Shoulder Quadruple Dislocation Fracture: Fracture of Glenoid Rim, Coracoid Process, Greater Tuberosity, Surgical Neck of Humerus Associated with Anterior Shoulder Dislocation: A Case Report
Article information

Abstract
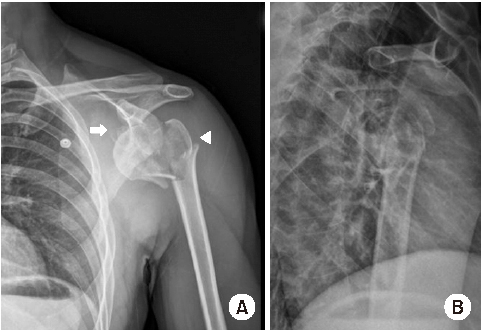
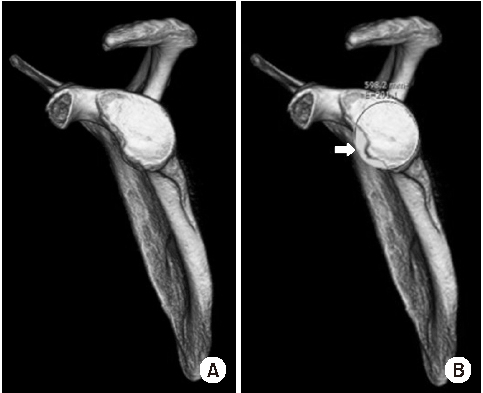
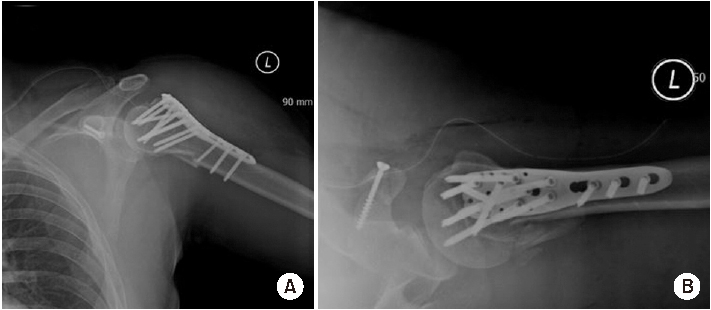
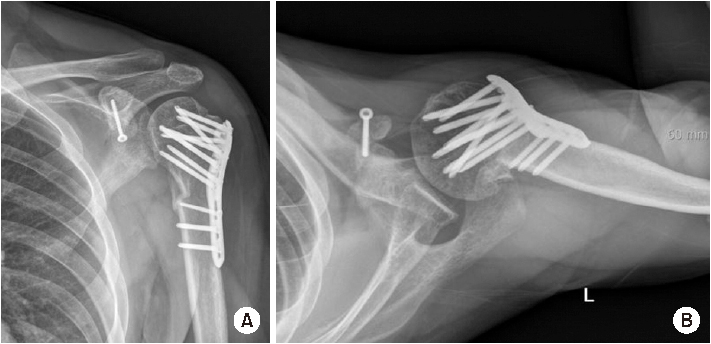
Shoulder joint dislocation has the most common incidence rate compare compared to other joints. It is reported that shoulder Shoulder dislocation couldmay be associated with glenoid rim, greater tuberosity of humerus and coracoid process fracture. There were have only been 2 cases of anterior shoulder dislocation simultaneously combined with simultaneous glenoid rim, coracoid process, and humerus greater tuberosity fracture worldwide and no report reports in Korea. We present a case of quadruple fracture (glenoid rim, coracoid process, greater tuberosity, surgical neck of humerus) associated with anterior shoulder dislocation and treated successfully by open reduction. In addition, with we provide the injury mechanism, diagnosis, treatment procedure and discussion.
Notes
None.
None.