 E-submission
E-submission TOTA
TOTA TOTS
TOTS
Search
- Page Path
- HOME > Search
Original Article
- Acute Compartment Syndrome of Thigh: Ten-Year Experiences from a Level I Trauma Center
- Hyung Keun Song, Won-Tae Cho, Wan-Sun Choi, Seung-Yeob Sakong, Sumin Im
- J Musculoskelet Trauma 2024;37(4):171-174. Published online October 25, 2024
- DOI: https://doi.org/10.12671/jmt.2024.37.4.171
-
 Abstract
Abstract
 PDF
PDF - Purpose
To assess the demographics, injury mechanisms, treatments, and outcomes of traumatic acute compartment syndrome in the thigh.
Materials and Methods
Patients diagnosed with thigh compartment syndrome were analyzed retrospectively at the authors’ level I trauma center from March 2012 to February 2022. Data were collected from medical and radiological records, focusing on demographics, injury details, treatment timelines, and clinical outcomes.
Results
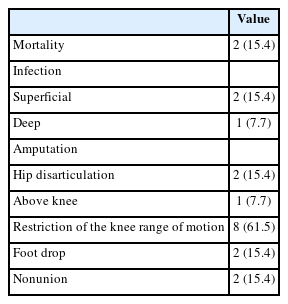
The cohort included 13 patients (11 males and 2 females) with a mean age of 46 years. Injuries primarily resulted from falls (6 patients) and vehicle accidents (5 patients). Fractures were noted in 11 patients, with seven involving the lower extremities and seven having open fractures; three of these were severe enough to be classified as Gustilo–Anderson type IIIc with associated femoral artery injuries. Time from the injury to fasciotomy ranged from within six hours to more than 24 hours. Fasciotomies were mainly single-sided (10 patients), targeting primarily the anterior compartments, and bilateral in three cases. Wound closures were performed using delayed primary closure (four patients) and partial- thickness skin grafts (five patients). Two patients died from multi-organ failure; other complications included infections (three patients), amputations (three patients), and long-term disabilities like drop foot (two patients), sensory deficits, joint stiffness (eight patients), and fracture non-unions requiring additional surgery (two patients).
Conclusion
Thigh-compartment syndrome, though infrequent, poses significant risks of mortality and chronic disability. This underscores the importance of prompt diagnosis and intervention.
- 2,096 View
- 60 Download

Review Articles
- Complications of Fracture: Acute Compartment Syndrome
- Sung Yoon Jung, Min Bom Kim
- J Korean Fract Soc 2023;36(3):103-109. Published online July 31, 2023
- DOI: https://doi.org/10.12671/jkfs.2023.36.3.103
-
Abstract
PDF
- Acute compartment syndrome occurs when the pressure in the closed bone-myofascial muscle compartment rises above a critical level, and venous perfusion through the capillaries is blocked, resulting in microcirculation disorders. Tissue ischemia in the compartment causes irreversible damage to the muscles, nerves, and even bones, and can cause functional disorders, muscle contractures, nerve damage, and nonunion. In addition to trauma, phlebitis after injection, pseudoaneurysm due to blood vessel damage, anticoagulants (e.g., warfarin), and exercise are all known causes of acute compartment syndrome. On the other hand, it commonly occurs after a fracture, leading to serious complications if not treated appropriately. Therefore, when a fracture occurs, care must be taken to determine if acute compartment syndrome has occurred, and capillary circulation must be quickly restored through early diagnosis and decompression.
- 970 View
- 29 Download
- Crush Syndrome: Traumatic Rhabdomyolysis, Reperfusion Injury
- Yong-Cheol Yoon
- J Korean Fract Soc 2023;36(2):62-68. Published online April 30, 2023
- DOI: https://doi.org/10.12671/jkfs.2023.36.2.62
-
Abstract
PDF
- A crush injury causes damage to bones, muscles, blood vessels, nerves, and other tissues caused due to pressure. Crush syndrome is a reperfusion injury that occurs throughout the body after a crush injury and leads to traumatic rhabdomyolysis, in which muscle fibers are broken down. Owing to the decreased blood supply, inflammation, and changes in metabolic activity, fluids and electrolytes in the blood can move into tissues, causing hypovolemic shock. In addition, toxic substances resulting from cell destruction can circulate through the bloodstream, causing electrolyte imbalances, renal failure, arrhythmias, and cardiac arrest, with approximately 15% of patients with acute renal failure dying. The treatment for crush syndrome involves aggressive fluid therapy and correction of the electrolyte imbalances, while patients with acute renal failure may require dialysis. Surgical treatment may include debridement and irrigation of necrotic tissue, and fasciotomy is necessary to address compartment syndrome, a complication that may arise.
- 1,575 View
- 34 Download
Original Article
- Clinical Outcomes of Fasciotomy for Acute Compartment Syndrome
- Ji Yong Park, Young Chang Kim, Ji Wan Kim
- J Korean Fract Soc 2015;28(4):223-229. Published online October 31, 2015
- DOI: https://doi.org/10.12671/jkfs.2015.28.4.223
-
Abstract
PDF
- PURPOSE
The purpose of this study is to evaluate clinical outcomes and complications after fasciotomy in acute compartment syndrome.
MATERIALS AND METHODS
Seventeen cases diagnosed as compartment syndrome and underwent fasciotomy from January 2011 to February 2015 were evaluated retrospectively. We investigated the causes and regions of acute compartment syndrome, the methods of wound management, the necessity of skin graft, and the complications including amputation and infection.
RESULTS
According to the causes of acute compartment syndrome, there were 7 fractures, 1 traumatic hematoma, 6 reperfusion injury, and 3 rhabdomyolysis. The regions of acute compartment syndrome were 3 cases of thigh, 10 cases of leg, and 3 cases of foot. One case had acute compartment syndrome involving thigh, leg, and foot. Of 17 cases, 3 cases died due to reperfusion injury and one case with severe necrosis of soft tissues underwent amputation. Among the 13 cases excluding 4 cases with death or amputation, 3 cases underwent split thickness skin graft. Shoelace technique and/or vacuum-assisted closure (VAC) was used for 9 cases, and wound closure without skin graft was achieved in all except one case, while 2 cases required skin graft among 4 cases without shoelace technique or VAC. There were 2 cases of infection.
CONCLUSION
Acute compartment syndrome caused by reperfusion injury had poor outcomes. Shoelace technique and/or VAC were useful for management of wound after fasciotomy.
- 727 View
- 6 Download
Case Reports
- Acute Compartment Syndrome of the Thigh Caused by Contusion: 4 Cases Report
- Oog Jin Shon, Gi Beom Kim, Chul Hyun Park
- J Korean Fract Soc 2012;25(3):215-218. Published online July 31, 2012
- DOI: https://doi.org/10.12671/jkfs.2012.25.3.215
-
Abstract
PDF
- Acute compartment syndrome of the thigh, which usually occurs in the anterior compartment, is a rare condition. It can have various causes including femur fractures, vessel injury, pseudoaneurysm of the femoral or popliteal artery, and use of anticoagulant. However, there have been few reports of acute compartment syndrome of the thigh without fracture caused by blunt trauma. We report 4 cases of acute compartment syndrome of the thigh without fracture caused by blunt trauma, in which three patients were treated with fasciotomy and a Vacuum-Assisted wound Closure system and the other one had a delayed diagnosis, and eventually underwent above-knee amputation.
-
Citations
Citations to this article as recorded by
- A Clinical Case Study of Residual Symptoms after Decompression of Traumatic Compartment Syndrome
Min Jung Ji, Seong Chul Lim, Jae Soo Kim, Hyun Jong Lee, Yun Kyu Lee
The Acupuncture.2015; 32(3): 197. CrossRef - Clinical Outcomes of Fasciotomy for Acute Compartment Syndrome
Ji Yong Park, Young Chang Kim, Ji Wan Kim
Journal of the Korean Fracture Society.2015; 28(4): 223. CrossRef
- A Clinical Case Study of Residual Symptoms after Decompression of Traumatic Compartment Syndrome
- 852 View
- 2 Download
- 2 Crossref
- Posterior Thigh Compartment Syndrome as a Result of Pseudoaneurysm of the Popliteal Artery in the Distal Femoral Fracture: A Case Report
- Seoung Jun Lee
- J Korean Fract Soc 2007;20(3):277-281. Published online July 31, 2007
- DOI: https://doi.org/10.12671/jkfs.2007.20.3.277
-
Abstract
PDF
- Compartment syndrome of the thigh is a rare condition and usually occurs in the anterior compartment. It is frequently caused by muscle injury, femur fracture, muscle overuse and vessel injury, but there have been few reports about posterior thigh compartment syndrome caused by pseudoaneurysm of the popliteal artery after fixation of distal femoral fracture with the retrograde intramedullary nail. We report a case of posterior thigh compartment syndrome caused by pseudoaneurysm of the popliteal artery, and report the clinical progression and result of our case.
-
Citations
Citations to this article as recorded by- Huge Pseudoaneurysm of Popliteal Artery Following Conservative Treatment of a Distal Femur Fracture: A Case Report
Won-Chul Cho, Chong Bin Park, Young-Jun Choi, Hyun-Il Lee, Hee-Jae Won, Jae-Kwang Hwang
Journal of the Korean Fracture Society.2016; 29(2): 137. CrossRef - Is CT Angiography a Reliable Tool for Diagnosis of Traumatic Vessel Injury in the Lower Extremities?
Jong-Hyuk Park, Kwang-Bok Lee, Hyuk Park, Jun-Mo Lee
Journal of the Korean Fracture Society.2012; 25(1): 26. CrossRef
- Huge Pseudoaneurysm of Popliteal Artery Following Conservative Treatment of a Distal Femur Fracture: A Case Report
- 725 View
- 0 Download
- 2 Crossref
- Spontaneous Intramuscular Hematoma associated with Acute Compartment Syndrome after Treatment of Low Molecular Weight Heparin: A Report of Two Cases
- Keun Woo Kim, Woo Dong Nam, Kee Hyung Rhyu, Byung Ryul Cho, Yong Hoon Kim, Soo Ik Awe
- J Korean Fract Soc 2006;19(1):89-92. Published online January 31, 2006
- DOI: https://doi.org/10.12671/jkfs.2006.19.1.89
-
Abstract
- Low-molecular-weight heparin (LMWH) has been considered superior to unfractionated heparin in several facets such as more effective anticoagulant, more predictable bioavailability, and less bleeding complications. We report two cases of LMWH, enoxaparin-induced spontaneous intramuscular hematoma with compartment syndrome of the lower extremity in patients with cardiac problems. The patients were treated with enoxaparin (LMWH) as bridging anticoagulation before use of warfarin due to cardiac problems. At the average 3 days of enoxaparin treatment, large and painful swelling was noticed in the lower extremities without intramuscular injection or trauma. The patients were diagnosed as having compartment syndrome with large intramuscular hematoma by CT. The patients underwent immediate fasciotomy and hematoma evacuation, and recovered without any complications.
- 786 View
- 0 Download
Original Articles
- Compartment Syndrome Complicating Avulsion Fractures of the Tibial Tubercle
- Yerl Bo Sung, Jin Hyok Kim, Hyung Jin Chung, Dong Soo Kim, Byung Hyun Jung, Jong Guk Ahn, Chil Soo Kwon, Kook Jin Chung, Bong Gyun Kang
- J Korean Soc Fract 1999;12(2):284-289. Published online April 30, 1999
- DOI: https://doi.org/10.12671/jksf.1999.12.2.284
-
Abstract
PDF
- Avulsion of the tibial tubercle is an uncommon physeal injury. Complications from this fracture have rarely been reported and seldom affect the long-term outcome. Three adolescent boys who sustained avulsion fracture of the tibial tubercle, were complicated by compartment syndrome and treated at Inje University Sang-Gye Paik Hospital from September 1989 to February 1995. Injury to the soft tissue surrounding the tibial tubercle avulsion may be more extensive than is usually appreciated. The anatomy of the proximal tibia and the tibial tubercle with nearby branches of the anterior tibial recurrent artery suggest a predisposing factor for the development of compartment syndrome. So, compartment syndrome should be added to the list of possible complications of this type of fracture.
- 474 View
- 2 Download
- Treatment of Acute Compartment Syndrome with Tibial fracture
- Young Bae Pyoi, Dong Min Shin, Pan Ok Kim
- J Korean Soc Fract 1996;9(3):614-621. Published online July 31, 1996
- DOI: https://doi.org/10.12671/jksf.1996.9.3.614
-
Abstract
PDF
- It has been known that early recognition and prompt decompression is critical in acute compartment syndrome with tibial fracture because inappropriate treatment lead to signincant functional disabilities. We treated 567 cases of tibial fracture and experienced 21 cases of acute compartment syndrome between September 1988 and June 1994. The purpose of this study is to analysis the initial degree of intracompartmental pressure and duration between the diagnosis and decompression, to evaluate the functional results and to discuss the complications. The result obtained were as follows 1. Anterior intracompartmental pressure was ranged from 25mnHg to 81mmHg (average 43.4mmHg), and deep posterior intracompartmental pressure ranged from 19mmHg to 61mmHg (average 32.7mmHg). 2. Among the 21 cases, common peroneal neuropathy were developed in 19 cases. We experienced complete recovery in 5 cases, incomplete recovery in 13 cases and 1 case of no change. We found posterior tibial neuropathy in 8 cases, and experienced complete recovery in 2 cases, incomplete recovery in 5 cases and 1 case of no change. 3. As an complications, clawing of toe developed in 3 cases, equinovarus deformity of ankle in 2 cases, superficial wound infection, osteomyelitis and nonunion in 1 case. 4. We obtained good or excellent results in 16 cases(76.1%). 5. We thought that the most important factor to decide the prognosis seems to be duration of high level of tissue pressure and also it is neccessary early diagnosis and early treatments to obtain good results.
-
Citations
Citations to this article as recorded by- Is CT Angiography a Reliable Tool for Diagnosis of Traumatic Vessel Injury in the Lower Extremities?
Jong-Hyuk Park, Kwang-Bok Lee, Hyuk Park, Jun-Mo Lee
Journal of the Korean Fracture Society.2012; 25(1): 26. CrossRef
- Is CT Angiography a Reliable Tool for Diagnosis of Traumatic Vessel Injury in the Lower Extremities?
- 732 View
- 0 Download
- 1 Crossref
 First
First Prev
Prev

