 E-submission
E-submission TOTA
TOTA TOTS
TOTS
Search
- Page Path
- HOME > Search
Original Articles
- Surgical outcomes of the coracoid process fracture associated with the acromioclavicular joint injury in Korea: a case series
- Dongju Shin, Sung Choi, Sangwoo Kim, Byung Hoon Kwack
- J Musculoskelet Trauma 2026;39(1):54-61. Published online January 14, 2026
- DOI: https://doi.org/10.12671/jmt.2025.00346
-
 Abstract
Abstract
 PDF
PDF - Background
Excluding technical reports and isolated case reports, there are no published studies evaluating coracoid process fixation with or without an acromioclavicular joint (ACJ) stabilization procedure for coracoid process fractures associated with ACJ injury. The purpose of this study was to assess the surgical outcomes of coracoid process fractures associated with ACJ injuries and to determine the usefulness of coracoid process fixation with or without an ACJ stabilization procedure.
Methods
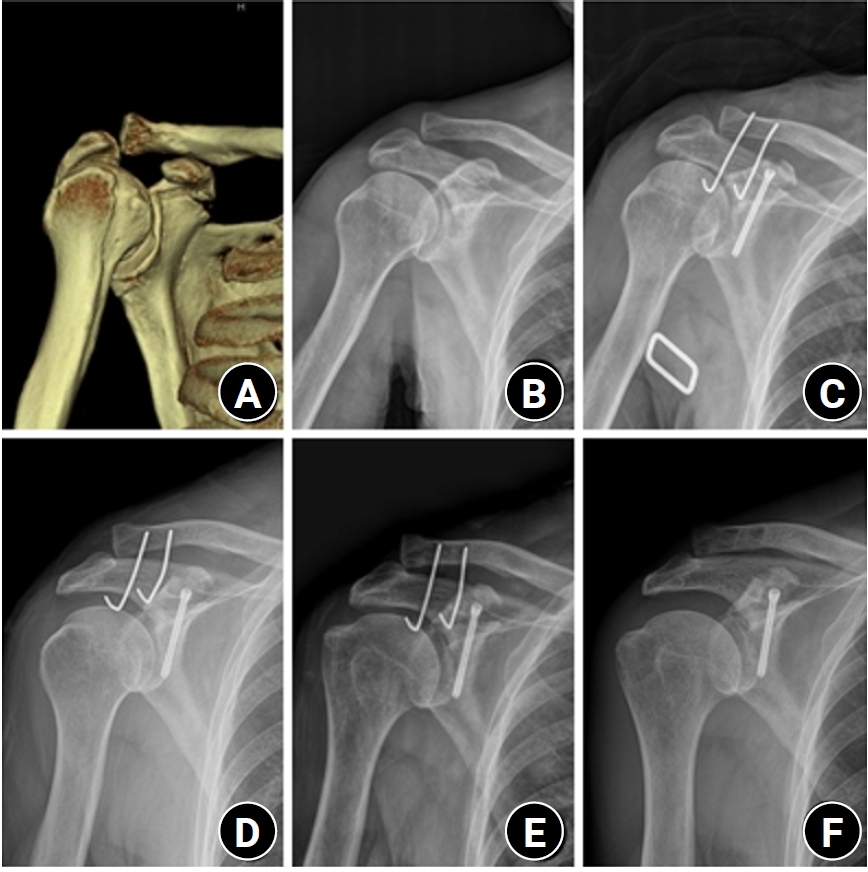
From February 2006 to December 2015, patients with coracoid process fractures associated with ACJ injuries were enrolled. Radiological and clinical outcomes were analyzed in 12 patients who underwent coracoid process fixation with or without an ACJ stabilization procedure. A 3.5-mm cannulated screw with a washer or a 3.0-mm headless compression screw was used for coracoid process fixation, and either a clavicle hook plate or Kirschner (K)-wires were used for ACJ injuries when additional fixation was necessary.
Results
Bone union was achieved in 11 patients (91.7%), while one case was determined to be a nonunion at 6 months. Radiological union occurred at an average of 3 months (range, 1.5–4 months) in all patients except the nonunion case. At the final follow-up, the average clinical scores were a visual analogue scale (VAS) pain score of 1.5 (range, 0–4) and a UCLA score of 30.9 (range, 28–35). Clinical outcomes were satisfactory in all patients, including the patient with nonunion.
Conclusion
The clinical and radiological outcomes of treating coracoid process fractures associated with ACJ injuries using coracoid process fixation with or without ACJ stabilization were favorable. A cannulated screw with a washer and clavicle hook plate fixation may provide sufficient stability for both the coracoid process fracture and the ACJ injury when feasible. Level of evidence: IV.
- 1,235 View
- 31 Download

- Outcomes of open reduction and internal fixation using 2.0/2.4 mm locking compression plate in isolated greater tuberosity fractures of humerus
- Sung Choi, Dongju Shin, Sangwoo Kim, Byung Hoon Kwack
- J Musculoskelet Trauma 2025;38(1):32-39. Published online January 24, 2025
- DOI: https://doi.org/10.12671/jmt.2025.00005
-
Abstract
PDF
- Background
The purpose of this study was to retrospectively evaluate the radiographic and clinical results of a small single or double low-profile plate fixation of 2.0/2.4 mm locking compression plate (LCP) in treating isolated greater tuberosity (GT) fractures of the humerus. Methods: From June 2015 to October 2022, patients who underwent LCP in treating isolated GT fractures of the humerus were included in this study. The radiological and clinical results were analyzed in 15 patients who underwent open reduction and internal fixation used 2.0/2.4 mm LCP. Results: Bone union was achieved in 14 patients (93.3%) and one failed case was treated with a 2.4 mm single LCP fixation. Radiological union was achieved within 10–20 weeks. Complications occurred in two patients (13.3%), including the reduction failure and shoulder stiffness. At the final follow-up, the average clinical scores were as follows: a visual analog scale for pain of 2.1 (range, 0–5) and a University of California, Los Angeles score of 27.2 (range, 18–31). Regarding range of motion (ROM), the average active ROMs were 142° for forward flexion (range, 120°–150°), 147.1° for abduction (range, 120°– 180°), and 59.3° for external rotation (range, 45°–80°). For internal rotation, the average was observed to reach the 10th thoracic vertebra (range, 1st lumbar vertebra–7th thoracic vertebra). Conclusions: The clinical and radiologic outcomes of treating isolated GT fracture using 2.0/2.4 mm LCP were favorable, and double low-profile plate fixation may be beneficial for sufficient fracture stability if possible. Level of evidence: Level IV, case series.
- 3,570 View
- 76 Download
- Assessment of Noncontiguous Posterior Malleolar Fractures in Distal One-Third Tibia Shaft Fractures with Proximal Fibula Fractures
- Dae-Geun Kim, Byung Hoon Kwack
- J Korean Fract Soc 2022;35(3):103-108. Published online July 31, 2022
- DOI: https://doi.org/10.12671/jkfs.2022.35.3.103
-
Abstract
PDF
- Purpose
Posterior malleolar fractures after intramedullary nail surgery rarely occur in distal tibia shaft fractures. The importance of preoperative ankle evaluation in preventing these fractures is also common knowledge. There are no studies in the literature on posterior malleolar fractures in distal onethird tibia shaft fractures except for distal metaphyseal tibia fractures to the best of our knowledge. The purpose of this study was to evaluate the incidence and radiological features of posterior malleolar fractures in distal one-third tibia shaft fractures with proximal fibula fractures.
Materials and Methods
Thirty-one patients diagnosed with distal one-third tibia shaft fractures with proximal fibula fractures from January 2016 to May 2021 were retrospectively reviewed. With the aid of plain radiographs and computed tomography (CT) scans, the fracture patterns of the tibia and fibula were classified according to the AO Foundation/Orthopedic Trauma Association (AO/OTA) classification, and posterior malleolar fractures were identified. The fracture pattern was classified according to the Haraguchi classification, and the angle between the bimalleolar axis and the posterior malleolar fracture line was measured when there was a posterior malleolar fracture.
Results
Out of the 31 distal one-third tibia shaft fractures with proximal fibula fractures, 16 cases (51.6%) had noncontiguous posterior malleolar fractures that were confirmed on a CT scan, while 3 cases (18.8%) were visible on initial plain radiographs. There was no statistically significant variation seen in the presence of a posterior malleolar fracture in the tibia (p=0.15) and fibula (p=0.87) fractures. According to the Haraguchi classification, there were 15 posterolateral-oblique fractures (Type I) and 1 medial-extension fracture (Type II), and the mean angle was 24.5°.
Conclusion
Noncontiguous posterior malleolar fractures occurred in approximately half of the distal one-third tibia shaft fractures with proximal fibula fractures, and a CT scan was considered necessary to diagnose posterior malleolar fractures before surgery
- 1,054 View
- 13 Download
- The Comparison of LC-DCP versus LCP Fixation in the Plate Augmentation for the Nonunion of Femur Shaft Fractures after Intramedullary Nail Fixation
- Se Dong Kim, Oog Jin Sohn, Byung Hoon Kwack
- J Korean Fract Soc 2008;21(2):117-123. Published online April 30, 2008
- DOI: https://doi.org/10.12671/jkfs.2008.21.2.117
-
Abstract
PDF
- PURPOSE
The purpose of this study was to evaluate the efficacy of the surgical treatment through the comparison of LC-DCP (Limited Contact-Dynamic Compression Plate) versus LCP (Locking Compression Plate) fixation in the plate augmentation for the nonunion of femur shaft fractures after intramedullary nail fixation.
MATERIALS AND METHODS
Twenty-four patients with the nonunion of femur shaft fractures after intramedullary nail fixation who underwent plate augmentation were evaluated from Mar. 2001 to Sept. 2005. The group with LC-DCP augmentation was done bicortical screw fixation and the group with LCP was done monocortical fixation.
RESULTS
There was one case of nail breakage in LC-DCP group, but sound bony union were achieved uneventfully in all the cases of both group. LCP fixation was slightly superior to LC-DCP fixation in view of the bony union time, operating time, postoperative Hb down, amount of postoperative transfusion, but there was no statistical difference (p>0.05). CONCLUSION: We got the satisfactory results after monocortical LCP augmentation as well as bicortical LC-DCP fixation and have concluded that monocortical LCP fixation was an effective treatment option for nonunion of femur shaft fracture occurred after Intrmedullary nail fixation. -
Citations
Citations to this article as recorded by
- Delayed Union and Nonunion: Current Concepts, Prevention, and Correction: A Review
Kristin M. Bowers, David E. Anderson
Bioengineering.2024; 11(6): 525. CrossRef - RETRACTED ARTICLE: An experimental study on stress-shielding effects of locked compression plates in fixing intact dog femur
Xinwen Zhao, Wensen Jing, Zhe Yun, Xun Tong, Zhao Li, Jiajia Yu, Yaohui Zhang, Yabin Zhang, Zhixue Wang, Yanhua Wen, Heping Cai, Jun Wang, Baoan Ma, Haien Zhao
Journal of Orthopaedic Surgery and Research.2021;[Epub] CrossRef - The Treatment of IM Nailing of Femoral Shaft Fracture: Piriformis Fossa versus Trochanteric Entry Portal
Hyun Kook Youn, Oog Jin Shon, Dong Sung Han
Journal of the Korean Fracture Society.2008; 21(3): 200. CrossRef
- Delayed Union and Nonunion: Current Concepts, Prevention, and Correction: A Review
- 2,471 View
- 23 Download
- 3 Crossref
 First
First Prev
Prev

