 E-submission
E-submission TOTA
TOTA TOTS
TOTS
Search
- Page Path
- HOME > Search
Original Articles
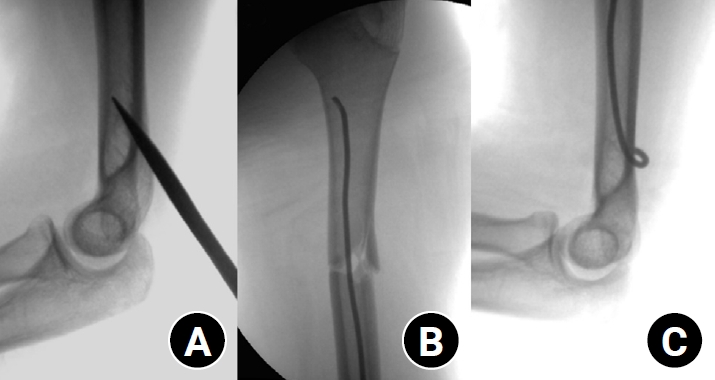
- Clinical and radiographic outcomes of elastic stable intramedullary nailing for pediatric humeral shaft fractures: a retrospective case series
- Kang-San Lee, Dongju Shin, Sang Hee Kim, Il Seo, Tae-Hoon Kim, Sung Jung Kim
- J Musculoskelet Trauma 2026;39(2):156-161. Published online March 10, 2026
- DOI: https://doi.org/10.12671/jmt.2025.00381
-
 Abstract
Abstract
 PDF
PDF - Background
Pediatric humeral shaft fractures are uncommon and are generally treated conservatively, with satisfactory clinical outcomes reported in most cases. However, conservative management often necessitates prolonged immobilization and frequent outpatient follow-up visits, and it carries an inherent risk of residual angular or translational deformity. Elastic stable intramedullary nailing (ESIN) provides a simple and minimally invasive method of fracture fixation that offers adequate stability without disrupting the periosteal blood supply, thereby permitting early mobilization and promoting rapid bone union. The purpose of this study was to evaluate the clinical and radiological outcomes of ESIN fixation in pediatric patients with humeral shaft fractures.
Methods
The medical records of pediatric patients with humeral shaft fractures who underwent ESIN fixation between January 2015 and November 2025 were retrospectively reviewed. Data collected included patient demographics, mechanism of injury, fracture location, number of elastic nails used, time to union, degree of residual angulation, range of motion (ROM), and postoperative complications.
Results
The mean age of the patients was 10.0 years (range, 7 to 15 years). The mean time to radiographic union was 5.4 weeks (range, 2.4 to 10.4 weeks). The mean coronal angulation was 0.2° (range, −9.1° to 5.8°), while the mean sagittal angulation was −1.3° (range, −6.9° to 5.3°). No cases of infection, nerve injury, or nail migration were observed during the follow-up period. At the final follow-up assessment, all patients demonstrated full shoulder and elbow ROM, with no residual deformity or pain reported.
Conclusions
In this small retrospective case series, ESIN fixation resulted in favorable union rates and excellent functional outcomes in pediatric humeral shaft fractures. Level of evidence: IV.
- 639 View
- 22 Download

- Hook plate fixation for volar plate avulsion fractures of the middle phalanges in Korea: a case series
- Kang-San Lee, Sang-Woo Son, Hee-June Kim, Hyun-Joo Lee, Dong Hee Kim
- J Musculoskelet Trauma 2026;39(1):48-53. Published online January 25, 2026
- DOI: https://doi.org/10.12671/jmt.2025.00339

-
Abstract
PDF
- Background
Volar plate avulsion fractures in phalanges are relatively common injuries. While surgical treatment can help reduce limitations in motion after injury, the small size of the fracture fragment can make the procedure challenging. In this study, we used hook plate fixation as a surgical technique for treating volar avulsion fractures in phalanges and evaluated its radiological and clinical outcomes.
Methods
The medical records of eight patients (nine digits) with volar plate avulsion fractures of the middle phalanx were retrospectively reviewed. All fractures were treated with a 1.5-mm hook plate after open reduction. Radiologic evaluations were performed using simple radiographs, and clinical outcomes were assessed through range of motion, instability, and pain.
Results
The mean follow-up period was 4.89 months (range, 1–9 months). All nine digits achieved bone union at the final follow-up. The mean union time was 2.2 months (range, 1–4 months). In all patients, the range of motion in the proximal interphalangeal joint was 85° (range, 70°–100°) before implant removal and 89.4° (range, 80°–100°) after implant removal. All patients demonstrated no joint instability and no residual pain.
Conclusion
Using a hook plate for volar plate avulsion fractures presents a promising alternative to existing fixation methods. Its biomechanical advantages and ease of fabrication make it a valuable tool in hand surgery. Level of evidence: IV.
- 1,467 View
- 41 Download
 First
First Prev
Prev

