-
Comparative results of the femoral neck system versus the dynamic hip screw for stable femoral neck fractures in older adults in Korea: a retrospective cohort study
-
Byung-Chan Choi, Byung-Woo Min, Kyung-Jae Lee, Jun-Sik Hong
-
J Musculoskelet Trauma 2025;38(4):203-211. Published online October 24, 2025
-
DOI: https://doi.org/10.12671/jmt.2025.00276
-
-
 Abstract Abstract
 PDF PDF
- Background
This study aimed to compare the clinical and radiological outcomes of the femoral neck system (FNS) and the dynamic hip screw (DHS) for the internal fixation of stable femoral neck fractures in older adults.
Methods
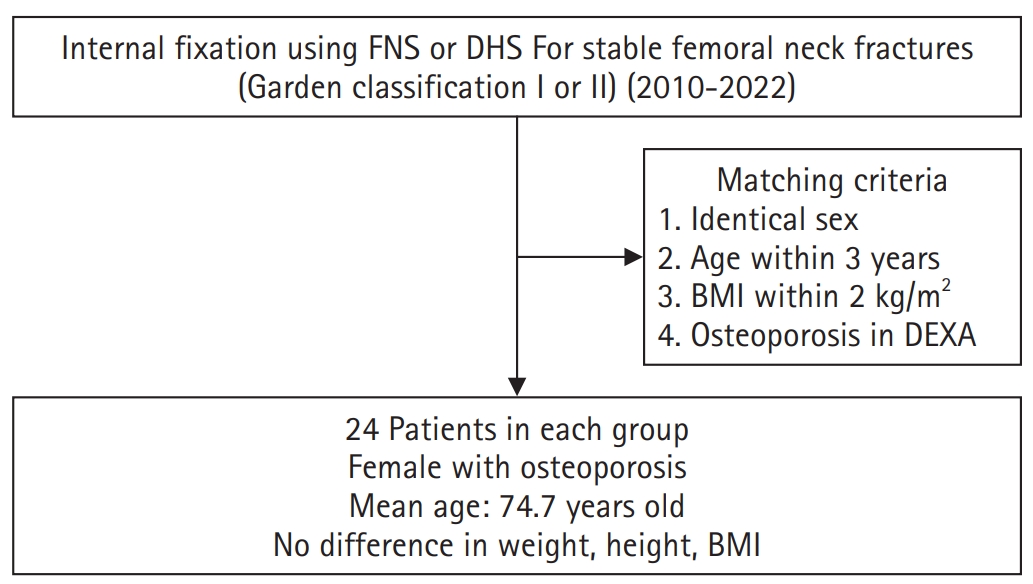
This retrospective cohort study included 48 matched older adult patients based on sex, age, BMI, and osteoporosis status, who had undergone internal fixation with either FNS or DHS for stable femoral neck fractures between January 2010 and December 2022. To minimize selection bias, a 1:1 case-control matching was performed based on sex, age, body mass index (BMI), and the presence of osteoporosis. A total of 48 patients (24 in each group) were included. We compared perioperative data (operation time, hemoglobin change, transfusion rate), functional outcomes using the Koval score, and radiological outcomes, including union rate, femoral neck shortening, and complication rates.
Results
The mean operation time was significantly shorter in the FNS group than in the DHS group (60.9 minutes vs. 70.8 minutes; P=0.007). There were no statistically significant differences between the two groups in the union rate (87.5% in FNS vs. 95.8% in DHS), femoral neck shortening, final Koval score distribution, or overall complication rates (12.5% in both groups).
Conclusions
For treating stable femoral neck fractures in older adults, the FNS demonstrated comparable clinical and radiological outcomes to the DHS, with the distinct advantage of a shorter operation time. While these findings suggest that the FNS is a promising and safe alternative that may reduce the surgical burden, definitive conclusions are precluded by the small sample size, warranting further research to corroborate these results.
Level of evidence: IV.
-
Osteoporotic Hip Fracture: How We Make Better Results?
-
Byung-Chan Choi, Kyung-Jae Lee
-
J Korean Fract Soc 2024;37(1):52-59. Published online January 31, 2024
-
DOI: https://doi.org/10.12671/jkfs.2024.37.1.52
-
-
Abstract
PDF
- The prevalence of osteoporosis and incidence of osteoporotic fractures is increasing gradually as life expectancy is prolonged and the aged population increases. Osteoporotic hip fractures (femoral neck fractures and femoral intertrochanteric fractures) have high mortality because the patients with these fractures are elderly and have several comorbidities. Thorough preparation and a multidisciplinary approach in the preoperative period are critical, and early surgery is recommended. There are also several principles to treat osteoporotic hip fractures and prevent fixation failures. Many studies have suggested various treatment methods for femoral neck fractures and femoral intertrochanteric fractures. Functional recovery treatment is essential based on the patient’s health and activity levels. Finally, aggressive management of osteoporosis and the prevention of falling is needed to treat osteoporotic hip fractures successfully.
-
Risk Factors for Subsequent Contralateral Hip Fracture following Osteoporotic Hip Fracture Surgery
-
Kyung-Jae Lee, Jung-Hoon Choi, Hee-Uk Ye, Young-Hun Kim, Kyung-Hwan Lim
-
J Korean Fract Soc 2021;34(2):51-56. Published online April 30, 2021
-
DOI: https://doi.org/10.12671/jkfs.2021.34.2.51
-
-
Abstract
PDF
- Purpose
This study examined the risk factors contributing to subsequent hip fractures in patients with osteoporotic hip fractures.
Materials and Methods
Between March 2008 and February 2016, 68 patients sustained a subsequent contralateral hip fracture after surgery for a primary osteoporotic hip fracture (Study group). The patients were compared with 475 patients who had been followed up for a minimum of one year with a unilateral osteoporotic hip fracture (Control group). The demographic data, bone mineral density (BMD), osteoporosis medication, osteoporotic fracture history, comorbid disease, type of surgery, preoperative, postoperative ambulatory capacity, and postoperative delirium in the two groups were compared.
Results
The demographic data, BMD, osteoporosis medication history, comorbid disease, type of surgery, and postoperative delirium were similar in the two groups. At three months after the primary surgery, the poor ambulatory capacity was significantly higher in the study group than the control group (p<0.001).
Conclusion
The ambulatory capacity after primary surgery is an important risk factor in the occurrence of subsequent hip fractures after osteoporotic hip fracture. Cause analysis regarding the poor ambulatory capacity after surgery will be necessary, and the development of a functional recovery program and careful management of the walking ability recovery will be needed.
-
Citations
Citations to this article as recorded by  - Osteoporotic Hip Fracture: How We Make Better Results?
Byung-Chan Choi, Kyung-Jae Lee
Journal of the Korean Fracture Society.2024; 37(1): 52. CrossRef
-
1,323
View
-
13
Download
-
1
Crossref
-
Clinical Outcomes and Radiologic Characteristics of Insufficiency Femoral Neck Fracture in Elderly Patients
-
Hee-Uk Ye, Kyung-Jae Lee, Byung-Woo Min, Kyung-Hwan Lim, Beom-Soo Kim, Young-Hoon Kim
-
J Korean Fract Soc 2021;34(1):1-7. Published online January 31, 2021
-
DOI: https://doi.org/10.12671/jkfs.2021.34.1.1
-
-
Abstract
PDF
- Purpose
In elderly patients, femoral neck insufficiency fractures that occur without a history of trauma are difficult to diagnose and treat, so it is emphasized that early suspicion of fractures and additional diagnostic tests are conducted.
Materials and Methods: Between December 2010 to December 2019, 12 femoral neck insufficiency fractures (group 1) were evaluated by comparing them with 50 traumatic femoral neck fractures of a similar age. Along with demographic data, neck cortical thickness, shaft cortical thickness, head diameter, neck width, trochanter width, shaft width, neck-shaft angle, hip axis length, femoral neck index on the simple radiographic image were compared.
Results: Seven of the 12 cases were non-displaced fractures, and it took an average of 19.2 days to diagnose the fracture after the symptoms occurred. The height was smaller than the control group at 149.1 cm in group 1 and 157.2 cm in group 2 (p<0.001). The cortical thickness of the medial femoral neck showed significant differences between the two groups: 3.16 mm in group 1 and 4.11 mm in group 2 (p=0.004). There was no statistical difference in the other measurements.
Conclusion: Femoral neck insufficiency fracture often has a delayed diagnosis because of the characteristics of the fracture. The cortical thickness of the medial femoral neck in simple radiographic images can help suspect femoral insufficiency fractures in elderly patients when considered with detailed medical history taking and a physical examination.
-
Three-Dimensional Analysis of the Morphological Features in the Femur of Atypical Fracture and Practical Implications of Intramedullary Nailing
-
Yong Uk Kwon, Kyung-Jae Lee, Joo Young Choi, Gu-Hee Jung
-
J Korean Fract Soc 2020;33(2):87-95. Published online April 30, 2020
-
DOI: https://doi.org/10.12671/jkfs.2020.33.2.87
-
-
Abstract
PDF
- Purpose
This study analyzed the morphological features of the contralateral femur without an atypical fracture by constructing a three-dimensional model with an actual size medullary canal.
Materials and Methods
Lateral and anterior bowing of the shaft were measured for 21 models, and the shape of the medullary canal was analyzed. To eliminate the projection error, the anteroposterior (AP) femur was rotated internally to the extent that the centerline of the head and neck, which is the ideal position of cephalomedullary nail screw, was neutral, and the lateral femur matched the medial and lateral condyle exactly.
Results
The lateral bowing and anterior bowing was an average of 5.5° (range, 2.8°-10.7°; standard deviation [SD], 2.4°) and 13.1° (range, 6.2°-21.4°; SD, 3.2°), respectively. In the area where lateral bowing increased, the lateral cortex became thicker, and the medullary canal was straightened. On the lateral femur, the anterior angle was increased significantly, and the diameter of curvature averaged 1,370.2 mm (range, 896-1,996 mm; SD, 249.5 mm).
Conclusion
Even if the anterolateral bowing increases in the atypical femur, the medullary canal tends to be straightened in the AP direction. So, it might be considered as a reference to the modification of an intramedullary nail to increase the conformity.
|
 E-submission
E-submission TOTA
TOTA TOTS
TOTS