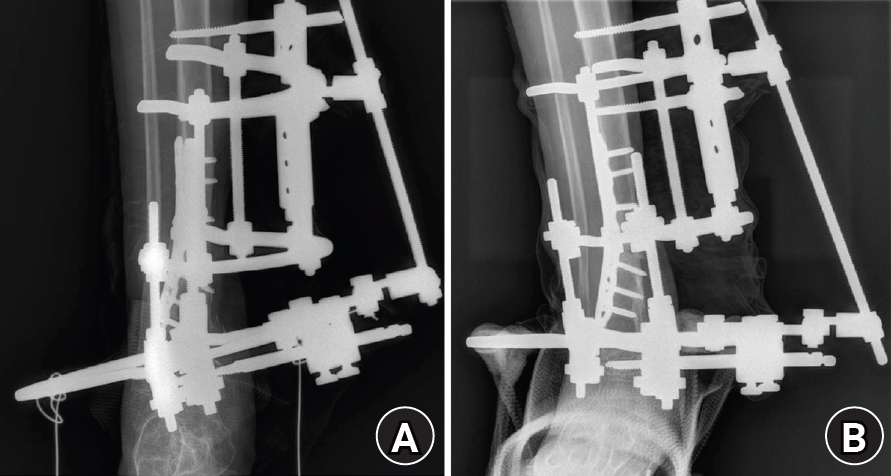
Ilizarov fixation for correction/overcorrection. (A) Anteroposterior radiograph obtained after application of an Ilizarov external fixator for deformity correction, intentional overcorrection, and alignment management. (B) Lateral radiograph obtained after application of an Ilizarov external fixator for deformity correction, intentional overcorrection, and alignment management.
Fig. 8.

Final follow-up on March 6, 2025. (A) Orthoroentgenogram radiograph obtained at the final follow-up, demonstrating maintained overall alignment. (B) Anteroposterior radiograph of the right ankle obtained at the final follow-up, showing osseous healing and maintained alignment. (C) Lateral radiograph of the right ankle obtained at the final follow-up. (D) Anteroposterior clinical photograph obtained at the final follow-up, demonstrating healed soft tissue and maintained alignment. (E) Lateral clinical photograph obtained at the final follow-up, demonstrating healed soft tissue and functional recovery.
Table 1.
Timeline of staged reconstruction and follow-up
- 1. Abbo O, Accadbled F, Laffosse JM, De Gauzy JS. Reconstruction and anticipatory Langenskiold procedure in traumatic defect of tibial medial malleolus with type 6 physeal fracture. J Pediatr Orthop B 2012;21:434-8.ArticlePubMed
- 2. Havranek P, Pesl T. Salter (Rang) type 6 physeal injury. Eur J Pediatr Surg 2010;20:174-7.ArticlePubMed
- 3. Singh V, Garg V, Parikh SN. Management of physeal fractures: a review article. Indian J Orthop 2021;55:525-38.ArticlePubMedPMCPDF
- 4. Foster BK, John B, Hasler C. Free fat interpositional graft in acute physeal injuries: the anticipatory Langenskiold procedure. J Pediatr Orthop 2000;20:282-5.PubMed
- 5. Williamson RV, Staheli LT. Partial physeal growth arrest: treatment by bridge resection and fat interposition. J Pediatr Orthop 1990;10:769-76.PubMed
- 6. Zhu C, Shi B, Rai S, Zhong H, Tang X. Case report: reconstruction of distal medial tibial epiphysis using iliac crest apophyseal autograft. Front Pediatr 2022;10:950211.ArticlePubMedPMC
- 7. Acar MA, Gulec A, Aydin BK, Erkoçak OF, Yilmaz G, Senaran H. Reconstruction of foot and ankle defects with a free anterolateral thigh flap in pediatric patients. J Reconstr Microsurg 2015;31:225-32.ArticlePubMed
- 8. Hu R, Ren YJ, Yan L, et al. A free anterolateral thigh flap and iliotibial band for reconstruction of soft tissue defects at children's feet and ankles. Injury 2015;46:2019-23.ArticlePubMed
References
Figure & Data
REFERENCES
Citations
Citations to this article as recorded by 
 ePub Link
ePub Link Cite
CiteSuccessful reconstruction and functional recovery of a pediatric medial malleolus defect in an 8-year-old girl using autologous iliac crest bone grafting in Korea: a case report

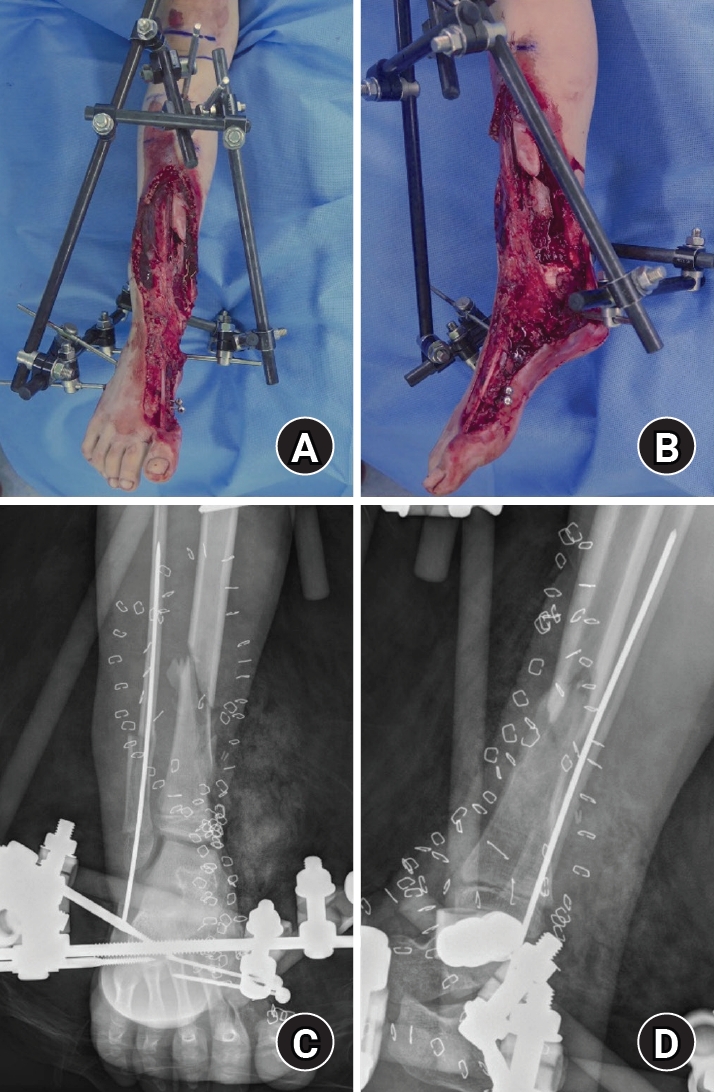

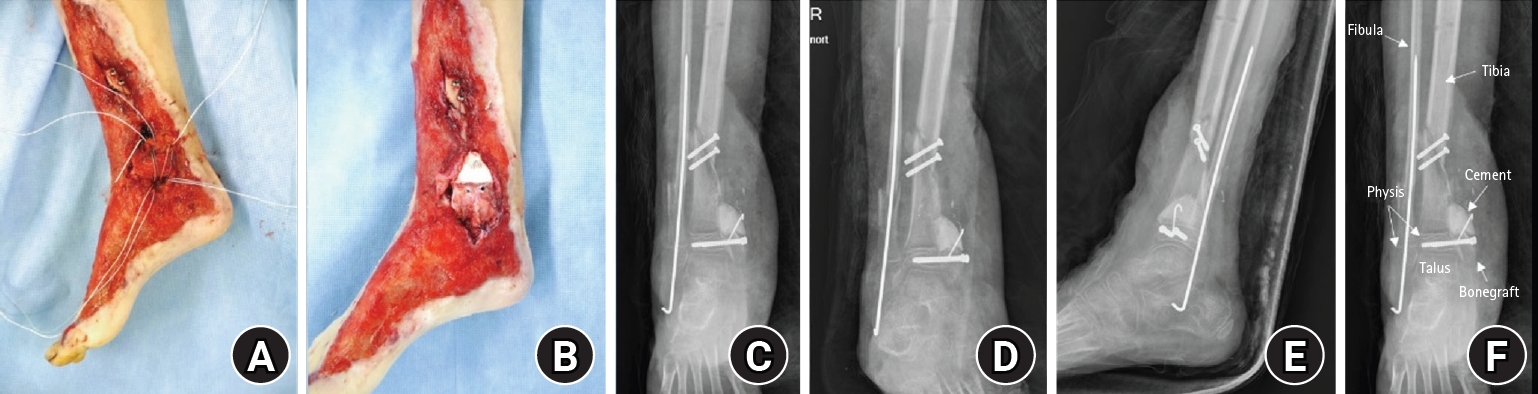
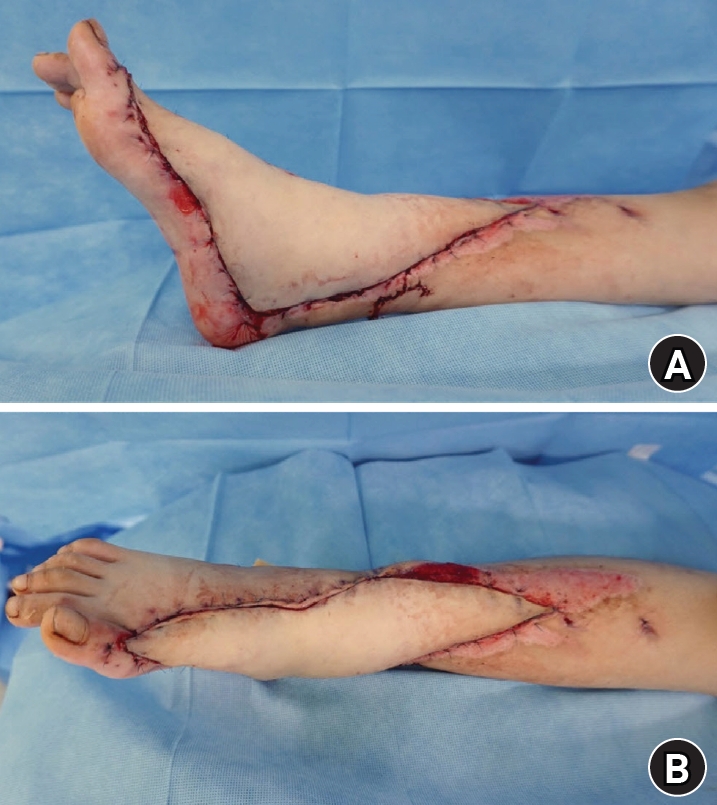

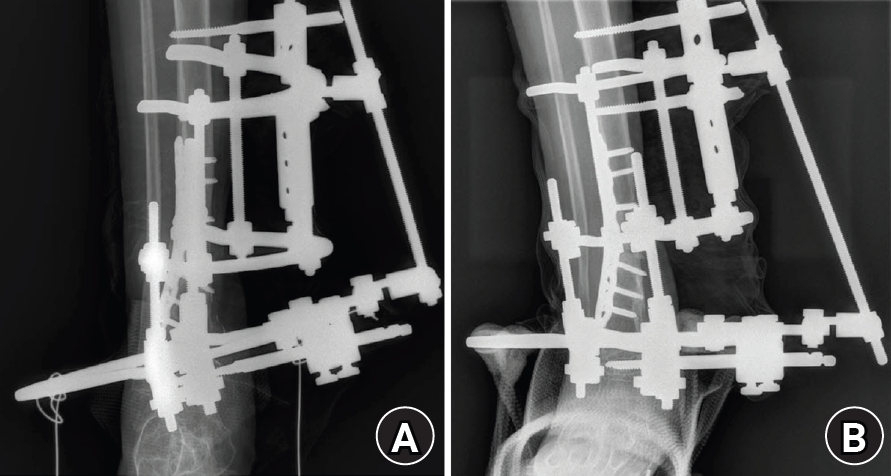

Fig. 1. Initial injury on June 14, 2016. (A) Anteroposterior gross photograph obtained at presentation showing a severe crush and degloving injury involving the medial aspect of the right ankle and foot. (B) Lateral gross photograph obtained at presentation demonstrating extensive soft-tissue loss and degloving injury of the medial right ankle and foot. (C) Anteroposterior radiograph obtained at presentation showing an associated distal tibiofibular fracture in a skeletally immature patient. (D) Lateral radiograph obtained at presentation demonstrating the distal tibiofibular fracture.
Fig. 2. Postdamage control stabilization with external fixation. (A) Anteroposterior gross photograph obtained after initial irrigation and debridement, showing temporary stabilization with an external fixator. (B) Lateral gross photograph obtained after initial irrigation and debridement, demonstrating temporary stabilization with an external fixator. (C) Anteroposterior radiograph obtained after initial irrigation and debridement, showing temporary stabilization with an external fixator. (D) Lateral radiograph obtained after initial irrigation and debridement, demonstrating temporary stabilization with an external fixator.
Fig. 3. Autologous iliac crest bone graft. Intraoperative photograph of the harvested autologous iliac crest bone graft prepared for medial malleolus reconstruction (defect size, 2.5×2.0 cm).
Fig. 4. Postmedial malleolus reconstruction. (A) Medial clinical photograph obtained after reconstruction of the medial malleolus using an autologous iliac crest bone graft with internal fixation. (B) Medial clinical photograph obtained after reconstruction, showing restoration of the medial malleolar contour and soft-tissue coverage. (C) Anteroposterior postoperative radiograph demonstrating reconstruction of the medial malleolus with internal fixation. (D) Mortise postoperative radiograph demonstrating reconstruction of the medial malleolus with internal fixation. (E) Lateral postoperative radiograph demonstrating reconstruction of the medial malleolus with internal fixation. (F) Anteroposterior radiograph, showing the reconstructed medial malleolus and surrounding anatomical structures.
Fig. 5. Soft-tissue coverage with a free anterolateral thigh flap. (A) Lateral gross photograph obtained after coverage of the medial ankle and foot defect using a free anterolateral thigh flap. (B) Anteroposterior gross photograph obtained after coverage of the medial ankle and foot defect using a free anterolateral thigh flap.
Fig. 6. Corrective osteotomy for progressive varus deformity. (A) Preoperative anteroposterior radiograph obtained during follow-up, showing progressive varus deformity of the ankle. (B) Preoperative lateral radiograph obtained during follow-up. (C) Preoperative mortise radiograph obtained during follow-up. (D) Postoperative anteroposterior radiograph obtained after corrective osteotomy and plate fixation. (E) Postoperative lateral radiograph obtained after corrective osteotomy and plate fixation. (F) Postoperative mortise radiograph obtained after corrective osteotomy and plate fixation.
Fig. 7. Ilizarov fixation for correction/overcorrection. (A) Anteroposterior radiograph obtained after application of an Ilizarov external fixator for deformity correction, intentional overcorrection, and alignment management. (B) Lateral radiograph obtained after application of an Ilizarov external fixator for deformity correction, intentional overcorrection, and alignment management.
Fig. 8. Final follow-up on March 6, 2025. (A) Orthoroentgenogram radiograph obtained at the final follow-up, demonstrating maintained overall alignment. (B) Anteroposterior radiograph of the right ankle obtained at the final follow-up, showing osseous healing and maintained alignment. (C) Lateral radiograph of the right ankle obtained at the final follow-up. (D) Anteroposterior clinical photograph obtained at the final follow-up, demonstrating healed soft tissue and maintained alignment. (E) Lateral clinical photograph obtained at the final follow-up, demonstrating healed soft tissue and functional recovery.
Fig. 1.
Fig. 2.
Fig. 3.
Fig. 4.
Fig. 5.
Fig. 6.
Fig. 7.
Fig. 8.
Successful reconstruction and functional recovery of a pediatric medial malleolus defect in an 8-year-old girl using autologous iliac crest bone grafting in Korea: a case report
| Date | Event |
|---|---|
| 2016-06-14 | Injury. Emergency I&D, temporary stabilization with external fixation, and fibular Rush pinning as indicated. |
| 2016-06 to 2016-08 | Multiple staged I&D procedures (marginal debridement) and wound management. |
| 2016-08-06 | Definitive reconstruction: medial malleolus reconstruction with a defect-matched autologous iliac crest bone graft (2.5×2.0 cm) and cannulated screw fixation; gluteal fascia used as a deltoid ligament substitute and secured with suture anchors; bone-cement spacer placed for physeal management; free ALT flap with skin graft for soft-tissue coverage. |
| 2017-01-09 | Corrective osteotomy and plate fixation for progressive varus deformity. |
| 2017-05-29 | Achilles tendon lengthening and Z-plasty for tendon/skin contracture; Ilizarov external fixation for correction/overcorrection; cement spacer removal as indicated. |
| 2025-03-06 | Final follow-up: limb-length discrepancy 5 mm; ankle dorsiflexion 0° active and 5° passive; pain-free; full activities of daily living including hiking and dancing. |
Table 1. Timeline of staged reconstruction and follow-up
I&D, irrigation and debridement; ALT, anterolateral thigh.

