 E-submission
E-submission TOTA
TOTA TOTS
TOTS
Articles
- Page Path
- HOME > J Musculoskelet Trauma > Volume 28(1); 2015 > Article
-
Original Article
- Olecranon Nonunion after Operative Treatment of Fracture
- Ho-Jung Kang, M.D., Ji-Sup Kim, M.D., Myung-Ho Shin, M.D., Il-Hyun Koh, M.D., Yun-Rak Choi, M.D.
-
Journal of the Korean Fracture Society 2015;28(1):30-37.
DOI: https://doi.org/10.12671/jkfs.2015.28.1.30
Published online: January 20, 2015
Department of Orthopedic Surgery, Yonsei University College of Medicine, Seoul, Korea.
- Address reprint requests to: Ji-Sup Kim, M.D. Department of Orthopedic Surgery, Gangnam Severance Hospital, 211 Eonju-ro, Gangnam-gu, Seoul 135-720, Korea. Tel: 82-2-2019-3412, Fax: 82-2-573-5393, kkimjsno1@naver.com
• Received: July 20, 2014 • Revised: November 27, 2014 • Accepted: December 3, 2014
Copyright © 2015 The Korean Fracture Society. All rights reserved.
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/3.0/) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
- 783 Views
- 14 Download
Abstract
-
Purpose
- Olecranon nonunion after surgical management is relatively rare, but it leads to limitation of motion of joint or instability. This retrospective study was conducted in order to analyze the cause and result of treatment.
-
Materials and Methods
- We analyzed 11 cases treated for nonunion of olecranon fractures. Nonunion was classified according to the spot of the lesion and the extent of articular surface damage. Evaluation was performed using Mayo elbow performance score (MEPS), Oxford elbow score (OES), Disabilities of the Arm, Shoulder and Hand (DASH) scores, and the range of motion.
-
Results
- According to the spot of the lesion and the extent of articular surface damage, nonunion was categorized as IA (2 cases), IIA (5 cases), and IIIA (4 cases). One case of IA underwent nonunion fragment excision and the remaining cases were treated by bone grafting. A plate was used in seven cases and the other three cases had both plate and tension band wiring fixation. All nonunions finally became union. The 11 patients with one year follow-up had average MEPS of 87.7 points (range: 60-100 points), average OES of 43.2, and average DASH score of 18.8 points. Complications included limitation of motion (2 cases) and ulnar nerve symptoms (3 cases).
-
Conclusion
- Bone grafting and fixation by plate may be beneficial. In addition, excision can be useful in type I.
- 1. Helm RH, Hornby R, Miller SW. The complications of surgical treatment of displaced fractures of the olecranon. Injury, 1987;18:48-50.Article
- 2. Horne JG, Tanzer TL. Olecranon fractures: a review of 100 cases. J Trauma, 1981;21:469-472.
- 3. Jensen CM, Olsen BB. Drawbacks of traction-absorbing wiring (TAW) in displaced fractures of the olecranon. Injury, 1986;17:174-175.Article
- 4. Macko D, Szabo RM. Complications of tension-band wiring of olecranon fractures. J Bone Joint Surg Am, 1985;67:1396-1401.Article
- 5. Murphy DF, Greene WB, Dameron TB Jr. Displaced olecranon fractures in adults. Clinical evaluation. Clin Orthop Relat Res, 1987;(224):215-223.Article
- 6. Rettig AC, Waugh TR, Evanski PM. Fracture of the olecranon: a problem of management. J Trauma, 1979;19:23-28.
- 7. Wolfgang G, Burke F, Bush D, et al. Surgical treatment of displaced olecranon fractures by tension band wiring technique. Clin Orthop Relat Res, 1987;(224):192-204.Article
- 8. Papagelopoulos PJ, Morrey BF. Treatment of nonunion of olecranon fractures. J Bone Joint Surg Br, 1994;76:627-635.ArticlePDF
- 9. Eriksson E, Sahlin O, Sandahl U. Late results of conservative and surgical treatment of fracture of the olecranon. Acta Chir Scand, 1957;113:153-166.
- 10. Veillette CJ, Steinmann SP. Olecranon fractures. Orthop Clin North Am, 2008;39:229-236.Article
- 11. Kang S, Hwang CS, Chung PH, Kim YS, Chung JW, Kim JP. Double tension band wiring for olecranon fractures. J Korean Fract Soc, 2008;21:130-134.Article
- 12. Kang HJ, Lee WY, Kim HS, Koh IH, Choi YR, Lee JJ. Fixation of olecranon fractures using plating system. J Korean Soc Surg Hand, 2012;17:29-36.
- 13. Rotini R, Antonioli D, Marinelli A, Katusić D. Surgical treatment of proximal ulna nonunion. Chir Organi Mov, 2008;91:65-70.ArticlePDF
- 14. Danziger MB, Healy WL. Operative treatment of olecranon nonunion. J Orthop Trauma, 1992;6:290-293.Article
REFERENCES

Fig. 2
(A) Lateral radiograph of a 69-year-old man after tension band wiring. (B) At 7 months after surgery, lateral radiograph shows nonunion of olecranon and pull out of tension band wiring (white arrow). (C) At 3 months after curettage and internal fixation with a reconstruction plate, radiograph shows union.

Fig. 3
(A) Lateral radiograph of a 53-year-old man shows a comminuted olecranon fracture. (B) At 7 months after surgery, lateral radiograph shows nonunion of olecranon, inadequate reduction and malposition of the proximal screw after plate fixation. (C) Osteosynthesis with plate fixation and auto-iliac bone graft. At 9 months after surgery, the patient was pain-free, had a range of motion greater than 90°.

Fig. 4
(A) Lateral radiograph of a 30-year-old man shows inadequate mechanical stability and failure of fixation with screws. (B) Osteosynthesis with plate fixation and autoiliac bone graft. (C, D) At 14 months after surgery, radiograph shows union. (E, F) Active range of motion 14 months after surgery.

Fig. 5
(A) Initial radiograph of a 46-year-old man shows a distal humerus fracture. (B) At 9 months after open reduction and internal fixation with double plating through olecranon osteotomy, radiograph shows non-union of olecranon after tension band wiring. (C) Excision of the olecranon fragment and advancement of the triceps tendon. (D) At 5 months after second surgery, active range of motion greater than 90° and painless elbow were achieved. (E, F) Active range of motion 1 year after hardware removal.



Figure & Data
REFERENCES
Citations
Citations to this article as recorded by 
 Cite
CiteOlecranon Nonunion after Operative Treatment of Fracture
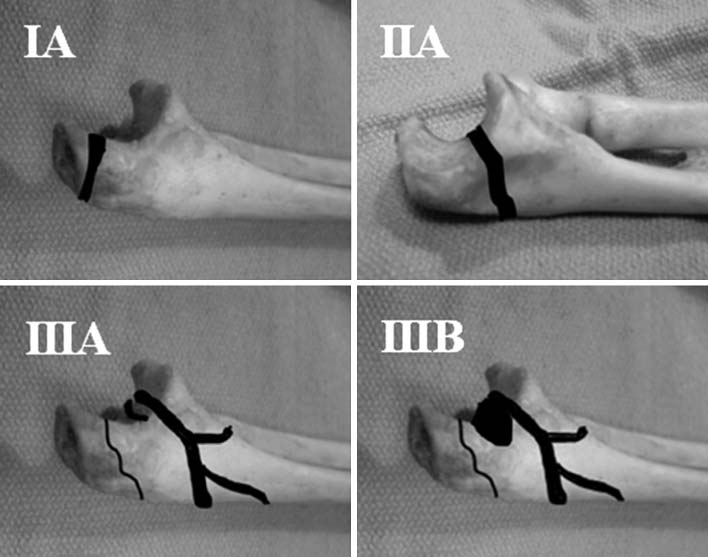




Fig. 1
Classification of olecranon nonunions.
Fig. 2
(A) Lateral radiograph of a 69-year-old man after tension band wiring. (B) At 7 months after surgery, lateral radiograph shows nonunion of olecranon and pull out of tension band wiring (white arrow). (C) At 3 months after curettage and internal fixation with a reconstruction plate, radiograph shows union.
Fig. 3
(A) Lateral radiograph of a 53-year-old man shows a comminuted olecranon fracture. (B) At 7 months after surgery, lateral radiograph shows nonunion of olecranon, inadequate reduction and malposition of the proximal screw after plate fixation. (C) Osteosynthesis with plate fixation and auto-iliac bone graft. At 9 months after surgery, the patient was pain-free, had a range of motion greater than 90°.
Fig. 4
(A) Lateral radiograph of a 30-year-old man shows inadequate mechanical stability and failure of fixation with screws. (B) Osteosynthesis with plate fixation and autoiliac bone graft. (C, D) At 14 months after surgery, radiograph shows union. (E, F) Active range of motion 14 months after surgery.
Fig. 5
(A) Initial radiograph of a 46-year-old man shows a distal humerus fracture. (B) At 9 months after open reduction and internal fixation with double plating through olecranon osteotomy, radiograph shows non-union of olecranon after tension band wiring. (C) Excision of the olecranon fragment and advancement of the triceps tendon. (D) At 5 months after second surgery, active range of motion greater than 90° and painless elbow were achieved. (E, F) Active range of motion 1 year after hardware removal.
Fig. 1
Fig. 2
Fig. 3
Fig. 4
Fig. 5
Olecranon Nonunion after Operative Treatment of Fracture
Classification of Olecranon Nonunions
Preoperative/Postoperative Series
BMD: Bone mineral density, MEPS: Mayo elbow performance score, TBW: Tension band wiring, LCP: Locking compression plate, LOM: Limitation of motion, Sx: Symptom. *Classification of olecranon nonunions.
Table 1
Classification of Olecranon Nonunions
Table 2
Preoperative/Postoperative Series
BMD: Bone mineral density, MEPS: Mayo elbow performance score, TBW: Tension band wiring, LCP: Locking compression plate, LOM: Limitation of motion, Sx: Symptom. *Classification of olecranon nonunions.

